Anxiolytic and hypnotic drugs also sedatives
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have enough content for a comprehensive, well-illustrated answer. Let me compile it.
Anxiolytic, Hypnotic, and Sedative Drugs
Definitions and Concepts
These three terms describe overlapping functional categories rather than distinct drug classes:
- Sedative: reduces anxiety and exerts a calming effect with minimal CNS depression
- Anxiolytic: relieves anxiety (functionally the same as sedation at low doses)
- Hypnotic: produces drowsiness and facilitates sleep onset/maintenance (more pronounced CNS depression than sedation)
A key principle is graded, dose-dependent CNS depression - most sedative-hypnotics produce sedation at low doses, hypnosis at higher doses, and anesthesia or death at very high doses. The dose-response curve shape differs critically between drug classes:
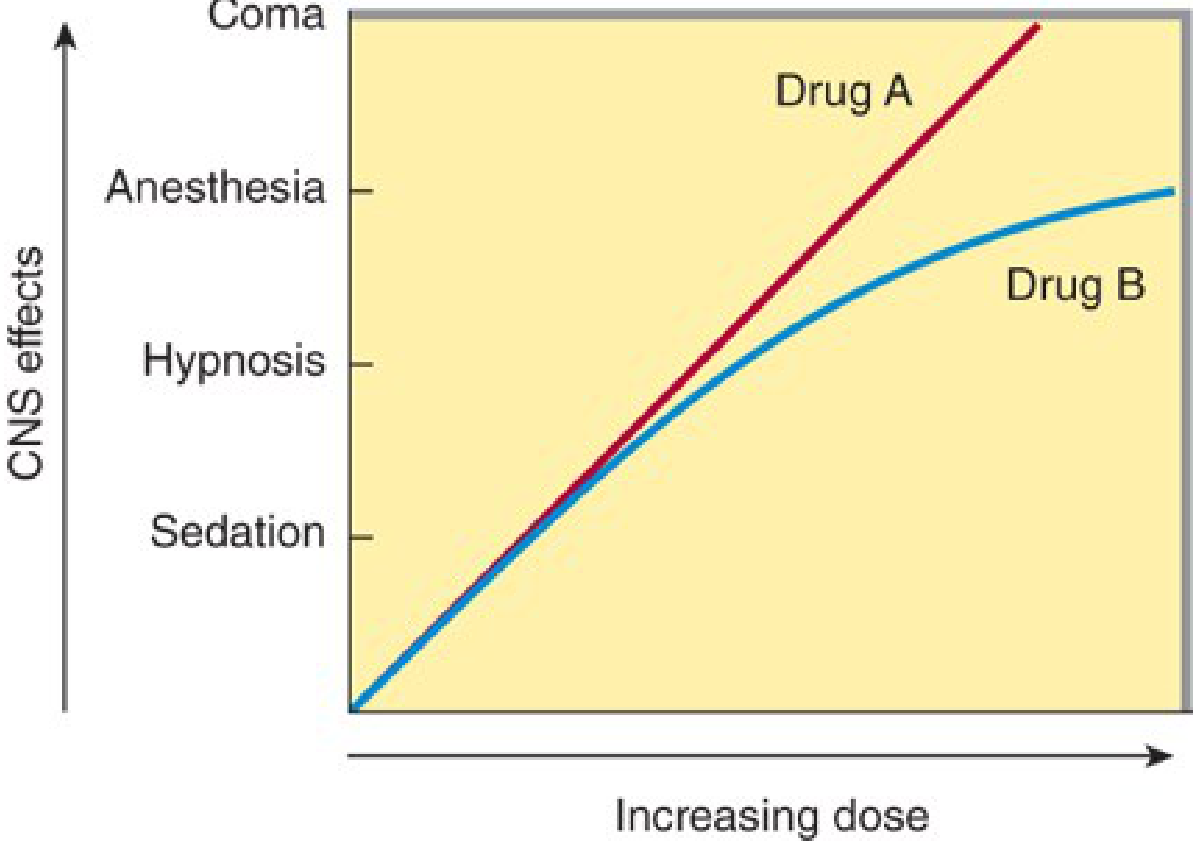
- Drug A (barbiturates, alcohols): linear response - dose increments produce proportional CNS depression, progressing to anesthesia, coma, and death
- Drug B (benzodiazepines, Z-drugs): flattened ceiling - proportionately greater dose increments are needed to reach anesthesia; much wider therapeutic index
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
Classification of Sedative-Hypnotic/Anxiolytic Drugs
1. Benzodiazepines (BZDs) - Most Widely Used
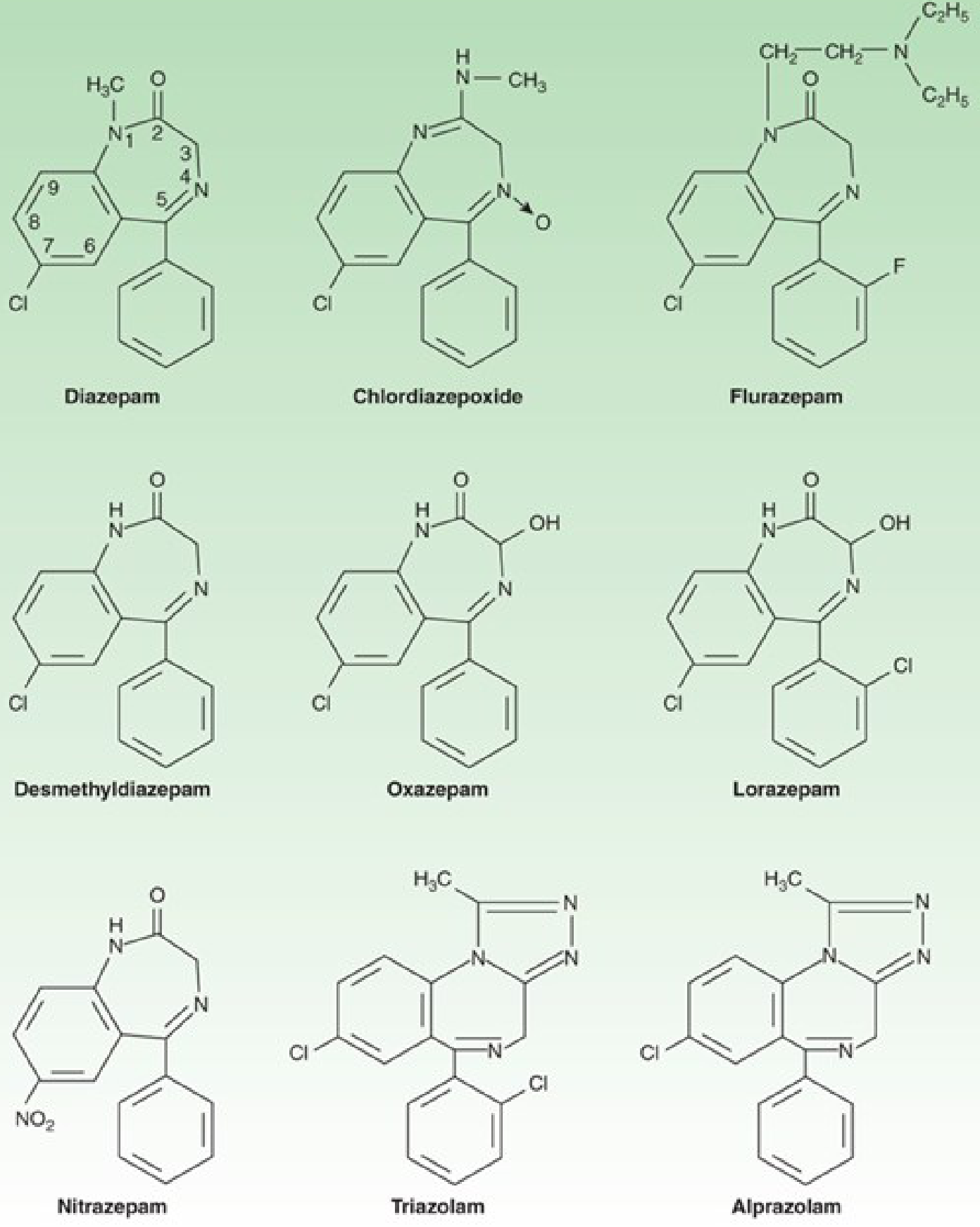
Chemical structure: 1,4-benzodiazepine ring with a carboxamide group in the seven-membered ring. A halogen or nitro group at position 7 is required for activity. Triazolam and alprazolam have an additional triazole ring at the 1,2 position.
Mechanism: Positive allosteric modulators of the GABA-A receptor. They bind to a distinct BZ site (between the alpha and gamma subunits) and increase the frequency of chloride channel opening in response to GABA. They do NOT activate the receptor directly (unlike barbiturates). This requires GABA to be present.
Classification by half-life:
| Duration | Examples | Clinical use |
|---|---|---|
| Ultra-short (<6h) | Triazolam | Sleep induction |
| Short-intermediate (6-24h) | Lorazepam, oxazepam, alprazolam, temazepam | Anxiety, pre-op sedation |
| Long (>24h) | Diazepam, chlordiazepoxide, flurazepam, clonazepam | Anxiety, seizures, alcohol withdrawal |
Important metabolic feature: Many BZDs (diazepam, chlordiazepoxide, flurazepam) are converted to desmethyldiazepam (nordazepam), an active metabolite with t½ of 36-200 hours. Oxazepam, lorazepam, and temazepam undergo direct glucuronide conjugation ("LOT" drugs) - safer in liver disease and the elderly.
Clinical Uses:
- Generalized anxiety disorder (GAD), panic disorder, social anxiety
- Insomnia (temazepam, triazolam, flurazepam)
- Seizure disorders (clonazepam, diazepam)
- Alcohol withdrawal (chlordiazepoxide, diazepam)
- Muscle relaxation (diazepam)
- Pre-operative sedation/amnesia
Adverse Effects:
- Sedation, cognitive impairment, anterograde amnesia
- Psychomotor impairment - falls, driving accidents
- CNS depression potentiated by alcohol and other depressants
- Dependence, tolerance, and withdrawal syndrome (anxiety, agitation, insomnia, tachycardia, seizures in severe cases)
- Respiratory depression (less than barbiturates; more dangerous in combination with opioids)
Tolerance and Dependence: Pharmacodynamic tolerance develops over weeks-months. Physical dependence leads to a withdrawal syndrome when stopped abruptly, which can precipitate seizures in long-term users. Tapering is required.
2. Z-Drugs (Non-Benzodiazepine Hypnotics)
- Zolpidem (imidazopyridine), Zaleplon (pyrazolopyrimidine), Eszopiclone (cyclopyrrolone - S-enantiomer of zopiclone)
Mechanism: Selective agonists at GABA-A receptors containing the alpha-1 subunit (the BZ1 subtype). This selectivity underpins relative preference for hypnotic over anxiolytic/muscle relaxant/anticonvulsant effects. They are antagonized by flumazenil.
Pharmacokinetics: Short half-lives (zaleplon ~1h, zolpidem ~2-3h, eszopiclone ~6h). Zaleplon is so short-acting it can be taken in the middle of the night. No significant active metabolites.
Advantages over BZDs: Less disruption of sleep architecture (less suppression of REM and slow-wave sleep compared to older BZDs), less daytime hangover, lower abuse potential (though not zero).
Adverse effects: Similar to BZDs but generally milder - residual sedation, complex sleep behaviors (sleepwalking, sleep-driving with zolpidem - FDA black box warning).
3. Barbiturates
Mechanism: Act at GABA-A receptors to increase the duration of chloride channel opening. At high doses, they can directly activate the chloride channel without GABA. This explains their narrow therapeutic index and danger in overdose.
Classification:
- Ultra-short: Thiopental, methohexital (IV anesthesia induction)
- Short-intermediate: Pentobarbital, secobarbital (sedation, no longer routinely used)
- Long-acting: Phenobarbital (epilepsy, febrile seizures, neonatal seizures)
Key dangers:
- Steep dose-response curve - toxic dose not far above therapeutic
- Respiratory and vasomotor center depression - cause of death in overdose
- No ceiling effect (unlike benzodiazepines)
- Induce hepatic CYP enzymes - many drug interactions
- Severe withdrawal syndrome (potentially fatal)
Modern use: Barbiturates are largely replaced by BZDs and Z-drugs for sedation/anxiety. Phenobarbital remains used for seizures; thiopental/methohexital in anesthesia.
4. Buspirone
Mechanism: Partial agonist at serotonin 5-HT1A receptors (and some D2 dopamine receptor activity). Does NOT act on GABA-A receptors. Has no cross-tolerance with BZDs.
Key features:
- Slow onset: 2-4 weeks for full anxiolytic effect (similar to antidepressants)
- No sedation, no muscle relaxation, no anticonvulsant effect
- No dependence, no withdrawal, no abuse potential
- Does not enhance CNS depression from alcohol
- Not effective for acute anxiety or panic attacks
Clinical use: Generalized anxiety disorder, especially in patients where benzodiazepine dependence is a concern, or those with a history of substance use disorders.
5. Melatonin Receptor Agonists
- Ramelteon and Tasimelteon: Agonists at MT1 and MT2 melatonin receptors in the suprachiasmatic nucleus
- Mechanism: Mimic the natural sleep-onset signal; regulate circadian rhythm
- Uses: Sleep-onset insomnia, circadian rhythm disorders (tasimelteon for non-24-hour sleep-wake disorder in the blind)
- Advantages: No abuse potential, no dependence, no withdrawal, no rebound insomnia; safe in elderly
6. Orexin Receptor Antagonists (DORAs)
- Suvorexant and Lemborexant: Dual orexin receptor antagonists (OX1R and OX2R)
- Mechanism: Block wake-promoting orexin (hypocretin) signaling, facilitating the transition to sleep
- Clinical use: Insomnia, particularly sleep-maintenance insomnia
- Advantages: New mechanism; do not suppress REM sleep; lower abuse potential than BZDs
- Adverse effects: Next-day somnolence, potential for sleep paralysis/hypnagogic hallucinations at high doses
7. Antihistamines
- Diphenhydramine, doxylamine: H1-receptor antagonists with significant CNS penetration
- Available OTC for sleep; significant hangover/anticholinergic effects; tolerance develops rapidly; not recommended for regular use, especially in the elderly (Beers criteria)
The GABA-A Receptor Complex
The GABA-A receptor is an ionotropic receptor containing alpha, beta, and gamma subunits. The chloride channel is the functional unit. Multiple drugs act here:
| Drug Class | Site | Effect on Channel |
|---|---|---|
| Benzodiazepines | BZ site (alpha-gamma interface) | ↑ frequency of opening |
| Barbiturates | Barbiturate site (beta subunit) | ↑ duration of opening |
| Z-drugs (zolpidem, zaleplon) | BZ site (alpha-1 selective) | ↑ frequency (alpha-1 selective) |
| Alcohol, propofol, etomidate | Multiple sites | Facilitate/mimic GABA |
| Picrotoxin | Channel pore | Direct channel block |
| Flumazenil | BZ site | Competitive antagonist |
Flumazenil is the specific BZ antagonist used for reversal of benzodiazepine sedation or overdose. It does NOT reverse barbiturate, meprobamate, or alcohol effects.
Pharmacokinetics Summary
Most BZDs are lipid-soluble and rapidly absorbed orally. Distribution is rapid into the CNS. Metabolism is primarily hepatic. The presence or absence of active metabolites greatly affects clinical duration.
Factors affecting BZD metabolism:
- Age (elderly: reduced hepatic metabolism, increased sensitivity)
- Liver disease (avoid drugs with active metabolites; use LOT drugs)
- Drug interactions: CYP3A4 inhibitors (e.g., ketoconazole) can significantly increase BZD levels
Clinical Issues
Tolerance and Dependence
- Sedative-hypnotics cause dispositional tolerance (increased metabolism) and pharmacodynamic tolerance (receptor downregulation/desensitization)
- Physical dependence occurs with regular use
- Cross-tolerance exists between all CNS depressants (BZDs, barbiturates, alcohol) - explains why one can substitute for another in withdrawal management
Withdrawal
- Severity depends on drug half-life: short-acting agents produce more rapid and intense withdrawal
- Symptoms: anxiety, tremor, insomnia, tachycardia, hypertension, diaphoresis
- Severe: seizures (potentially life-threatening in untreated barbiturate or BZD withdrawal)
- Management: gradual taper, often switching to a long-acting BZD (diazepam) or phenobarbital
Drug Interactions - Critical Warning
- BZDs + opioids = synergistic respiratory depression (FDA black box warning; common cause of overdose death)
- Parenteral buprenorphine + benzodiazepines = hazardous combination
- Any sedative + CNS depressant = additive/synergistic depression
Special Populations
- Elderly: increased sensitivity; LOT drugs preferred (lorazepam, oxazepam, temazepam); avoid long-acting BZDs
- Pregnancy: BZDs cross placenta; associated with neonatal withdrawal and possible cleft palate (Category D)
- Liver disease: use LOT drugs (direct glucuronidation, no active metabolites)
Summary Comparison Table
| Drug Class | Mechanism | Onset | Dependence | Key Use |
|---|---|---|---|---|
| Benzodiazepines | GABA-A BZ site (↑ frequency) | Fast | Yes | Anxiety, insomnia, seizures, withdrawal |
| Barbiturates | GABA-A (↑ duration; direct at high dose) | Fast | Yes (severe) | Anesthesia, seizures |
| Z-drugs | GABA-A alpha-1 selective | Fast | Low-moderate | Insomnia |
| Buspirone | 5-HT1A partial agonist | Slow (2-4 wk) | No | GAD |
| Ramelteon/Tasimelteon | MT1/MT2 agonist | Fast | No | Insomnia, circadian disorders |
| Suvorexant/Lemborexant | Orexin antagonist | Fast | No | Insomnia |
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed.; Goldman-Cecil Medicine, 2-Volume Set
Detailed pharmacology notes on above
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
These notes cover the full pharmacology of sedative-hypnotic and anxiolytic drugs in exam-ready depth. Here's a quick orientation to the sections:
What's covered:
- Core concepts - definitions, dose-response curve differences (the most fundamental concept)
- Benzodiazepines - chemistry, mechanism (BZ site, frequency of Cl⁻ opening), full PK table with active metabolites, LOT drugs, organ effects on sleep architecture, tolerance/dependence/withdrawal, clinical uses, flumazenil
- Barbiturates - mechanism (duration of Cl⁻ opening, direct activation at high doses), classification by duration, enzyme induction, porphyria contraindication
- Z-drugs - α1 selectivity, individual drug comparisons (zaleplon ultra-short vs. eszopiclone longer), complex sleep behaviors
- Buspirone - 5-HT1A partial agonism, 2-4 week onset, no dependence - contrasted clearly with BZDs
- Melatonin agonists - CYP1A2 and the fluvoxamine interaction
- Orexin antagonists - wake-promoting orexin system, narcolepsy connection, sleep maintenance advantage
- GABA-A receptor - master comparison table of all drugs acting at one receptor
- Tolerance/withdrawal - mechanisms and life-threatening seizure risk
- Special populations and drug interactions - practical clinical points
- Final exam summary table - all classes side-by-side
This is a shared conversation. Sign in to Orris to start your own chat.