Mitral stenosis pr notes banaao medicine subject hai hinglish mein notes banao
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Ab poore notes tayar karne ke liye kaafi content aa gaya hai. Comprehensive Hinglish notes likhta hoon:
🫀 MITRAL STENOSIS - Complete Notes (Hinglish)
Subject: Medicine | Topic: Valvular Heart Disease
1. DEFINITION
Mitral stenosis (MS) ek aise condition hai jisme mitral valve ka opening (orifice) narrow ho jata hai, jisse left atrium se left ventricle mein blood flow restricted ho jata hai.
- Normal mitral valve area: 4-5 cm²
- Symptoms tab tak nahi aate jab tak valve area 1/3 tak reduce na ho jaaye (~1.5-2 cm²)
- Severe MS: < 1.0 cm²
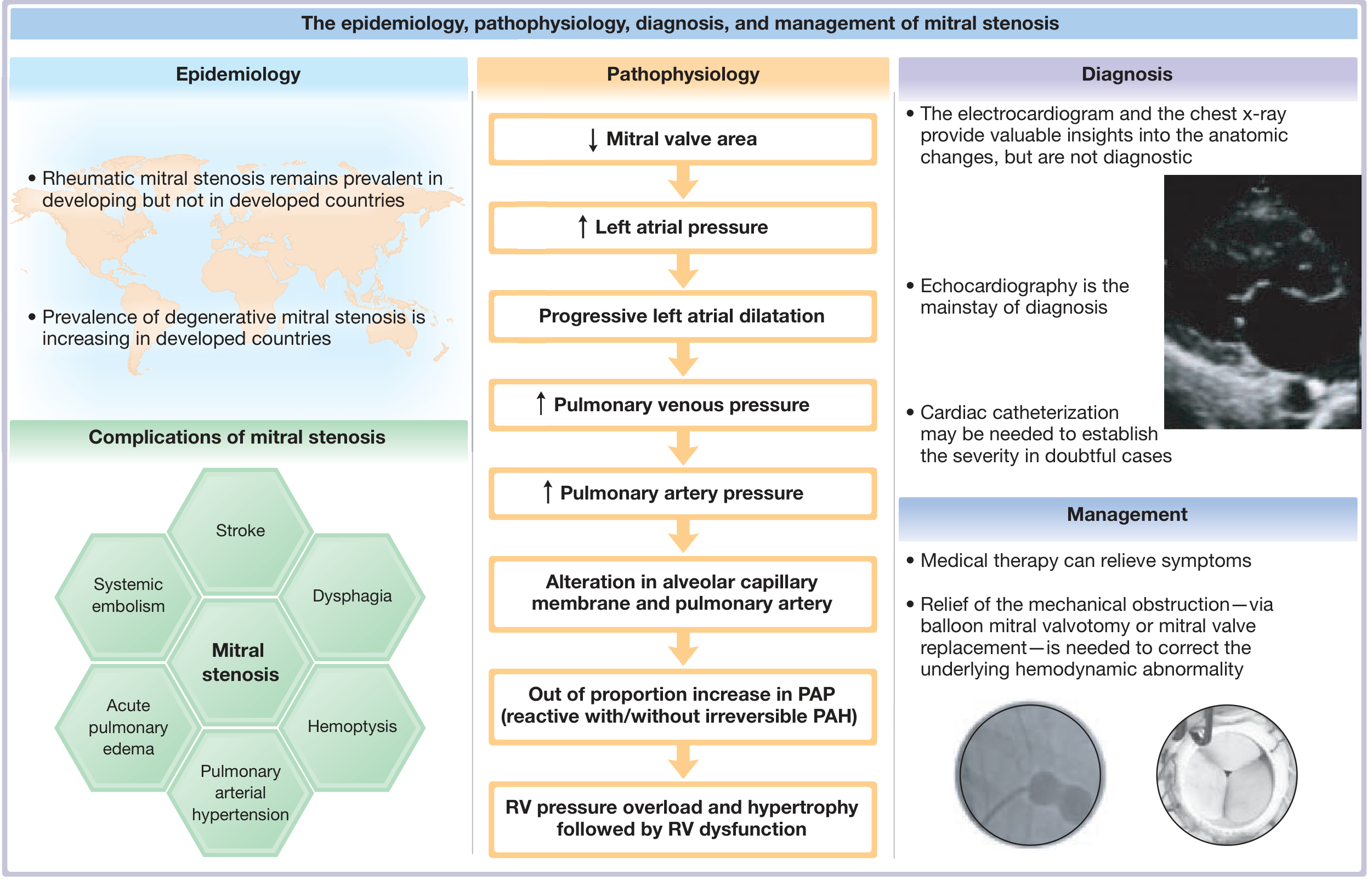
2. ETIOLOGY (Causes)
| Cause | Details |
|---|---|
| Rheumatic Heart Disease | Most common cause worldwide; especially in developing countries jaise India |
| Mitral Annular Calcification (MAC) | Developed countries mein increasingly common; elderly mein |
| Congenital | Rare |
Yaad rakho: Rheumatic disease 3 times more common in women hai, aur 40s-50s mein present hota hai.India jaise developing countries mein aaj bhi Rheumatic MS sabse common cause hai. - Goldman-Cecil Medicine
3. PATHOPHYSIOLOGY
Chain of events yaad karo - Step-by-step:
↓ Mitral Valve Area
↓
↑ Left Atrial Pressure (LA pressure ↑)
↓
Progressive Left Atrial Dilatation → Atrial Fibrillation risk ↑
↓
↑ Pulmonary Venous Pressure
↓
↑ Pulmonary Artery Pressure (PAP)
↓
Alteration in alveolar capillary membrane
↓
Out-of-proportion increase in PAP → Reactive / Irreversible PAH
↓
RV Pressure Overload → RV Hypertrophy → RV Failure
Key pathophysiology points:
- Normal diastole mein LA aur LV pressure jaldi equalize hoti hai. MS mein yeh gradient persist karta hai
- LV myocardium usually normal hota hai MS mein
- Lekin ~1/3 patients mein LV ejection fraction reduce hoti hai - reduced preload + reflex vasoconstriction ke wajah se
- Right ventricle hi transmitral gradient propel karta hai, isliye RV pe pressure overload aata hai
- Secondary pulmonary vasoconstriction hota hai jo reversible hota hai initially
4. CLASSIFICATION - Severity
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| MVA (Mitral Valve Area) | > 1.5 cm² | 1.0-1.5 cm² | < 1.0 cm² |
| Mean Gradient | < 5 mmHg | 5-10 mmHg | > 10 mmHg |
| Pulmonary Artery Pressure | < 30 mmHg | 30-50 mmHg | > 50 mmHg |
5. CLINICAL FEATURES
Symptoms (Complaints)
Cardinal symptoms - left-sided failure:
- Dyspnea on exertion (DOE) - sabse pehla aur common
- Orthopnea - lait ke sone mein takleef
- Paroxysmal Nocturnal Dyspnea (PND)
Advanced disease mein:
- Hemoptysis - bronchial veins ki anastomoses rupture hone se (left atrial pressure ↑↑ hone par). MS mein common hai, lekin other causes of LA hypertension mein uncommon!
- Ascites + Pedal edema - jab RV failure ho
- Ortner Syndrome - Large LA → Left Recurrent Laryngeal Nerve compress → Hoarseness of voice
- Dysphagia - Large LA → Esophagus compress karta hai
Trigger factors jo symptoms worsen karte hain: Atrial fibrillation, pregnancy, infection, exercise, anemia (koi bhi condition jo heart rate badhaaye ya cardiac output demand badhaaye)
6. PHYSICAL EXAMINATION
Inspection/Palpation:
- Quiet apical impulse (LV usually underfilled)
- Parasternal lift (RV heave) - jab Pulmonary Hypertension + RV hypertrophy develop ho
- "Malar flush" - butterfly rash on cheeks (low CO + vasodilation)
Auscultation - Yaad karo "S1-OS-MDM" pattern:
| Sign | Description |
|---|---|
| Loud S1 | Most prominent finding - transmitral gradient mitral valve ko pura diastole bhar open rakhta hai, phir LV systole forcefully close karta hai |
| S2 - Normal split | A2 aur P2 normal; P2 loud/loud ho jata hai jab Pulmonary HTN develop ho |
| Opening Snap (OS) | S2 ke baad aata hai - stenosed mitral valve forcefully open hota hai |
| Mid-Diastolic Murmur (MDM) | Low-pitched, rumbling, best heard at apex, with patient in left lateral decubitus position, with bell of stethoscope |
| Presystolic accentuation | Sinus rhythm mein - atrial kick se murmur increase hota hai |
| Graham Steell Murmur | Pulmonary hypertension hone par - pulmonary regurgitation ka diastolic blowing murmur |
S2-OS interval - Trick:
- S2-OS close (0.06 sec) = Left Atrial Pressure HIGH = MS SEVERE
- S2-OS wide (0.12 sec) = LA pressure relatively normal = MS MILD
S3, S4 nahi aate MS mein - kyunki obstruction at mitral valve rapid LV filling prevent karta hai!
7. INVESTIGATIONS
ECG:
- "P-mitrale" - broad, notched P wave (bifid P wave) in lead II → Left Atrial enlargement
- Atrial Fibrillation - common complication
- RVH - Right axis deviation, tall R in V1 (jab PH develop ho)
Chest X-Ray (CXR):
- Left Atrial enlargement:
- Double shadow on right heart border
- Splaying of carina (> 70°)
- Elevation of left main bronchus
- Straightening of left heart border
- Pulmonary venous hypertension:
- Upper lobe venous diversion (Kerley A lines)
- Kerley B lines (horizontal, peripheral, lower zones)
- Pulmonary edema pattern
- Hemosiderosis in lungs (chronic cases)
Echocardiography - GOLD STANDARD:
- 2D Echo: Mitral valve area (planimetry), "Hockey stick deformity" of anterior mitral leaflet
- Pressure Half Time (PHT): MVA = 220/PHT
- Mean transmitral gradient via Doppler
- Wilkins Score (for balloon valvotomy suitability):
| Feature | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Leaflet mobility | Highly mobile | Mildly restricted | Subvalvular only | Minimal movement |
| Leaflet thickening | Near normal | Midleaflet + margin | Thickening through | Marked/all |
| Calcification | Single area | Scattered margins | Extending to mid | Extensive |
| Subvalvular involvement | Minimal | Mild 1/3 | Extending to 1/3 distal | Extensive |
Wilkins Score ≤ 8 = Suitable for PTMC (Balloon Valvotomy)
Cardiac Catheterization:
- Doubtful cases mein
- Coronary angiography (> 40 years age mein before surgery)
8. COMPLICATIONS
"SAFE" mnemonic use karo:
- S - Stroke / Systemic embolism (LA thrombus → embolize)
- A - Atrial Fibrillation (most common arrhythmia)
- F - Failure (RV failure, pulmonary edema)
- E - Endocarditis (infective)
Plus:
- Hemoptysis
- Pulmonary Arterial Hypertension (PAH)
- Dysphagia / Ortner Syndrome
9. MANAGEMENT
A. PREVENTION:
- Beta-hemolytic Streptococcal infections ka antibiotic treatment karo → Rheumatic fever/MS prevent hota hai
- Penicillin prophylaxis for rheumatic fever prevention
B. MEDICAL THERAPY:
1. Asymptomatic + Sinus Rhythm:
- Koi therapy zaruri nahi
2. Mild symptoms (dyspnea, orthopnea):
- Diuretics alone
3. Atrial Fibrillation management:
| Situation | Drug |
|---|---|
| Acute AF | IV Diltiazem / Amiodarone / Esmolol (rate control) |
| Chronic AF | Beta-blocker / CCB / Oral Digoxin |
IMPORTANT: AF mein cardioversion se pehle anticoagulation karo!
4. Anticoagulation:
- MS + AF = HIGH risk for systemic embolism
- Warfarin (INR target: 2.5 to 3.5)
- Note: Rheumatic MS + AF mein DOACs (Direct Oral Anticoagulants) NAHI dete - sirf Vitamin K Antagonist (Warfarin) dena hai!
C. MECHANICAL THERAPY (Indications):
Jab symptoms ordinary activity mein aayein OR pulmonary hypertension develop ho (PAP systolic > 50 mmHg):
| Procedure | Details |
|---|---|
| PTMC (Percutaneous Transluminal Mitral Commissurotomy) = Balloon Valvotomy | Preferred if Wilkins Score ≤ 8, No significant MR, No LA thrombus |
| Open Surgical Commissurotomy | If anatomy not suitable for balloon (severe MR, calcification) |
| Mitral Valve Replacement (MVR) | Severe calcification, failed commissurotomy, combined MS + MR |
Balloon valvotomy commissurotomy karta hai (fused leaflets separate karta hai) → Valve area substantially increase hoti hai → Results comparable to surgical commissurotomy for at least a decade Even at 20 years, ~30% patients ko durable benefit milta hai.
Non-rheumatic MS (Mitral Annular Calcification wali) balloon valvotomy se NAHI khoolta - surgical debridement + MVR karni padti hai.
10. PROGNOSIS & NATURAL HISTORY
- Asymptomatic reh sakte hain decades tak
- Once symptoms develop → Rapid deterioration without intervention
- Severe symptomatic MS mein untreated patients ki survival poor hai
- PTMC/Surgical intervention se prognosis bahut improve hoti hai
11. SPECIAL SITUATIONS
MS in Pregnancy:
- Very dangerous - pregnancy mein heart rate badhti hai + blood volume badhta hai
- Both factors transmitral gradient aur LA pressure badhate hain
- PTMC pregnancy mein bhi kiya ja sakta hai (2nd trimester preferred)
- Anticoagulation management tricky hoti hai (warfarin teratogenic in 1st trimester)
MS in Elderly:
- MAC-related MS common
- AF aur systemic embolism ka risk zyada
- S1 loud nahi hoti (fibrotic valve), OS absent ho sakti hai
- PTMC success rate < 50% in elderly; complications zyada
- MVR mein perioperative mortality ≥ 10%
12. QUICK REVISION TABLE
| Feature | Mitral Stenosis |
|---|---|
| Most common cause | Rheumatic Heart Disease |
| Gender predominance | Female (3:1) |
| LV | Usually normal |
| Key auscultatory finding | Loud S1 + OS + MDM |
| Best position to hear murmur | Left lateral decubitus |
| ECG finding | P-mitrale, AF, RVH |
| Gold standard diagnosis | Echocardiography |
| Anticoagulant of choice (MS+AF) | Warfarin (NOT DOACs) |
| Mechanical intervention | PTMC if Wilkins ≤ 8 |
| Emergency in MS | Acute pulmonary edema → IV diuretics + rate control |
Sources: Goldman-Cecil Medicine (International Edition), Braunwald's Heart Disease (11th ed.), Fuster and Hurst's The Heart (15th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.