teach me everything i nned to know about approach to azotemia ,proteinuria and hematuria
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the key content needed. Let me compile the comprehensive teaching guide.
Approach to Azotemia, Proteinuria, and Hematuria
Based on Harrison's Principles of Internal Medicine 22E, Brenner & Rector's The Kidney, and Campbell-Walsh-Wein Urology
PART 1: AZOTEMIA
What is Azotemia?
Azotemia is retention of nitrogenous waste products (urea, creatinine) in the blood due to a reduced GFR. It does not equal uremia - uremia is the symptomatic clinical syndrome that only develops when GFR falls below ~15 mL/min.
The three-tier framework for azotemia (pre-renal / intrinsic / post-renal) is the cornerstone of the approach:
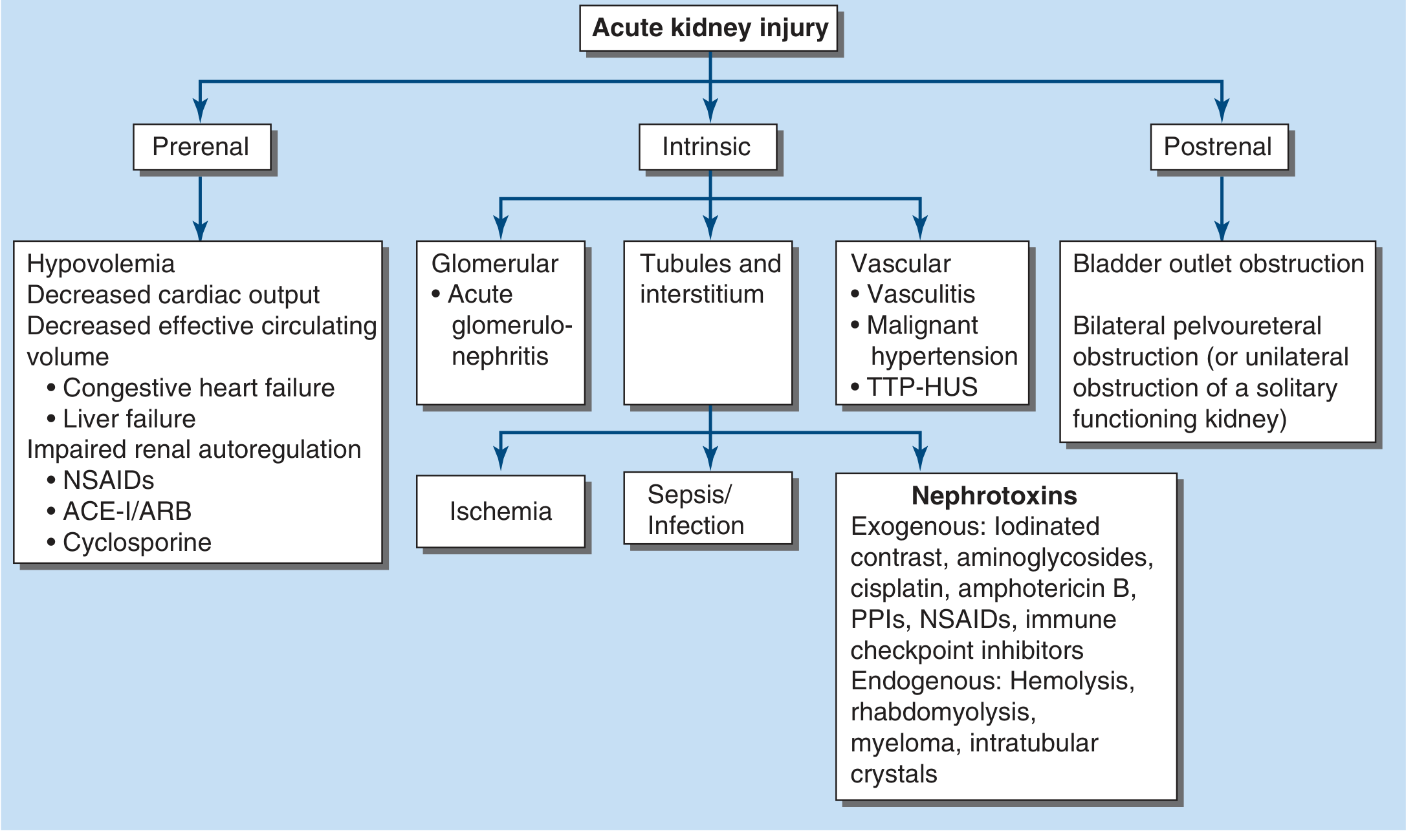
1A. PRERENAL AZOTEMIA
Definition: Reduced intraglomerular hydrostatic pressure without parenchymal damage - the most common form (~40-80% of acute kidney injury).
Causes:
- True hypovolemia: hemorrhage, burns, diarrhea, diuretics
- Volume sequestration: pancreatitis, peritonitis, rhabdomyolysis
- Decreased effective arterial volume: CHF, liver failure (hepatorenal syndrome), sepsis
- Impaired renal autoregulation: NSAIDs (block afferent prostaglandin dilation), ACE inhibitors / ARBs (block efferent angiotensin II constriction), cyclosporine
Pathophysiology:
- Reduced renal perfusion → activation of sympathetic NS + RAAS + AVP → avid Na/water retention
- GFR is maintained by two counterbalancing mechanisms: prostaglandin-mediated afferent dilation AND angiotensin II-mediated efferent constriction
- Once mean arterial pressure drops below 80 mmHg, GFR falls steeply
- Key point: Prolonged prerenal azotemia → ischemic tubular injury → ATN
Key feature: Entirely reversible once perfusion is restored. No parenchymal damage.
1B. INTRINSIC AKI (Renal Azotemia)
The most common causes are sepsis, ischemia, and nephrotoxins.
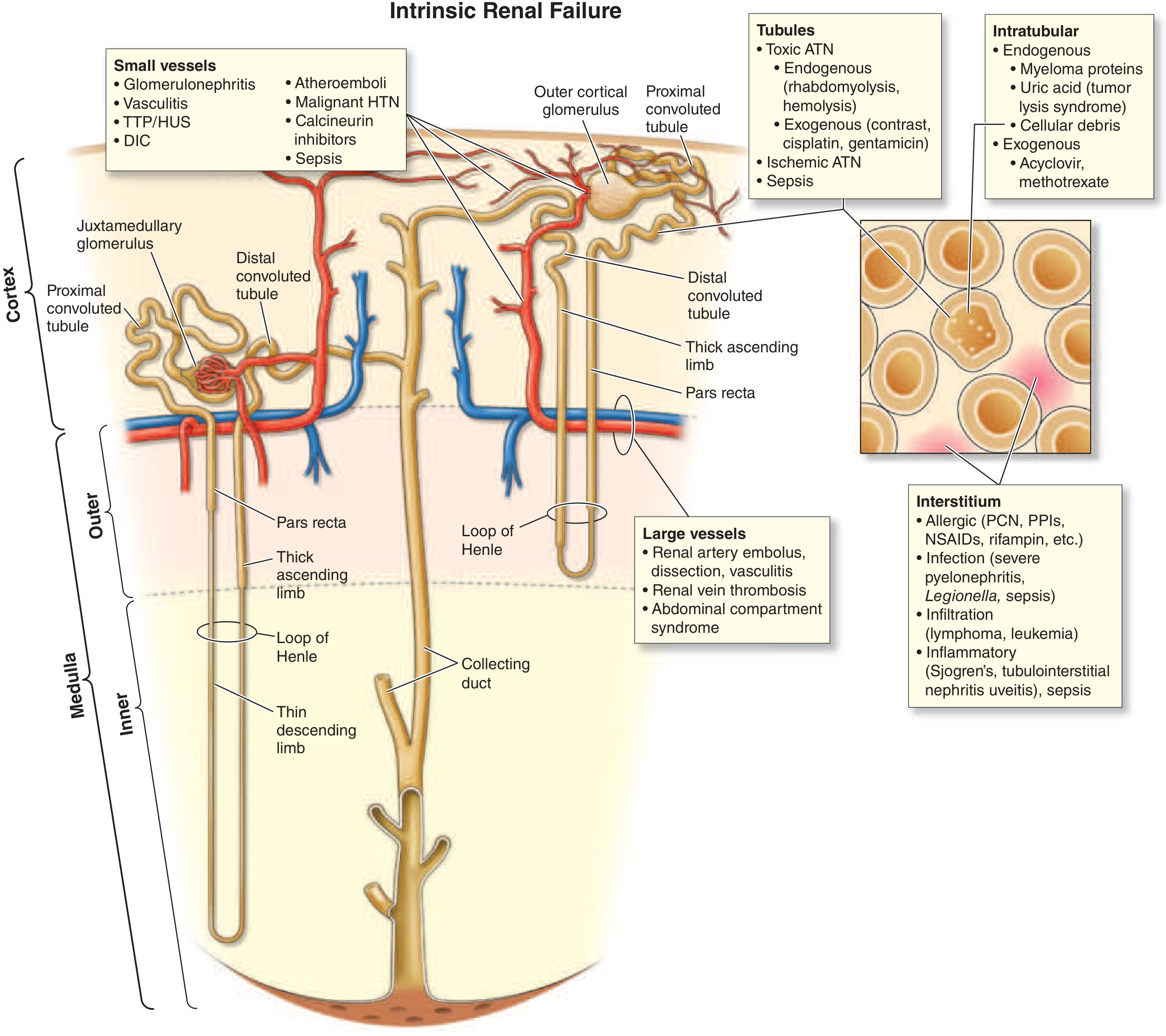
Categorized anatomically:
| Compartment | Examples |
|---|---|
| Tubules | ATN from ischemia, sepsis; toxic ATN (aminoglycosides, contrast, cisplatin, amphotericin B, PPIs) |
| Interstitium | Allergic AIN (PCN, NSAIDs, PPIs, rifampin); infection; infiltration (lymphoma, leukemia) |
| Small vessels | Glomerulonephritis, vasculitis, TTP/HUS, DIC |
| Large vessels | Renal artery embolus/dissection, renal vein thrombosis |
| Intratubular obstruction | Myeloma proteins, uric acid (tumor lysis), myoglobin, hemoglobin, acyclovir |
Sepsis-AKI (most important): AKI complicates >50% of severe sepsis cases. Mechanism involves cytokine-driven inducible NO synthase upregulation → systemic vasodilation + inappropriate renal vasoconstriction + endothelial damage + microvascular thrombosis.
1C. POSTRENAL AZOTEMIA
Requires bilateral obstruction (or unilateral obstruction of a solitary functioning kidney):
- Bladder outlet obstruction (BPH, prostate cancer, neurogenic bladder)
- Bilateral ureteral obstruction (retroperitoneal fibrosis, bilateral calculi, pelvic malignancy)
Key: Prompt decompression (catheterization, stenting) usually restores function.
1D. DIFFERENTIATING PRERENAL vs. INTRINSIC (ATN) - THE KEY TABLE
| Index | Prerenal Azotemia | Oliguric ATN |
|---|---|---|
| BUN:Creatinine ratio | >20:1 | 10-15:1 |
| Urine Na (UNa, mEq/L) | <20 | >40 |
| Urine osmolality (mOsm/L) | >500 | <350 |
| FENa | <1% (<0.5% often) | >2% |
| Urine/plasma creatinine (Ucr/Pcr) | >40 | <20 |
| Urine casts | None or hyaline/granular | Muddy-brown granular casts |
(Harrison's Principles, 22E, Table 55-2)
FENa formula:
FENa (%) = (UNa × PCr) / (PNa × UCr) × 100
Important caveats:
- FENa can be falsely low (<1%) with ATN in: contrast nephropathy, rhabdomyolysis, hemolysis, early obstruction, glomerulonephritis
- FENa is unreliable with diuretic use → use FEurea instead (FEurea <35% = prerenal; >50% = intrinsic)
1E. GFR Measurement
- Gold standard: Inulin or iothalamate clearance (rarely used clinically)
- Creatinine clearance (CrCl): 24-h urine collection; adequate if male excretes 18.5-25 mg/kg/day, female 16.5-22.4 mg/kg/day
- Cockcroft-Gault: CrCl = [(140-age) × LBW (kg)] / [PCr × 72] × 0.85 if female
- MDRD: eGFR = 186.3 × PCr^(-1.154) × age^(-0.203) × 0.742 (female) × 1.21 (Black)
- CKD-EPI: Currently most accurate for population-level use
Caveats on creatinine as a GFR marker:
- Rises acutely after eating cooked meat
- Secreted by proximal tubule (overestimates GFR in advanced CKD)
- Varies with muscle mass (misleadingly normal in elderly, cachectic patients)
PART 2: PROTEINURIA
What is Normal Protein Excretion?
- Normal: <150 mg/day total protein (<30 mg/day albumin)
- Microalbuminuria: 30-300 mg/day (or ACR 30-300 mg/g)
- Macroalbuminuria (overt): >300 mg/day
How Proteins Are Filtered
The glomerular capillary wall has two barriers:
- Size-selective barrier: Functional pores in the GBM restrict molecules >150 kDa
- Charge-selective barrier: Glycosaminoglycans repel negatively charged albumin
Additionally, the proximal tubule reabsorbs filtered albumin via a high-capacity transcytotic pathway - so even normally filtered albumin is almost entirely reclaimed.
Types / Causes of Proteinuria
| Type | Mechanism | Amount | Examples |
|---|---|---|---|
| Glomerular | Disrupted size/charge barrier | >1-3 g/day, up to >3.5 g/day | Nephrotic syndrome (MCD, FSGS, MN, DM), nephritic (GN) |
| Tubular | Failed proximal reabsorption | <1-2 g/day, low-MW proteins | ATN, Fanconi syndrome, AIN, heavy metals, tenofovir |
| Overflow | Overproduction exceeds tubular capacity | Variable | Multiple myeloma (Bence Jones), hemolysis, myoglobin |
| Functional/transient | Stress, fever, exercise, orthostatic | Usually <1 g/day | Benign; no structural disease |
Important: Dipstick detects albumin only - it will miss Bence Jones proteins (light chains). Use sulfosalicylic acid (SSA) test or urine protein electrophoresis (UPEP) when myeloma suspected.
Nephrotic vs. Nephritic Proteinuria
| Nephrotic | Nephritic | |
|---|---|---|
| Proteinuria | >3.5 g/day (massive) | <3.5 g/day (mild-moderate) |
| Hematuria | Absent or mild | Yes - dysmorphic RBCs, RBC casts |
| Edema | Severe | Mild-moderate |
| Hypertension | Variable | Yes |
| GFR | May be normal early | Reduced |
| Mechanism | Pure filtration barrier defect | Inflammatory glomerular destruction |
Why Proteinuria Matters - Prognostic Power
Proteinuria is the most powerful independent predictor of ESKD risk. Data from screening of 107,192 participants: proteinuria OR for ESKD = 14.9 (95% CI 10.9-20.2). In MRFIT (12,866 men): 2+ dipstick proteinuria raised the HR for ESKD from 2.4 → 41 in those with eGFR <60. ACR >30 mg/g is an independent predictor of ESKD, progressive CKD, and AKI.
(Brenner & Rector's The Kidney)
Quantification Methods
| Test | What it measures | Threshold |
|---|---|---|
| Dipstick | Albumin semi-quantitative (1+, 2+...) | Detects ~30 mg/dL; misses light chains |
| 24-hour urine protein | Total daily excretion | >150 mg/day = abnormal |
| Urine PCR (spot) | Protein-to-creatinine ratio | PCR >0.2 ≈ >200 mg/day |
| Urine ACR (spot) | Albumin-to-creatinine ratio | ACR >30 mg/g = microalbuminuria |
| SSA test | All proteins including light chains | Precipitates all protein |
| UPEP/UIFE | Immunofixation for M-protein | Myeloma workup |
Orthostatic (Postural) Proteinuria
A benign condition in young individuals - proteinuria appears when upright but not when recumbent. Confirmed with split 24-h collections (day vs. night). No treatment needed.
Management Principles
- ACE inhibitors / ARBs: reduce proteinuria and slow CKD progression by reducing intraglomerular pressure (efferent dilation) AND reducing podocyte injury via angiotensin II blockade + decreasing TGF-β expression
- SGLT-2 inhibitors: renoprotective in CKD with or without diabetes
- BP target: <130/80 mmHg in proteinuric CKD
- Specific treatment based on underlying cause (steroids for MCD, immunosuppression for FSGS/MN/lupus nephritis)
PART 3: HEMATURIA
Definition
- Gross hematuria: Blood visible to naked eye
- Microscopic hematuria: ≥3 RBCs/high-power field (hpf) on microscopy (adults)
- In children: >5 RBCs/hpf on at least 2 weekly samples
- Important: Dipstick alone is insufficient - myoglobin and hemoglobin also give positive dipstick. Microscopy is required for true confirmation.
Pseudohematuria
Urine appears red without true RBCs. Causes:
- Beetroot, blackberries, rhubarb (foods)
- Rifampin, phenazopyridine, phenytoin (drugs)
- Myoglobinuria, hemoglobinuria (dipstick positive, no RBCs on micro)
- Porphyria
Clinical Approach
Step 1: Localize within the urinary stream
- Initial stream hematuria → prostatic or urethral source
- Total stream hematuria → bladder or above
- Terminal hematuria → bladder neck (contracts at end of void)
- Clot shape: Vermiform (worm-like) = upper tract origin; cuboid = bladder
Step 2: Identify type
| Glomerular (Medical) | Non-glomerular (Urological) | |
|---|---|---|
| RBC morphology | Dysmorphic (acanthocytes, blebs) | Eumorphic (biconcave discs) |
| Casts | RBC casts present | Absent |
| Proteinuria | Often significant | Usually absent/minimal |
| Color | Brown / "cola-colored" | Bright red |
| Clots | Absent | May be present |
| Associated findings | HTN, edema, reduced GFR | Flank pain (stone/tumor), dysuria |
Glomerular hematuria signals: IgA nephropathy, post-infectious GN, RPGN, thin basement membrane disease, Alport syndrome.
Step 3: Risk-stratify for malignancy
Risk factors for urologic cancer in hematuria:
- Age >50 (most common cause of gross hematuria in >50 y/o = bladder cancer)
- Smoking history
- Industrial chemical/dye exposure (aniline, benzidine)
- Alkylating chemotherapy (cyclophosphamide)
- Analgesic abuse
- Chronic indwelling foreign bodies
- Gross hematuria (even single episode) in adults
Statistics: Malignancy rate in screening hematuria studies = 2.6%. Sensitivity of gross hematuria for bladder cancer = 83%; PPV = 22%.
Step 4: Workup algorithm
Hematuria confirmed by microscopy
│
├─── Exclude: UTI, menstruation, trauma, recent urologic procedure
│
├─── Glomerular features (dysmorphic RBCs, RBC casts, proteinuria)?
│ → Nephrology: serologies, renal biopsy
│
└─── No glomerular features (eumorphic RBCs, no casts)?
→ Urologic evaluation:
1. Imaging (CT urogram - gold standard for upper tract)
2. Cystoscopy (for lower tract - mandatory in adults >35)
3. Urine cytology
4. Urine culture
AUA Guidelines key points:
- All adults with asymptomatic microscopic hematuria should be evaluated
- In young women, exclude UTI first (common benign cause)
- Gross hematuria: aggressive workup regardless of suspected benign cause (e.g. stones) - always rule out concurrent malignancy
- Even after finding a "cause" (e.g. stone), follow-up urinalysis is required as hematuria can be a harbinger of serious pathology
SYNTHESIS: The Nephrologic Syndrome Framework
Harrison's teaches you to classify the findings into one of the major nephrologic syndromes using this combination:
| Syndrome | GFR | Proteinuria | Hematuria | Casts | Edema | HTN |
|---|---|---|---|---|---|---|
| Nephrotic | Normal/↓ | >3.5 g/day | Absent | Fatty, oval fat bodies | Severe | ± |
| Nephritic (AGN) | ↓↓ | Moderate | Yes, dysmorphic | RBC casts | Mild | Yes |
| RPGN | ↓↓↓ rapid | Yes | Yes | RBC casts | ± | Yes |
| AKI (prerenal) | ↓ | <1 g/day or none | None | Hyaline/granular | ± | ± |
| AKI (ATN) | ↓ | Tubular (<1 g) | Rare | Muddy-brown | ± | ± |
| AKI (AIN) | ↓ | Variable | Sterile pyuria | WBC casts | - | ± |
| CKD | ↓ progressive | Variable | Variable | Broad waxy casts | ± | Yes |
| Nephrolithiasis/obstruction | ↓ (if bilateral) | Minimal | Gross, eumorphic | None | No | No |
CLINICAL PEARLS
- BUN:Cr >20:1 with FENa <1% = prerenal until proven otherwise
- Muddy-brown granular casts = ATN signature
- RBC casts are pathognomonic of glomerulonephritis - never normal
- WBC casts = AIN or pyelonephritis
- Broad waxy casts = severe chronic kidney disease (end-stage tubules)
- Dipstick misses light chains (myeloma) - always check SSA or UPEP when suspected
- A single episode of gross hematuria in a patient >50 years needs full urologic workup
- Orthostatic proteinuria in a young person: split collections, benign if absent when recumbent
- FENa is unreliable with diuretics - use FEurea (<35% = prerenal)
- ACE inhibitors/ARBs reduce both proteinuria and progression - they are renoprotective beyond BP control
Sources: Harrison's Principles of Internal Medicine 22E (2025); Brenner and Rector's The Kidney; Campbell-Walsh-Wein Urology; Textbook of Family Medicine 9E
This is a shared conversation. Sign in to Orris to start your own chat.