hocm
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypertrophic cardiomyopathy"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have rich content from multiple authoritative sources. Let me now compile the comprehensive answer.
Hypertrophic Obstructive Cardiomyopathy (HOCM)
Definition
HOCM is a subset of hypertrophic cardiomyopathy (HCM) in which LV outflow tract (LVOT) obstruction is present. HCM itself is defined as unexplained left ventricular hypertrophy in the absence of abnormal loading conditions (valve disease, hypertension, or congenital heart defects) sufficient to account for the degree of hypertrophy. Prevalence is 0.2-0.5% worldwide, affecting all racial groups. - Goldman-Cecil Medicine, p. 494
Genetics and Pathogenesis
-
Inheritance: Autosomal dominant with variable penetrance
-
Sarcomere mutations account for ~50-60% of cases; over 1400 pathogenic variants identified
-
Most common genes:
- MYH7 (beta-myosin heavy chain) - most frequently mutated
- MYBPC3 (myosin-binding protein C)
- TNNT2 (troponin T)
- These three genes together account for 70-80% of all HCM cases
-
All are gain-of-function mutations affecting sarcomeric proteins - this enhances myofilament function, causing myocyte hypercontractility, increased energy use, and net negative energy balance
-
Contrast with dilated cardiomyopathy (DCM): same genes (e.g., beta-myosin) can be involved, but in DCM the mutations are loss-of-function
-
Robbins & Kumar Basic Pathology, p. 373-374; Goldman-Cecil Medicine, p. 496
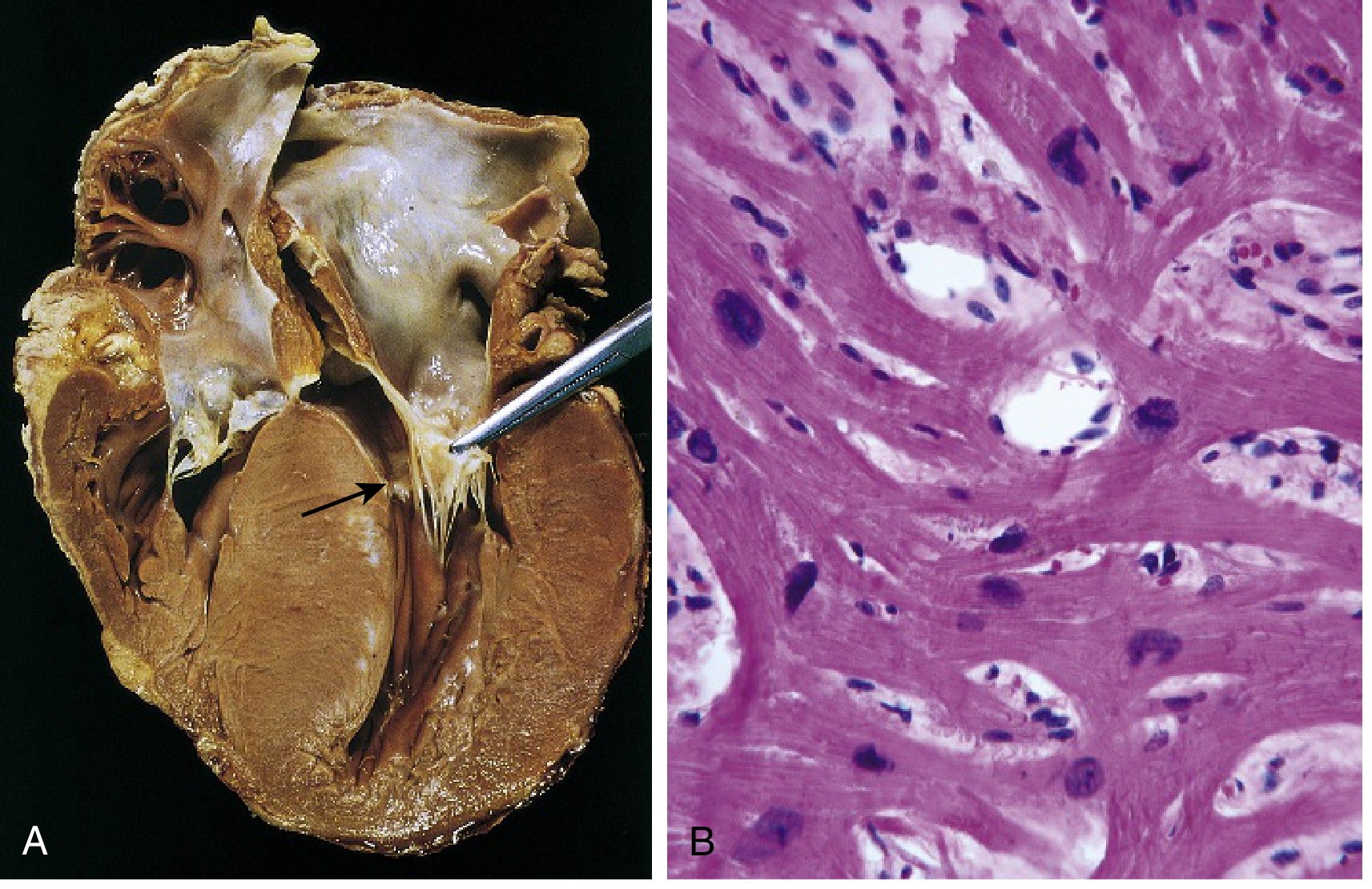
Morphology / Gross Pathology
The key gross and microscopic findings:
- Massive myocardial hypertrophy without ventricular dilation (heart is thick-walled, heavy, and hypercontractile)
- 90% show asymmetric septal hypertrophy (ASH) - disproportionate thickening of the ventricular septum vs. LV free wall
- Remaining 10% show concentric hypertrophy
- On longitudinal section: ventricular cavity takes on a "banana-like" configuration due to septal compression
- Systolic anterior motion (SAM) of the mitral valve - the anterior mitral leaflet contacts the septum during systole, creating a fibrous endocardial plaque in the LVOT
- Left atrium is enlarged
Histological triad:
- Marked myocyte hypertrophy
- Myocyte (and myofiber) disarray (haphazard arrangement)
- Interstitial fibrosis
- Robbins & Kumar Basic Pathology, p. 373-374
Pathophysiology
The obstruction is dynamic, not fixed. Two main mechanisms impair cardiac output:
| Mechanism | Effect |
|---|---|
| Diastolic dysfunction | Myocardium doesn't fully relax after systole → impaired LV filling |
| LVOT obstruction (SAM of mitral valve) | Dynamic obstruction during systole → reduced effective stroke volume |
Combined effect:
- Reduced cardiac output
- Elevated pulmonary venous pressure
- Secondary mitral regurgitation (from SAM)
- Myocardial ischemia even without CAD (massive hypertrophy + high LV pressures + compromised intramural arterial blood flow)
Clinical Features
Typically manifests during the postpubertal growth spurt, but can present at any age.
Symptoms:
- Exertional dyspnea (most common)
- Angina (ischemia without obstructive CAD)
- Syncope / pre-syncope (often exertional)
- Palpitations
Cardinal sign: Harsh systolic ejection murmur at the LLSB/apex
Murmur behavior (dynamic obstruction):
| Maneuver | Effect on murmur | Mechanism |
|---|---|---|
| Valsalva (straining phase) / standing | ↑ murmur | Decreased preload → more obstruction |
| Squatting / passive leg raise | ↓ murmur | Increased preload → less obstruction |
| Exercise | ↑ murmur | Increased inotropy + decreased afterload |
Major Complications
- Sudden cardiac death (SCD) - HCM is the leading cause of SCD in athletes under 35 years old (responsible for ~1/3 of cases)
- Atrial fibrillation with mural thrombus formation and thromboembolic stroke
- Ventricular fibrillation
- Infective endocarditis of the mitral valve
- Congestive heart failure (late)
- 4-6% incidence of sudden death in children and adolescents specifically
- Robbins & Kumar, p. 374; Harriet Lane Handbook, p. 248
Drugs That Worsen HOCM (Contraindicated / Use with Caution)
HOCM is a preload-dependent lesion. These agents worsen LVOT obstruction:
| Drug Class | Mechanism of Harm |
|---|---|
| Diuretics | Volume depletion → decreased preload |
| Vasodilators (nitrates, ACE inhibitors) | Decreased preload and afterload |
| Positive inotropes (digoxin, dopamine) | Increased contractility → decreased LV end-diastolic volume |
| Tachycardia (e.g., from atropine, dehydration) | Less filling time → worsened obstruction |
- Frameworks for Internal Medicine, p. 319
Diagnosis
- Echo (cornerstone): Asymmetric septal hypertrophy (septal/posterior wall ratio >1.3-1.5), SAM of the mitral valve, LVOT gradient (resting ≥30 mmHg, or provoked ≥50 mmHg = significant obstruction)
- ECG: LV hypertrophy, deep Q waves (especially inferior and lateral leads), ST/T changes
- Genetic testing: Recommended when a diagnostic phenotype is present; valuable for cascade screening of family members
- Cardiac MRI: Detects fibrosis (late gadolinium enhancement) - marker of SCD risk
Management
Medical (mainstay)
- Beta-blockers (first-line) - reduce heart rate, decrease inotropy, improve diastolic filling
- Calcium channel blockers (verapamil or diltiazem) - negative inotropes; alternative to beta-blockers
- Disopyramide - negative inotrope + antiarrhythmic; often combined with a beta-blocker for LVOT obstruction
- Mavacamten (myosin inhibitor) - novel agent; reduces LVOT obstruction; first-in-class cardiac myosin inhibitor
- Avoid: diuretics, vasodilators, digoxin, inotropes
Rate/Rhythm Control for AF in HCM
- Preferred: disopyramide + beta-blocker, OR verapamil/diltiazem for rate control, OR amiodarone alone
- Anticoagulation for AF (stroke prevention)
Invasive / Procedural
- Septal myectomy (Morrow procedure) - surgical resection of the hypertrophied septum; gold standard for drug-refractory symptomatic LVOT obstruction
- Alcohol septal ablation - catheter-based injection of alcohol into the first septal perforator → controlled septal infarction; reduces obstruction; used in surgical candidates and pre-transplant HOCM patients
- ICD (implantable cardioverter-defibrillator) - for SCD prevention in high-risk patients
Lifestyle
- Moderate restriction of physical activity (avoid competitive sports)
- Maintain adequate hydration (preload protection)
Pediatric-Specific
-
Negative inotropes (beta-blocker or CCB) for symptom control
-
ICD if at increased risk for SCD
-
Myectomy if symptomatic with subaortic obstruction
-
Harriet Lane Handbook, p. 248; Goldman-Cecil Medicine; Robbins & Kumar, p. 374
Key Distinguishing Features vs. Other Cardiomyopathies
| Feature | HCM/HOCM | DCM | RCM |
|---|---|---|---|
| Wall thickness | Increased | Normal/thin | Normal (may increase) |
| Cavity size | Small | Dilated | Normal/small |
| Systolic function | Normal/hyperdynamic | Reduced | Normal |
| Diastolic function | Impaired (stiff) | Impaired | Severely impaired (stiff) |
| Genetics | Gain-of-function sarcomere | Loss-of-function sarcomere | Variable |
Summary: HOCM is the obstructive form of HCM, caused by gain-of-function sarcomere mutations, characterized by asymmetric septal hypertrophy + dynamic LVOT obstruction from SAM of the mitral valve. Management hinges on negative inotropes, avoidance of preload-reducing agents, and septal reduction procedures for refractory cases. It is the leading cause of sudden cardiac death in young athletes.
This is a shared conversation. Sign in to Orris to start your own chat.