Latissimus dorsi flap surgery
Reading File
Finding Sources
Finding Sources
Searching PubMed
"latissimus dorsi" AND "flap reconstruction"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Now I have all the information needed for a thorough, well-cited response.
Latissimus Dorsi Flap Surgery
Overview
The latissimus dorsi (LD) flap is one of the most versatile and reliable flaps in reconstructive surgery. It can be used as a pedicled or free (microvascular) flap, transferred as muscle only, myocutaneous (muscle + skin paddle), or as part of a composite "chimeric/superflap" incorporating adjacent tissue from the scapular system. The muscle is classified as a Type V muscle (one dominant pedicle + multiple secondary segmental pedicles), giving it a highly predictable blood supply.
Vascular Anatomy
The entire LD flap system is based on the subscapular artery axis:
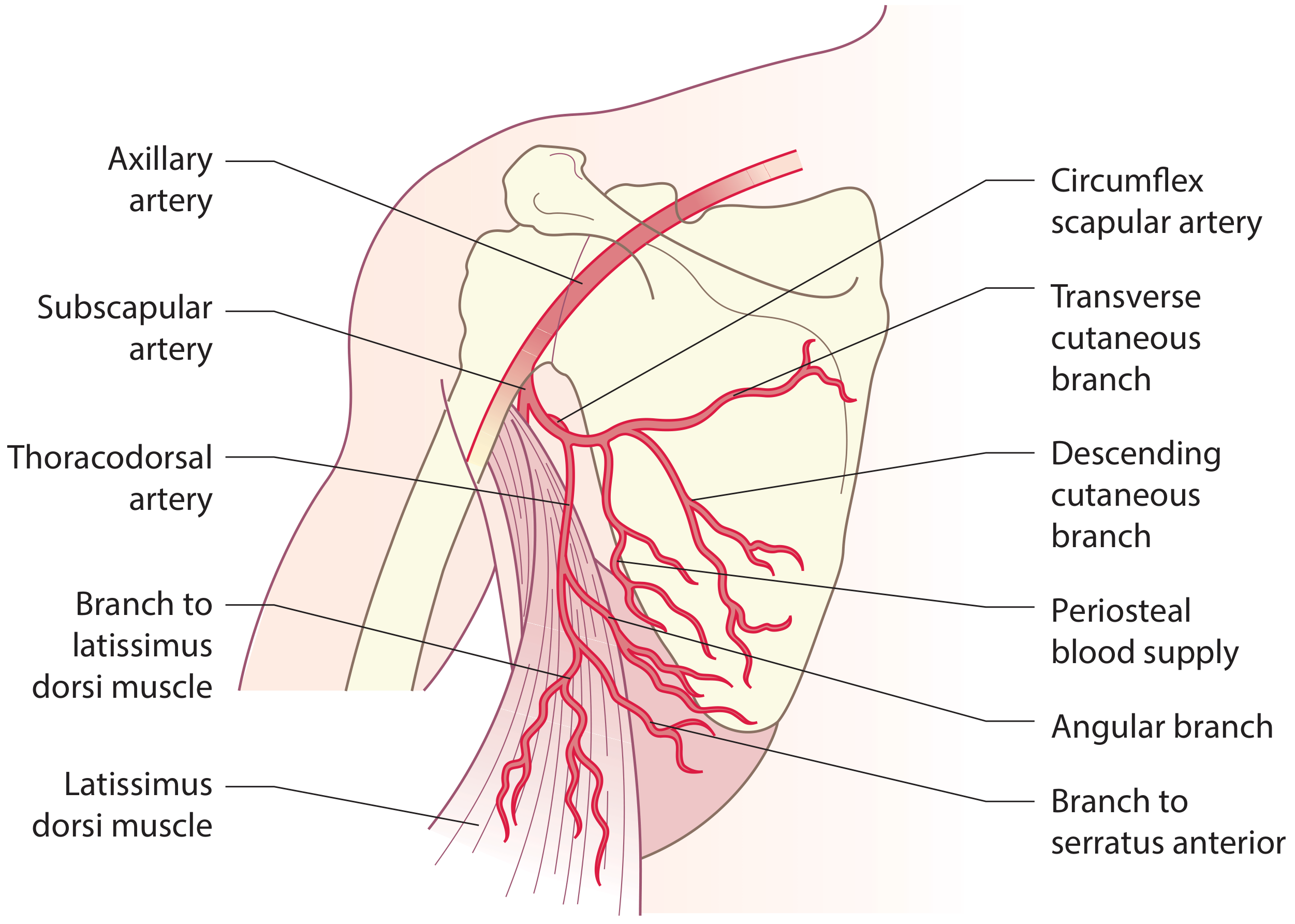
- Axillary artery → Subscapular artery → divides into:
- Circumflex scapular artery - supplies the scapula and overlying skin (scapular/parascapular flaps)
- Thoracodorsal artery - the dominant pedicle of the LD muscle; also gives off:
- A branch to the serratus anterior
- The angular artery (to the scapular tip)
- A descending cutaneous branch and a transverse cutaneous branch to the overlying skin
- Venous drainage is via paired venae comitantes joining the axillary vein near the subscapular artery origin
- Pedicle length: long (can be extended to the subscapular artery), vessel caliber is large, making microvascular anastomosis relatively straightforward
The thoracodorsal artery being a branch of the subscapular artery means the LD can be harvested as part of a "superflap" based on the subscapular artery, incorporating scapular, parascapular, and serratus anterior flaps all on a single vascular pedicle - a unique advantage of this system. Defect coverage of up to 1,050 cm² has been described with a chimeric LD + serratus anterior flap.
- Scott-Brown's Otorhinolaryngology, p.1348; Rockwood & Green's Fractures, p.752
Forms of the Flap
| Form | Contents | Notes |
|---|---|---|
| Muscle-only flap | LD muscle alone | Covered with split-skin graft; good for filling deep defects |
| Myocutaneous flap | Muscle + skin paddle (up to 20 × 40 cm) | Skin paddle serves as monitor of flap perfusion |
| Thoracodorsal artery perforator (TDAP) flap | Skin/fat only, muscle spared | Reduces donor-site morbidity |
| Chimeric/superflap | LD + serratus anterior ± scapular bone | Single pedicle; for massive defects |
Surgical Technique
Patient Positioning
- Lateral decubitus position (most commonly)
- This is a key limitation as it can complicate synchronous (two-team) surgery
Flap Design
- The skin paddle is designed along the anterior inferior portion of the muscle
- For pedicled myocutaneous rotation flaps to the head/neck: oblique or vertical orientation
- For free flaps or breast reconstruction: horizontal orientation below the scapular tip - scar concealed in the bra line
Step-by-Step Elevation (Scott-Brown's Otorhinolaryngology, p.1338)
- Outline the flap on the skin
- Initial incision to expose the anterior edge of the LD muscle
- Dissect inferiorly, cutting through muscle
- Identify the serratus anterior (its fibres run at right angles to LD fibres) - do not go deep to it here, as this places the pedicle in jeopardy
- Divide LD inferiorly; the muscle flap may be extended beyond the skin island in any direction for additional bulk
- Elevate the flap in the submuscular plane
- Identify the pedicle running down the muscle centrally - key tip: identify the branches to serratus anterior and follow them superiorly to find the thoracodorsal take-off
- Divide vessels to serratus anterior, continue dissecting superiorly toward the scapular tip
- The junction of thoracodorsal vessels with the circumflex scapular vessels forming the subscapular artery is visible at the upper anterior end of the muscle in the axilla
- For a longer pedicle: ligate the circumflex scapular vessels and follow subscapular vessels into the axilla
- Island the flap by dividing the muscle insertion into the humerus (required for free transfer or when extended pedicle length is needed)
Note: When using as a pedicled rotation flap, consider leaving the humeral insertion intact - this prevents pedicle twisting and reduces the risk of venous congestion.
Clinical Applications
1. Breast Reconstruction (most common pedicled use)
- Raised on thoracodorsal vessels; tunneled to the anterior chest wall
- The LD flap alone rarely provides sufficient volume to reconstruct a breast, so a subpectoral implant is placed under the LD muscle at the anterior chest wall to augment volume
- Used as a salvage option after failed microsurgical (DIEP, TRAM) flaps
- Skin paddle can be oriented transversely to hide scar in the bra line
- Current Surgical Therapy 14e, p.842
2. Head and Neck Reconstruction (free flap)
The LD free flap is particularly suited for large defects:
- Large scalp defects
- Cranio-orbital defects
- Cheek and maxillectomy reconstruction
- Lower lip/chin complex
- Tongue reconstruction
- Pharyngoesophageal reconstruction
- As a pedicled flap: lateral neck and scalp (transposed subcutaneously or via transaxillary approach)
- K.J. Lee's Essential Otolaryngology, p.1090 & p.1094
3. Lower Extremity / Trauma Reconstruction
- Preferred muscle flap for large soft-tissue defects (>15 cm) of the distal lower extremity, particularly after orthopedic procedures such as sequestrectomy for osteomyelitis
- Can be combined with serratus anterior as a chimeric flap for massive traumatic defects
- The long, large-caliber pedicle allows tension-free anastomosis outside the zone of injury
- Rockwood & Green's Fractures, p.752; Campbell's Operative Orthopaedics, p.3928
4. Functioning Muscle Transfer
- Can be transferred as a functioning neuromuscular unit (motor innervated by thoracodorsal nerve) for restoring active movement in the forearm or face
Advantages
- Predictable, reliable blood supply (Type V muscle; thoracodorsal artery dominant pedicle)
- Largest available muscle flap - up to 20 × 40 cm surface area
- Long vascular pedicle with large-caliber vessels - easy microvascular anastomosis
- Can be harvested quickly due to reliable anatomic landmarks
- Versatile: pedicled or free, muscle-only or myocutaneous
- Part of the subscapular "superflap" system for multi-tissue reconstruction on a single pedicle
- Shoulder mobilization can begin the day after surgery
Disadvantages and Complications
| Issue | Detail |
|---|---|
| Positioning | Lateral decubitus required - makes simultaneous two-team surgery difficult |
| Seroma | Donor site seroma is common despite postoperative drains |
| Shoulder/upper-limb weakness | Up to 30% incidence reported in some series |
| Volume | Rarely provides sufficient volume alone for breast reconstruction |
| Donor site dehiscence | Frequent, especially at the wound edges |
| Scapular winging risk | The branch to serratus anterior (and its nerve) must be preserved when dividing the LD insertion; failure to do so risks winging of the scapula |
Key Technical Pearls
- Identify serratus anterior first - its perpendicular fibres distinguish it from LD; staying superficial to it protects the pedicle
- To find the thoracodorsal pedicle: identify serratus branches and follow them proximally to the thoracodorsal trunk
- For free flaps: ligating the circumflex scapular vessels allows dissection to the subscapular artery, providing maximum pedicle length
- The skin island should be placed along the anterior inferior portion of the muscle for best perforator density
- Suction drainage at the donor site is essential to reduce seroma/hematoma risk
- Flap cooling with iced saline during ischemia time reduces metabolic demand and extends safe ischemic time
Sources:
- Current Surgical Therapy, 14th ed., p.842 - Pedicled LD Flap / Breast Reconstruction
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, pp.1338, 1348 - Surgical technique, scapular system anatomy
- K.J. Lee's Essential Otolaryngology, pp.1090, 1094 - Pedicled and free LD flap for H&N
- Rockwood & Green's Fractures in Adults, 10th ed., p.752 - LD and serratus anterior flaps for trauma
- Campbell's Operative Orthopaedics, 15th ed., p.3928 - LD musculocutaneous flap technique
This is a shared conversation. Sign in to Orris to start your own chat.