Abdoman important topics explanations in details for university exam mbbs 1st year
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Loading Image
I now have comprehensive content. Let me compile the complete, detailed MBBS 1st year Abdomen guide.
Abdomen - Important Topics for MBBS 1st Year (Detailed Notes)
Sources: Gray's Anatomy for Students, General Anatomy and Musculoskeletal System (Thieme Atlas), Bailey and Love's Surgery
TOPIC 1: Boundaries and Surface Anatomy of the Abdomen
The abdomen extends between the thorax above and the pelvis below.
Palpable Bony Landmarks:
- Above: Costal margin (separates abdomen from thorax)
- Below: Pubic tubercle, Anterior Superior Iliac Spine (ASIS), iliac crest
- The inguinal ligament runs between ASIS and pubic tubercle, separating the anterior abdominal wall from the thigh
- The dome of the right diaphragm can reach as high as the 4th costal cartilage during forced expiration - so abdominal viscera in this upper region are protected by the thoracic cage
Quadrant/Region Division:
| 9-Region System | 4-Quadrant System |
|---|---|
| Right hypochondrium, Epigastric, Left hypochondrium | Right Upper Quadrant (RUQ) |
| Right lumbar, Umbilical, Left lumbar | Left Upper Quadrant (LUQ) |
| Right iliac fossa, Hypogastric/Pubic, Left iliac fossa | Right/Left Lower Quadrants |
- Gray's Anatomy for Students, p. 466
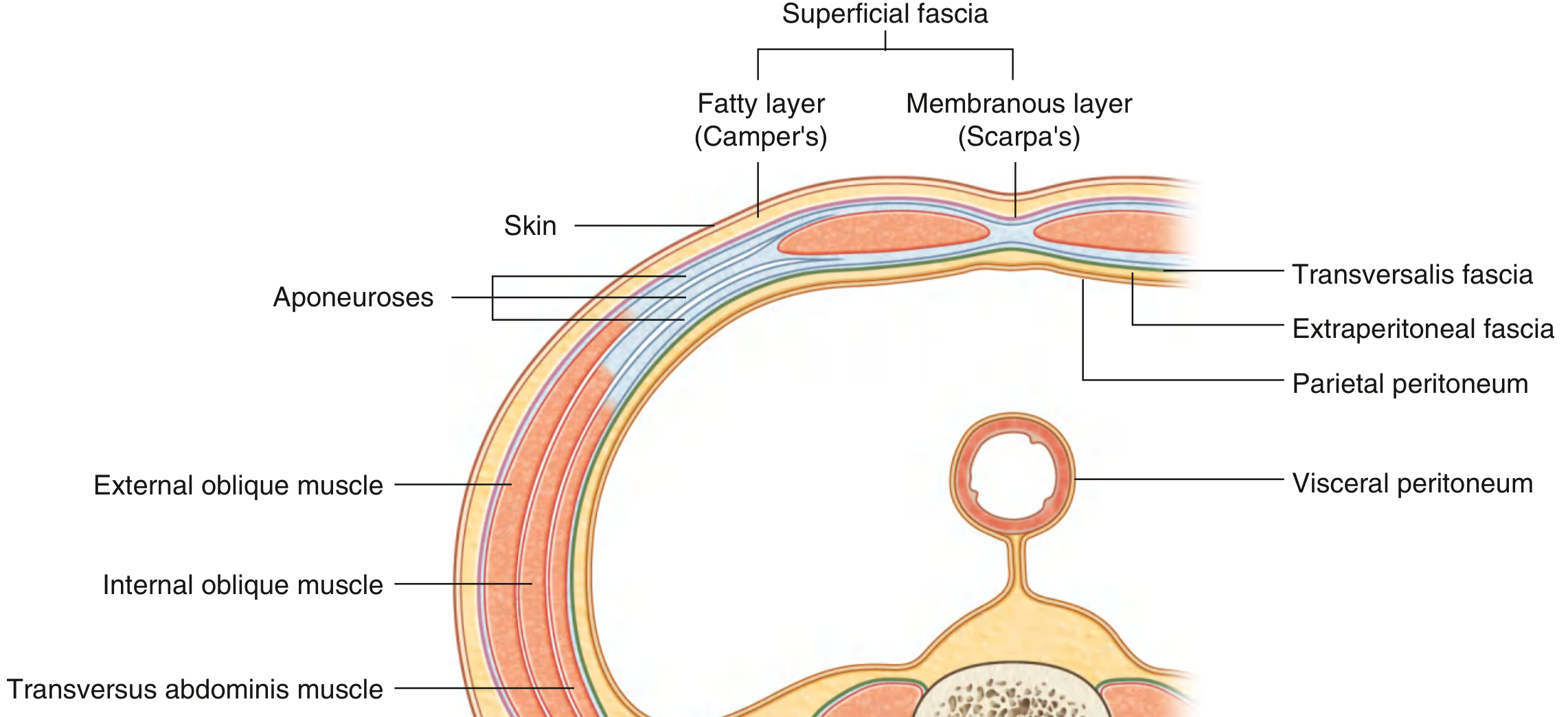
TOPIC 2: Layers of the Anterior Abdominal Wall
From superficial to deep, the anterolateral abdominal wall consists of:
- Skin
- Superficial fascia - has two layers:
- Camper's fascia - superficial fatty layer
- Scarpa's fascia - deep membranous layer (continues into the perineum as Colles' fascia)
- Three flat muscles + their aponeuroses (see below)
- Transversalis fascia - lines the inner surface of transversus abdominis
- Extraperitoneal fascia - divided into preperitoneal (anteriorly) and retroperitoneal (posteriorly)
- Parietal peritoneum - innermost lining
TOPIC 3: Muscles of the Anterolateral Abdominal Wall
Five muscles form the abdominal wall. The key ones for MBBS exams:
Flat Muscles (Lateral Group)
| Muscle | Origin | Insertion | Nerve Supply | Action |
|---|---|---|---|---|
| External oblique | Outer surfaces of ribs V-XII (lower 8 ribs) | Iliac crest (lateral lip); aponeurosis to linea alba | T7-T12 (anterior rami) | Compresses abdomen; flexes trunk; rotates to opposite side |
| Internal oblique | Thoracolumbar fascia; iliac crest; lateral 2/3 of inguinal ligament | Lower 3-4 ribs; aponeurosis to linea alba; pubic crest | T7-T12 and L1 | Compresses abdomen; rotates to same side |
| Transversus abdominis | Thoracolumbar fascia; iliac crest (medial lip); lateral 1/3 inguinal ligament; costal cartilages VII-XII | Aponeurosis to linea alba; pubic crest | T7-T12 and L1 | Compresses abdominal contents only (no rotation) |
Vertical Muscles (Medial Group)
| Muscle | Origin | Insertion | Nerve Supply | Action |
|---|---|---|---|---|
| Rectus abdominis | Pubic crest, pubic tubercle, pubic symphysis | Costal cartilages V-VII; xiphoid process | T7-T12 | Flexes vertebral column; compresses abdomen; tenses wall |
| Pyramidalis | Front of pubis | Linea alba | T12 | Tenses linea alba (often absent) |
Clinical Mnemonics
- The fiber direction of flat muscles: External oblique - "hands in pockets" (downward-medial); Internal oblique - perpendicular; Transversus - horizontal.
- Rectus abdominis has 3-4 tendinous intersections which are visible in developed individuals (the "six-pack").
Key Structures Formed by Aponeuroses:
Rectus Sheath:
- Above arcuate line: anterior wall = external oblique + anterior leaf of internal oblique; posterior wall = posterior leaf of internal oblique + transversus
- Below arcuate line: all three aponeuroses pass anterior to rectus, leaving the posterior wall covered only by transversalis fascia
Linea Alba: Midline raphe formed by the fusion of all three aponeuroses. Extends from xiphoid process to pubic symphysis.
Arcuate Line (of Douglas): Midpoint between umbilicus and pubis. Below this, the posterior rectus sheath is absent.
- Gray's Anatomy for Students, p. 344
TOPIC 4: Innervation of the Anterior Abdominal Wall
Supplied by T7 to T12 and L1 spinal nerves (anterior rami).
- Intercostal nerves (T7-T11) leave their intercostal spaces and run between internal oblique and transversus abdominis, then enter the rectus sheath to supply skin via anterior cutaneous branches
- T12 = subcostal nerve
- L1 = gives iliohypogastric and ilio-inguinal nerves
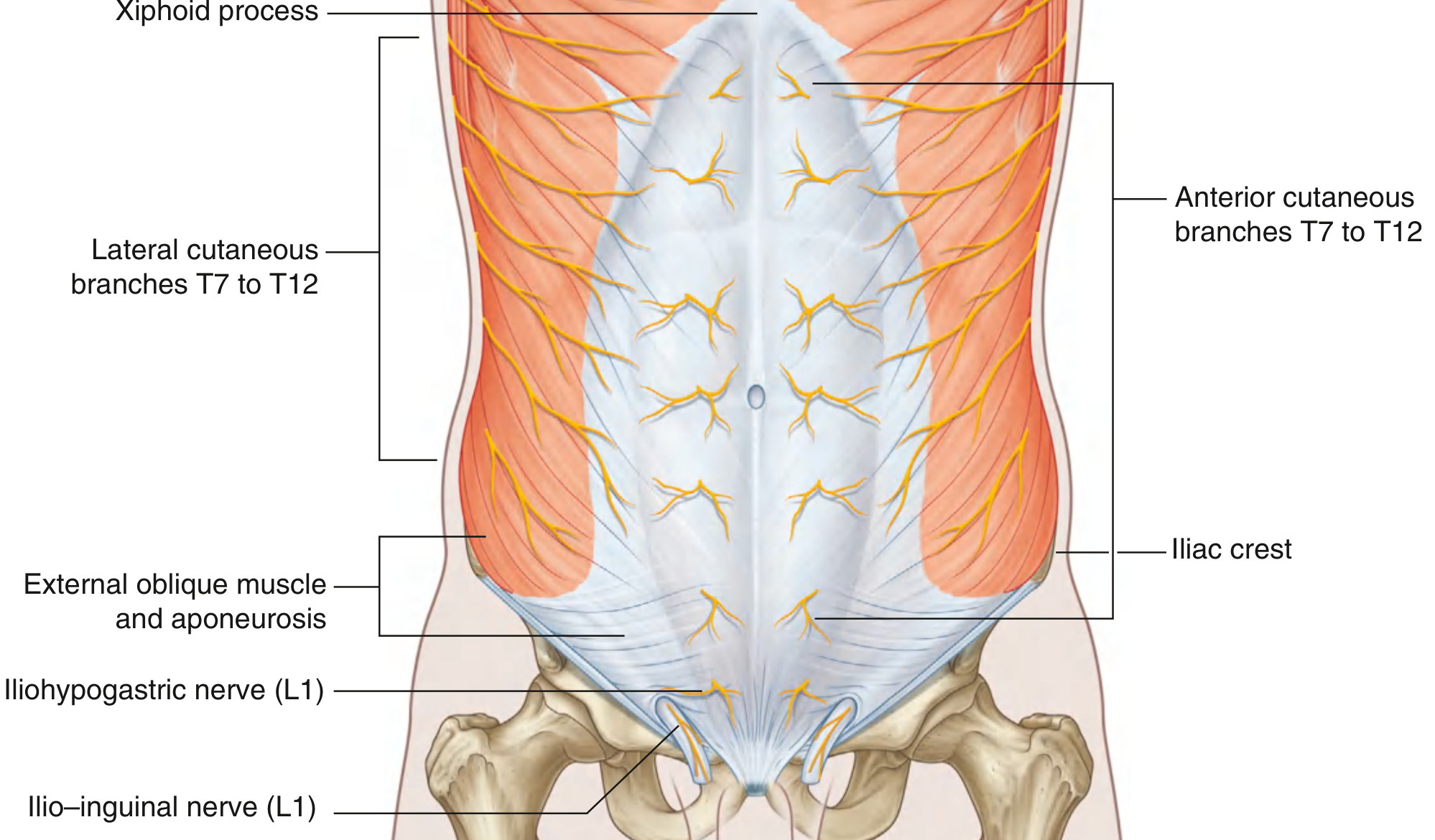
Dermatome landmarks (high-yield for exams):
- T7-T9 = above umbilicus
- T10 = at the umbilicus
- T11-T12 = below umbilicus
- L1 = groin
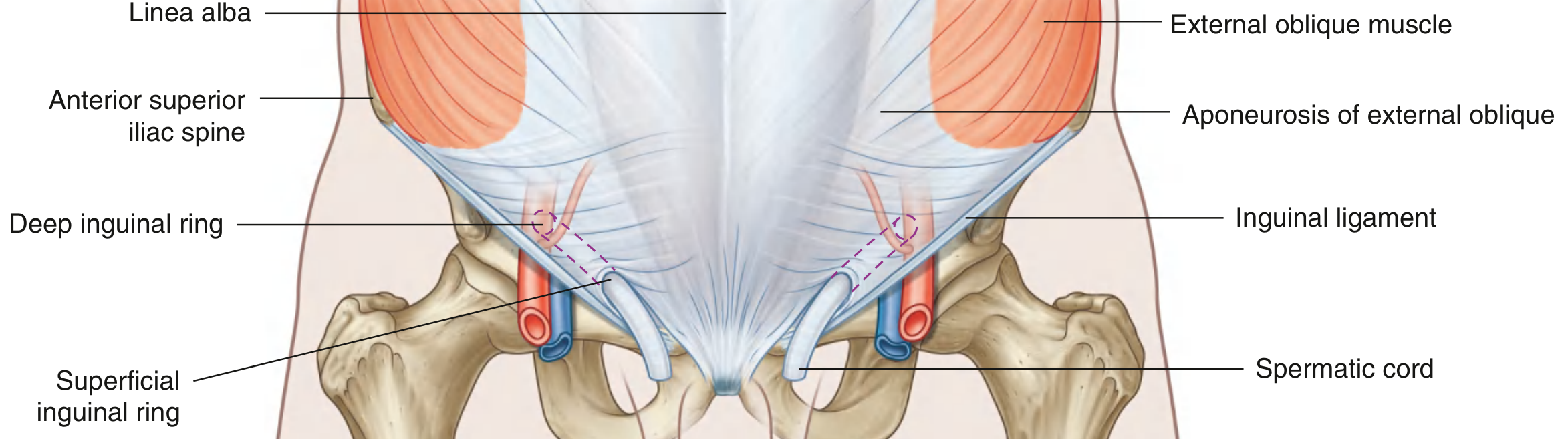
TOPIC 5: Inguinal Canal
The inguinal canal is a slit-like passage that is a high-yield topic in every MBBS 1st year exam.
Key Facts:
- Length: Approximately 4 cm
- Direction: Downward and medially, parallel to the lower half of the inguinal ligament
- Begins at: Deep (internal) inguinal ring
- Ends at: Superficial (external) inguinal ring
Deep Inguinal Ring
- Located midway between ASIS and pubic symphysis, just above the inguinal ligament
- Lies lateral to the inferior epigastric vessels (important for distinguishing indirect vs direct hernia)
- Not a true hole - it is an evagination of the transversalis fascia
Superficial Inguinal Ring
- Located superolateral to the pubic tubercle
- Triangular opening in the aponeurosis of external oblique
- Apex points superolaterally; base formed by pubic crest
- Two crura: medial crus (to pubic symphysis) and lateral crus (to pubic tubercle)
- Held together at apex by intercrural fibers
Walls of the Inguinal Canal
| Wall | Formation |
|---|---|
| Anterior wall | Aponeurosis of external oblique (entire length); internal oblique muscle (lateral 1/3) |
| Posterior wall | Transversalis fascia (entire length); conjoint tendon medially |
| Roof (superior wall) | Arched fibers of internal oblique and transversus abdominis |
| Floor (inferior wall) | Inguinal ligament + lacunar ligament medially |
Contents:
| In Males | In Females |
|---|---|
| Spermatic cord | Round ligament of uterus |
| Ilio-inguinal nerve (in both) | Ilio-inguinal nerve (in both) |
| Genital branch of genitofemoral nerve (in both) | Genital branch of genitofemoral nerve (in both) |
Spermatic Cord Coverings (from outside in):
- External spermatic fascia - from external oblique aponeurosis
- Cremasteric fascia and cremasteric muscle - from internal oblique
- Internal spermatic fascia - from transversalis fascia
Contents of Spermatic Cord:
- Ductus (vas) deferens
- Testicular artery (from aorta)
- Artery to ductus deferens
- Cremasteric artery (from inferior epigastric)
- Pampiniform plexus of veins
- Lymphatics
- Sympathetic nerves
- Genital branch of genitofemoral nerve
Clinical Application - Inguinal Hernias:
-
Indirect inguinal hernia: Passes through the deep inguinal ring (lateral to inferior epigastric vessels), traverses the inguinal canal, and exits through the superficial ring. More common, especially in males. Congenital.
-
Direct inguinal hernia: Protrudes directly through the posterior wall of the inguinal canal (Hesselbach's triangle), medial to inferior epigastric vessels. Acquired, seen in older men with weak abdominal muscles.
-
Hesselbach's triangle: Bounded laterally by inferior epigastric vessels, medially by lateral border of rectus abdominis, inferiorly by inguinal ligament.
-
Gray's Anatomy for Students, p. 352
TOPIC 6: Peritoneum
Definition and Layers:
- The peritoneum is a thin serous membrane lining the abdominal cavity
- Parietal peritoneum: Lines the walls of the abdominal cavity
- Visceral peritoneum: Covers the abdominal viscera
- Peritoneal cavity: Potential space between the two layers. Closed in men; has two openings in women (via uterine tubes)
Peritoneal Cavity Subdivisions:
- Greater sac - main large portion
- Lesser sac (omental bursa) - posterior to the stomach, communicates with greater sac via the epiploic foramen (foramen of Winslow)
Visceral Positions:
| Intraperitoneal organs | Retroperitoneal organs |
|---|---|
| Stomach, liver, spleen | Kidneys, ureters, adrenal glands |
| Jejunum, ileum | Aorta, IVC |
| Transverse colon, sigmoid colon | Duodenum (2nd, 3rd, 4th parts) |
| Uterus, ovaries (females) | Pancreas (except tail) |
| Ascending colon, descending colon | |
| Rectum (lower 2/3) |
Mnemonic for retroperitoneal organs: "SAD PUCKER"
- Suprarenal glands (adrenals)
- Aorta + IVC
- Duodenum (2nd-4th parts)
- Pancreas (except tail)
- Ureters
- Colon (ascending and descending)
- Kidneys
- Esophagus (lower part)
- Rectum
Peritoneal Folds and Ligaments:
- Mesentery: Fan-shaped fold connecting jejunum/ileum to posterior abdominal wall; root goes from left of L2 to right iliac fossa
- Greater omentum: Apron-like fold hanging from greater curvature of stomach; acts as "abdominal policeman" by walling off infections
- Lesser omentum: Between liver and lesser curvature of stomach + duodenum; contains hepatic artery, portal vein, bile duct in its free edge
- Falciform ligament: Connects liver to anterior abdominal wall; contains ligamentum teres (obliterated umbilical vein) in its free edge
- Coronary ligament: Connects liver to diaphragm
Innervation of Peritoneum:
- Parietal peritoneum - somatic innervation (spinal nerves T7-L1) → well-localized, sharp pain; tenderness and guarding
- Visceral peritoneum - autonomic/visceral innervation → poorly localized, dull, crampy pain; referred pain patterns
Pouches (Clinically Important):
-
Hepatorenal pouch (Morrison's pouch): Between liver and right kidney; lowest point of peritoneal cavity when supine - fluid collects here first
-
Recto-uterine pouch (Pouch of Douglas): In females, between uterus and rectum; lowest point of peritoneal cavity in females when standing - fluid, pus, blood collect here first
-
Vesico-uterine pouch: Between bladder and uterus in females
-
Paracolic gutters: On either side of the ascending/descending colon - allows fluid to spread up to the subphrenic space
-
Gray's Anatomy for Students, p. 346, 362
TOPIC 7: Hernias of the Abdominal Wall
A hernia is the protrusion of a viscus (or part of it) through the walls of the cavity that normally contains it.
Types:
- Inguinal hernia (most common overall) - see above
- Femoral hernia: Below and lateral to pubic tubercle, through femoral canal. More common in females. High risk of strangulation.
- Umbilical hernia: Through umbilicus - congenital (failure of bowel to return from umbilical cord) or acquired (para-umbilical in adults)
- Incisional hernia: Through scar of previous surgery; wide neck, less risk of strangulation
- Epigastric hernia: Through linea alba between xiphoid and umbilicus
- Spigelian hernia: Through arcuate line into lateral border of posterior rectus sheath
Parts of a Hernia:
- Sac - peritoneum
- Contents - viscus (omentum, bowel)
- Coverings - layers of abdominal wall
Complications:
-
Irreducible: Cannot be pushed back
-
Obstructed: Bowel within hernia is obstructed
-
Strangulated: Blood supply cut off - surgical emergency
-
Gray's Anatomy for Students, p. 351-354
TOPIC 8: Stomach
Position:
- Located in the left hypochondrium and epigastric region
- Lies between esophagus (cardia) and duodenum (pylorus)
Parts:
- Cardia - where esophagus joins (at T11)
- Fundus - dome-shaped part above cardia, related to left dome of diaphragm
- Body - largest part
- Pyloric antrum and pyloric canal - leads to pylorus
- Pylorus - at L1 vertebra level; contains pyloric sphincter
Curvatures:
- Lesser curvature - right border, related to lesser omentum
- Greater curvature - left border, related to greater omentum
Blood Supply:
| Artery | Origin | Supplies |
|---|---|---|
| Left gastric | Celiac trunk | Lesser curvature |
| Right gastric | Hepatic artery | Lesser curvature |
| Left gastroepiploic | Splenic artery | Greater curvature |
| Right gastroepiploic | Gastroduodenal artery | Greater curvature |
| Short gastric arteries | Splenic artery | Fundus |
All ultimately from celiac trunk (T12/L1)
Relations:
- Anterior: Left lobe of liver, diaphragm, anterior abdominal wall
- Posterior: Lesser sac (omental bursa), pancreas, left kidney, spleen
Nerve Supply:
- Parasympathetic: Vagus nerves (CN X) - left vagus = anterior, right vagus = posterior
- Sympathetic: T6-T10 via celiac plexus
TOPIC 9: Duodenum
- C-shaped structure, about 25 cm long
- Mostly retroperitoneal (except the first 2.5 cm which is intraperitoneal)
- Surrounds the head of the pancreas
Parts:
| Part | Level | Features |
|---|---|---|
| 1st (superior) | L1 | "Duodenal cap" on X-ray; common site for duodenal ulcer |
| 2nd (descending) | L1-L3 | Ampulla of Vater (hepatopancreatic ampulla) opens here; where bile + pancreatic juice enter |
| 3rd (horizontal) | L3 | Crosses the aorta and IVC; superior mesenteric artery and vein cross in front |
| 4th (ascending) | L3-L2 | Ends at duodenojejunal flexure (at L2); held by ligament of Treitz |
Blood Supply:
- Superior pancreaticoduodenal artery (from gastroduodenal = celiac)
- Inferior pancreaticoduodenal artery (from superior mesenteric artery)
- This junction marks the boundary between foregut and midgut
TOPIC 10: Liver
Position:
- Right hypochondrium + epigastric region
- Protected by lower ribs
- Lower border of liver is felt at the right costal margin at rest
Surfaces and Lobes:
- Diaphragmatic surface (anterior, superior, posterior) - smooth, convex
- Visceral surface (inferior) - has H-shaped fissures dividing into 4 lobes
4 Lobes (morphological):
- Right lobe (largest)
- Left lobe
- Caudate lobe (between IVC and ligamentum venosum)
- Quadrate lobe (between gallbladder and ligamentum teres)
Functional division (Couinaud): Left and right functional lobes divided by the middle hepatic vein and IVC plane (Cantlie's line)
Porta Hepatis (Gateway of the Liver):
Located on the visceral surface, contains (from front to back):
- Hepatic duct (bile duct - anterior)
- Hepatic artery (middle)
- Portal vein (posterior and largest)
Mnemonic: "BDA" - Bile duct, artery, vein (Duct + Artery anterior, vein posterior)
Blood Supply:
- Hepatic artery proper (25% of blood flow, 50% of oxygen)
- Portal vein (75% of blood flow, 50% of oxygen)
- Drained by hepatic veins (right, middle, left) → IVC
Portal Vein:
- Formed behind the neck of pancreas by union of superior mesenteric vein + splenic vein
- Carries nutrient-rich blood from GI tract and spleen to liver
- No valves (important clinically - portal hypertension)
- Level: L1-L2
Portal-Systemic (Porto-caval) Anastomoses:
Critical for exams - sites where portal and systemic venous systems communicate:
| Site | Portal vessel | Systemic vessel | Clinical result |
|---|---|---|---|
| Lower esophagus | Esophageal tributaries of left gastric | Azygos/hemiazygos | Esophageal varices |
| Rectum | Superior rectal (IMV) | Middle/inferior rectal | Rectal varices/hemorrhoids |
| Umbilicus | Paraumbilical veins | Epigastric veins | Caput medusae |
| Bare area of liver | Small hepatic veins | Phrenic veins | Rarely symptomatic |
| Retroperitoneum | Colic/intestinal veins | Lumbar/renal veins | Veins of Retzius |
These anastomoses open up in portal hypertension (e.g., liver cirrhosis)
Ligaments of Liver:
- Falciform ligament - connects liver to anterior abdominal wall; contains ligamentum teres (obliterated left umbilical vein of fetus) in its free edge
- Coronary ligament - connects liver to diaphragm; the two layers separate to create the bare area of liver (not covered by peritoneum)
- Ligamentum venosum - fibrous remnant of ductus venosus (shunted blood from portal vein to IVC in fetus)
TOPIC 11: Gallbladder and Bile Duct
Gallbladder:
- Stores and concentrates bile (up to 10x)
- Located in gallbladder fossa on visceral surface of right lobe of liver
- Parts: Fundus, Body, Neck (neck has spiral valve of Heister; Hartmann's pouch is at the junction of neck and cystic duct - gallstones lodge here)
Calot's Triangle (Cystohepatic Triangle):
- Boundaries: Cystic duct (inferiorly), common hepatic duct (medially), inferior surface of liver (superiorly)
- Contents: Cystic artery (usually a branch of right hepatic artery)
- Critical for cholecystectomy - identify and ligate cystic artery here
Biliary Tree:
Right hepatic duct + Left hepatic duct → Common hepatic duct → joins cystic duct → Common bile duct (CBD) → joins main pancreatic duct → Ampulla of Vater → opens at major duodenal papilla in 2nd part of duodenum
TOPIC 12: Pancreas
- Both exocrine (acini secrete digestive enzymes) and endocrine (islets of Langerhans: insulin/glucagon)
- Lies retroperitoneal across the posterior abdominal wall at L1-L2
Parts:
- Head - in the C-loop of duodenum; uncinate process projects from head
- Neck - anterior to portal vein (formed here); posterior to pylorus
- Body - crosses L1-L2; posterior to lesser sac
- Tail - tip enters the splenorenal ligament; only intraperitoneal part; related to hilum of spleen
Main Pancreatic Duct (Wirsung) + Accessory Duct (Santorini):
- Main duct runs from tail to head, joins CBD at ampulla of Vater
- Accessory duct opens separately at minor duodenal papilla above the major papilla
Blood Supply:
- Head: Superior + inferior pancreaticoduodenal arteries
- Body/tail: Splenic artery branches
TOPIC 13: Spleen
- Largest lymphoid organ in the body
- Located in left hypochondrium, at the level of ribs 9-11
- Long axis lies along the 10th rib
- Can only be felt clinically when enlarged more than 3 times normal size
Features:
- Notched anterior border - distinguishes spleen from other masses on palpation
- Protected by ribs 9-11; rib fractures commonly injure the spleen
- Lies against the diaphragm, left kidney, and tail of pancreas
Blood Supply:
- Splenic artery (largest branch of celiac trunk; tortuous course along upper border of pancreas)
- Splenic vein (joins superior mesenteric vein → portal vein)
Functions:
- Filters blood (removes old/damaged RBCs)
- Immune function (production of IgM)
- In fetus: hematopoiesis
- Reservoir of blood/platelets
Clinical:
- Splenomegaly: Extends towards right iliac fossa following the line of the 10th rib
- Hypersplenism: Overactive spleen destroys blood cells
- Spleen vs. kidney distinction: Spleen has a notch, cannot "get above" it, moves with respiration, not ballottable, dull to percussion
TOPIC 14: Kidneys (Posterior Abdominal Wall)
Position:
- Retroperitoneal, on either side of vertebral column at T12-L3
- Right kidney is lower (pushed down by liver) - at L1-L3
- Left kidney is slightly higher - at T12-L2
- The hilus is at the level of transpyloric plane (L1)
Coverings (from inside out):
- Fibrous capsule (renal capsule)
- Perirenal fat (adipose capsule)
- Renal (Gerota's) fascia - encloses kidney and adrenal gland
- Pararenal fat (paranephric fat)
Relations of the Kidney:
Right kidney:
- Anterior: Right suprarenal gland (superomedial), liver, hepatic flexure of colon, 2nd part of duodenum
- Posterior: Diaphragm, 12th rib, psoas major, quadratus lumborum, transversus abdominis
Left kidney:
- Anterior: Left suprarenal gland, stomach, spleen, tail of pancreas, jejunum, splenic flexure of colon
- Posterior: Same muscles + 11th and 12th ribs
Blood Supply:
- Renal arteries from aorta at L1 level (right longer than left)
- Sequence: Segmental arteries → lobar → interlobar → arcuate → interlobular arteries
- Avascular plane (Brodel's line): Between anterior 4 and posterior 1 segment; used for incisions during pyelolithotomy
Ureter (Anatomy):
- ~25 cm long
- Three sites of narrowing (where stones lodge):
- Pelviureteric junction (PUJ) - most proximal
- Pelvic brim - where ureter crosses iliac vessels
- Vesicoureteric junction (VUJ) - where it enters bladder wall (narrowest point)
TOPIC 15: Posterior Abdominal Wall Muscles
| Muscle | Origin | Insertion | Nerve Supply | Action |
|---|---|---|---|---|
| Psoas major | T12-L5 vertebrae (bodies + transverse processes) | Lesser trochanter of femur | L1-L3 | Flexes thigh at hip; flexes lumbar spine |
| Iliacus | Iliac fossa | Lesser trochanter | Femoral nerve (L2-L4) | Flexes thigh |
| Quadratus lumborum | Iliac crest, iliolumbar ligament | 12th rib, L1-L4 transverse processes | T12, L1-L4 | Depresses 12th rib; lateral flexion of spine |
Psoas major forms a fascial sheath - a "psoas abscess" (TB of vertebrae) can track down within this sheath to present in the thigh.
TOPIC 16: Diaphragm
Structure:
- Musculotendinous partition separating thorax from abdomen
- Muscle fibers arise from periphery and converge on the central tendon in the middle
Origins (Three Parts):
- Sternal part: Posterior surface of xiphoid process
- Costal part: Inner surfaces of lower 6 costal cartilages and adjacent ribs
- Lumbar part: Medial and lateral arcuate ligaments + crura (from L1-L3)
Three Major Openings:
| Opening | Level | Structures passing through |
|---|---|---|
| Caval opening (Vena caval hiatus) | T8 | IVC + right phrenic nerve |
| Esophageal hiatus | T10 | Esophagus + both vagal trunks + esophageal branches of left gastric vessels |
| Aortic hiatus | T12 | Aorta + thoracic duct + azygos vein |
Mnemonic for levels: "I 8 (ate) 10 (ten) eggs at 12 (twelve)"
- I (IVC) = T8
- Ate (esophagus) = T10
- Eggs (aorta/EGG-orta) = T12
Nerve Supply:
- Motor: Phrenic nerve (C3, C4, C5 - "C3, 4, 5 keeps the diaphragm alive")
- Sensory: Central diaphragm = phrenic nerve (referred to C3-C5 dermatome = shoulder tip); Peripheral = lower intercostal nerves
Clinical:
- Hiatus hernia: Stomach slides through esophageal hiatus (sliding type - most common) or herniates alongside esophagus (rolling/para-esophageal type)
- Phrenic nerve irritation (e.g., blood under diaphragm) causes referred pain to the shoulder tip
TOPIC 17: Celiac, Superior Mesenteric, and Inferior Mesenteric Arteries
Celiac Trunk (T12/L1):
"Foregut artery" - supplies organs derived from foregut (distal esophagus to first half of duodenum + liver, spleen, pancreas)
Three branches:
- Left gastric artery - smallest; to stomach (lesser curvature) + lower esophagus
- Splenic artery - largest; to spleen, gives short gastric and left gastroepiploic arteries, pancreatic branches
- Common hepatic artery - to liver; gives off gastroduodenal artery (→ superior pancreaticoduodenal + right gastroepiploic) and right gastric artery, then becomes hepatic artery proper
Superior Mesenteric Artery (SMA) (L1):
"Midgut artery" - from second half of duodenum to 2/3 of transverse colon
Branches:
- Inferior pancreaticoduodenal artery
- Jejunal and ileal arteries (10-16 branches forming arterial arcades → vasa recta)
- Ileocolic artery (→ appendicular artery)
- Right colic artery
- Middle colic artery
Inferior Mesenteric Artery (IMA) (L3):
"Hindgut artery" - from left 1/3 of transverse colon to upper rectum
Branches:
- Left colic artery
- Sigmoid arteries
- Superior rectal artery
Marginal artery of Drummond: Arcade formed by SMA and IMA branches running along the mesenteric border of the colon - ensures collateral supply.
TOPIC 18: Important Vertical Planes and Clinical Landmarks
| Plane | Level | Structures at this level |
|---|---|---|
| Transpyloric plane (L1) | Midpoint between jugular notch and pubic symphysis | Pylorus of stomach; neck of pancreas; duodenojejunal flexure; hilus of kidneys; origin of SMA; conus medullaris |
| Transtubercular plane (L5) | Level of iliac tubercles (5 cm behind ASIS) | L5 vertebra; bifurcation of IVC |
| Subcostal plane (L3) | Lower margin of costal cartilage 10 | Origin of IMA |
| Intertubercular plane (L5) | Between iliac tubercles | Bifurcation of aorta (L4, but the plane at L5) |
| Midclavicular line | Vertical from midpoint of clavicle | Lateral border of rectus abdominis |
Quick Revision Summary Table
| Topic | Most High-Yield Fact |
|---|---|
| Abdominal wall layers | Skin → Camper's → Scarpa's → muscles → transversalis fascia → extraperitoneal fascia → peritoneum |
| Inguinal canal floor | Inguinal ligament + lacunar ligament (medially) |
| Deep inguinal ring location | Midpoint ASIS-pubic symphysis, lateral to inferior epigastric |
| Indirect vs direct hernia | Lateral vs medial to inferior epigastric vessels |
| Diaphragm openings | T8 IVC, T10 esophagus, T12 aorta |
| Portal vein formed | Behind neck of pancreas = SMV + splenic vein |
| Porta hepatis (front to back) | Bile duct, Hepatic artery, Portal vein |
| Porto-systemic anastomoses | Esophagus (varices), rectum (hemorrhoids), umbilicus (caput medusae) |
| Ureter narrowings (3) | PUJ, pelvic brim (iliac crossing), VUJ |
| Transpyloric plane (L1) | Pylorus, hilus of kidney, neck of pancreas, origin of SMA |
| Calot's triangle contents | Cystic artery (from right hepatic) |
| Celiac trunk branches | Left gastric, splenic, common hepatic |
| Phrenic nerve roots | C3, C4, C5 |
All anatomical content sourced from: Gray's Anatomy for Students (9780323934237), General Anatomy and Musculoskeletal System - Thieme Atlas (9781626237186), Bailey and Love's Short Practice of Surgery (9780367548117)
Pelvis explain in details for university exam mbbs 1st year for write in exam
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
I now have sufficient textbook content and images to write a complete, exam-focused guide on the Pelvis. Let me compile it now.
THE PELVIS - Complete MBBS 1st Year Exam Notes
Sources: Gray's Anatomy for Students, General Anatomy & Musculoskeletal System (Thieme Atlas), Mulholland & Greenfield's Surgery, Campbell-Walsh Urology
TOPIC 1: Introduction and Definition
The pelvis is the basin-shaped bony structure at the lower end of the vertebral column. It connects the trunk to the lower limbs and contains important viscera (urinary bladder, rectum, reproductive organs), major blood vessels, and nerves.
The term "pelvis" is used in two senses:
- Bony pelvis - the skeletal framework
- Pelvic cavity - the space enclosed within it
TOPIC 2: Bony Pelvis
Bones Forming the Pelvis:
The pelvis is formed by 4 bones:
- Two hip bones (os coxae) - each formed by fusion of ilium, ischium, and pubis
- Sacrum
- Coccyx
Hip Bone (Os Coxae):
Each hip bone consists of three parts that fuse at the acetabulum by age 15-17:
| Bone | Position | Key Features |
|---|---|---|
| Ilium | Superiorly | Iliac crest, ASIS, AIIS, PSIS, iliac fossa, gluteal surface |
| Ischium | Posteroinferiorly | Ischial tuberosity (weight bearing when sitting), ischial spine, lesser sciatic notch |
| Pubis | Anteroinferiorly | Pubic body, superior and inferior rami, pubic crest, pubic tubercle |
Obturator foramen: Large opening formed by ischium + pubis; closed by obturator membrane except for the obturator canal (superiorly)
Joints of the Pelvis:
| Joint | Type | Features |
|---|---|---|
| Pubic symphysis | Secondary cartilaginous (fibrocartilage) | Midline; slightly mobile; softens in pregnancy |
| Sacroiliac joint | Synovial (plane) + fibrous | Between sacrum and ilium; transmits weight of body to lower limbs |
| Sacrococcygeal joint | Secondary cartilaginous | Between sacrum and coccyx |
Ligaments:
| Ligament | Attachment | Function |
|---|---|---|
| Sacrotuberous | Posterior sacrum → ischial tuberosity | Resists upward rotation of sacrum |
| Sacrospinous | Lateral sacrum → ischial spine | Divides posterior aperture into greater and lesser sciatic foramina |
| Inguinal ligament | ASIS → pubic tubercle | Lower border of anterior abdominal wall |
| Iliolumbar | L5 transverse process → iliac crest | Stabilizes lumbosacral junction |
TOPIC 3: Greater Pelvis vs. Lesser Pelvis
The pelvis is divided into greater (false) pelvis and lesser (true) pelvis by the pelvic brim (linea terminalis):
Pelvic Brim (Linea Terminalis):
A continuous line running from:
- Pubic symphysis (anteriorly) →
- Pubic crest + pectineal line (along superior pubic ramus) →
- Arcuate line of ilium →
- Sacral promontory (posteriorly)
Greater (False) Pelvis:
- Above the pelvic brim
- Part of the abdominal cavity
- Contains iliac fossae and lower abdominal viscera (sigmoid colon, ileum, cecum)
- Has no clinical "obstetric" significance
Lesser (True) Pelvis:
- Below the pelvic brim
- The true pelvic cavity proper
- Contains bladder, rectum, and reproductive organs
- Has an inlet (above), outlet (below), and cavity (between them)
- Clinically significant in obstetrics
TOPIC 4: Pelvic Inlet, Cavity, and Outlet
Pelvic Inlet (Superior Pelvic Aperture):
Bounded by the linea terminalis (pelvic brim)
Diameters of Pelvic Inlet:
| Diameter | Measurement | Description |
|---|---|---|
| Anteroposterior (True conjugate/Obstetric conjugate) | ~11 cm (>10 cm needed for vaginal delivery) | From sacral promontory to upper border of pubic symphysis |
| Diagonal conjugate | ~12.5 cm | From sacral promontory to lower border of pubic symphysis (clinically measurable by vaginal exam) |
| Transverse | ~13 cm (widest) | Widest part of inlet |
| Oblique | ~12 cm | From sacroiliac joint to iliopubic eminence of opposite side |
Obstetric conjugate = Diagonal conjugate - 1.5 cm
Pelvic Outlet (Inferior Pelvic Aperture):
Boundaries:
- Anteriorly: Pubic arch (inferior pubic rami + ischial rami)
- Laterally: Ischial tuberosities + sacrotuberous ligaments
- Posteriorly: Tip of coccyx
Diameters of Pelvic Outlet:
| Diameter | Measurement |
|---|---|
| Anteroposterior | ~13.5 cm (from pubic symphysis to coccyx) |
| Transverse (bispinous) | ~11 cm (between ischial tuberosities) |
Subpubic Angle:
- Males: 70° (narrow, V-shaped - android pelvis)
- Females: 100-110° (wide, U-shaped - gynecoid pelvis)
Pelvic Axis:
A curved line through the center of every pelvic plane - curves anteriorly as it descends (like the letter "J")
TOPIC 5: Male vs. Female Pelvis (Sex Differences)
This is a very common exam question.
| Feature | Male Pelvis | Female Pelvis |
|---|---|---|
| General shape | Narrow, deep, funnel-shaped | Wide, shallow, cylindrical |
| Pelvic inlet | Heart-shaped | Oval/rounded |
| Pelvic outlet | Narrower | Wider |
| Subpubic angle | <90° (60-70°) | >90° (90-110°) |
| Acetabula | Closer together | Further apart |
| Obturator foramen | Round | Oval |
| Greater sciatic notch | Narrow | Wide |
| Sacrum | Long, narrow, with more curvature | Short, wide, less curved |
| Ischial tuberosities | Turned inwards | Everted (turned outwards) |
| Iliac crests | Less flared | More flared |
| Overall build | Heavy/thick | Light/thin |
| Purpose | Built for locomotion | Built for childbirth |
Types of Female Pelvis (Caldwell-Moloy Classification):
- Gynecoid (50%) - round inlet, wide arch - best for delivery
- Android (30%) - heart-shaped inlet, narrow arch - poor for delivery, male type
- Anthropoid (20%) - AP diameter > transverse, oval - delivery possible
- Platypelloid (rare) - flat pelvis, transverse oval, wide arch - difficult delivery
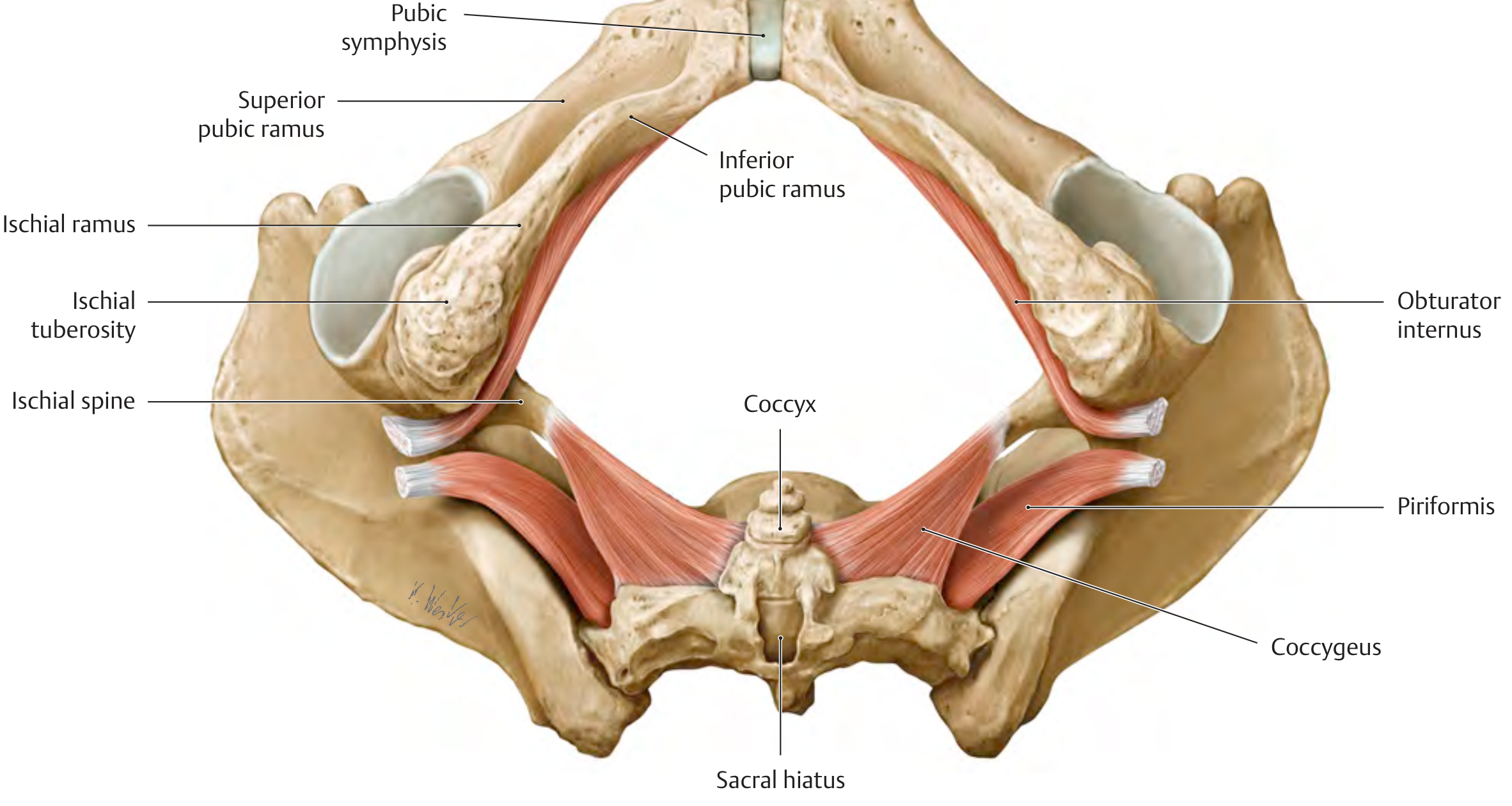
TOPIC 6: Pelvic Walls
Anterior Wall:
Formed by the posterior surface of the pubic bones and symphysis - the shortest wall
Posterior Wall:
Formed by:
- Sacrum (S1-S5)
- Coccyx
- Piriformis muscle covering anterior sacrum
Lateral Walls:
Formed by:
- Inner surface of hip bone below the pelvic brim
- Obturator internus muscle + its fascia (covers most of lateral wall)
- Sacrospinous and sacrotuberous ligaments
Pelvic Wall Muscles:
1. Obturator Internus:
- Origin: Inner surface of obturator membrane + surrounding bone
- Insertion: Greater trochanter of femur (after turning 90° through lesser sciatic foramen)
- Nerve: Nerve to obturator internus (L5, S1, S2)
- Action: Lateral rotation of the extended thigh; abduction of flexed thigh
- Clinical: Its fascia forms the tendinous arch of levator ani and the pudendal canal (Alcock's canal)
2. Piriformis:
- Origin: Anterior surface of sacrum (S2-S4), sacrotuberous ligament
- Insertion: Greater trochanter of femur
- Nerve: S1, S2
- Action: Lateral rotation and abduction of thigh
- Exits: Through greater sciatic foramen, dividing it into:
- Suprapiriform space - superior gluteal nerve and vessels pass through
- Infrapiriform space - inferior gluteal nerve/vessels + sciatic nerve + pudendal nerve and vessels + nerve to obturator internus + nerve to quadratus femoris pass through
- Clinical: Piriformis syndrome - sciatic nerve compressed by piriformis → buttock pain + sciatica
TOPIC 7: Pelvic Floor (Pelvic Diaphragm)
This is the MOST HIGH-YIELD topic in pelvic anatomy.
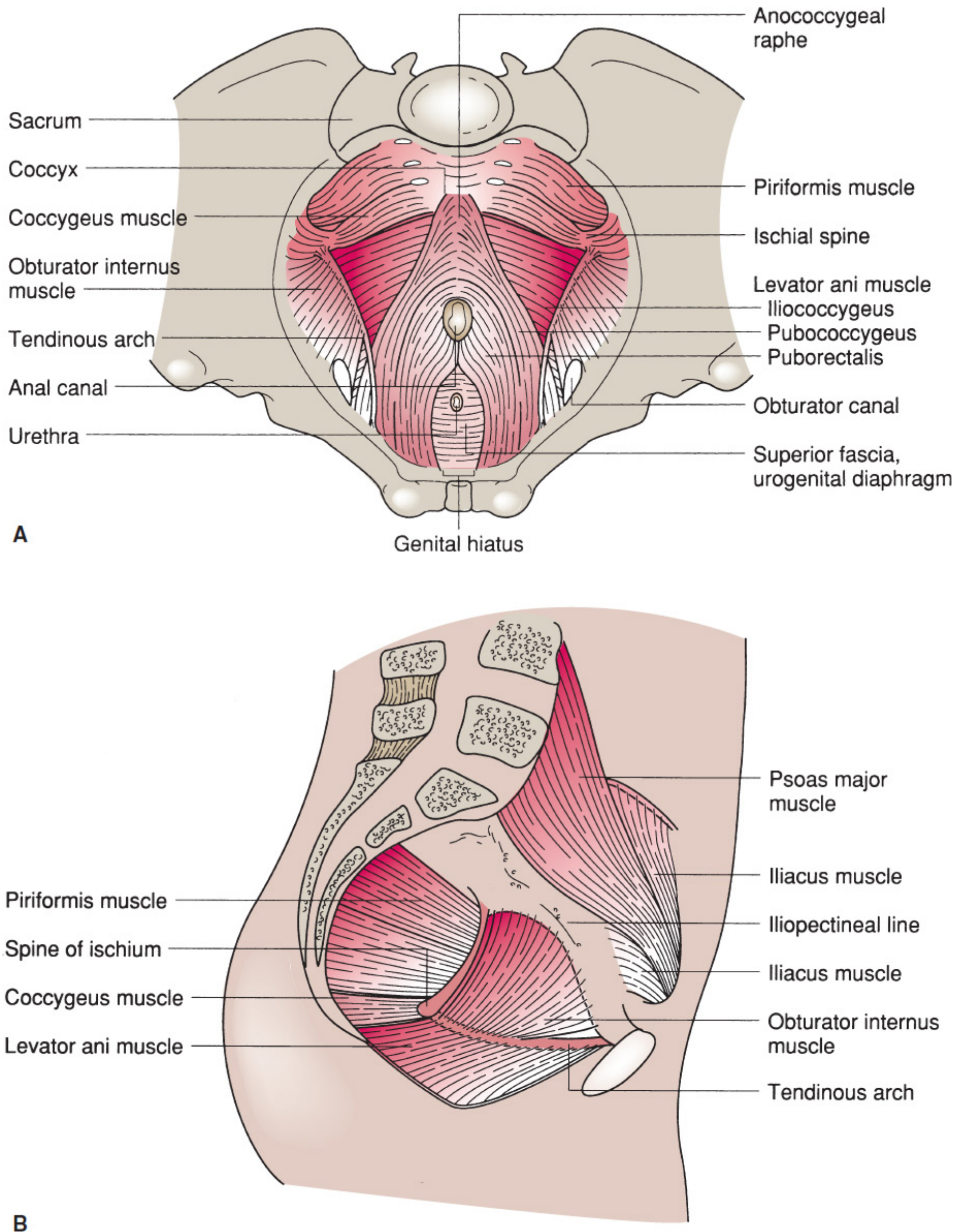
Definition:
The pelvic diaphragm is a musculofascial hammock/funnel that forms the floor of the pelvic cavity. It supports the pelvic organs and controls sphincters.
Components:
- Levator ani muscle (main component)
- Coccygeus muscle
- Superior and inferior fasciae covering them
Levator Ani Muscle - Three Parts:
The levator ani is a broad, thin sheet of muscle with three named parts:
| Part | Origin | Insertion | Key Function |
|---|---|---|---|
| Pubococcygeus | Posterior aspect of pubic body + tendinous arch | Anococcygeal raphe + coccyx | Supports pelvic viscera; elevates pelvic floor |
| Puborectalis | Posterior pubis | Loops behind the rectum (puborectal sling) | Forms anorectal angle; maintains continence; most important for fecal continence |
| Iliococcygeus | Tendinous arch of levator ani (on obturator internus fascia) + ischial spine | Anococcygeal raphe + coccyx | Closes pelvic outlet |
Tendinous Arch of Levator Ani:
A thickened band of obturator internus fascia running from the back of the pubis to the ischial spine - the attachment line for iliococcygeus and pubococcygeus
Genital Hiatus (Urogenital Hiatus):
An anteriomedian gap in the levator ani through which:
- In females: Urethra, vagina
- In males: Urethra pass out of the pelvis
Anococcygeal Raphe/Body:
A fibromuscular mass between the anal canal and the coccyx where the posterior fibers of levator ani converge
Coccygeus (Ischiococcygeus):
- Origin: Ischial spine
- Insertion: Lateral margins of coccyx and S5
- Nerve: S4, S5
- Action: Supports pelvic floor; pulls coccyx forward after defecation
Nerve Supply of Pelvic Floor:
- Levator ani: Nerve to levator ani (branches of S3, S4) from above + perineal branches of pudendal nerve from below
- Coccygeus: S4, S5
Functions of the Pelvic Floor:
- Supports abdominal and pelvic organs against gravity and raised intraabdominal pressure
- Maintains urinary and fecal continence (sphincter function)
- Controls the genital hiatus (important in childbirth)
- Resists peristaltic pressures
Clinical Relevance of Pelvic Floor:
- Pelvic floor weakness (after childbirth, in multiparous women) → uterine prolapse, cystocele, rectocele, stress urinary incontinence
- Puborectalis dysfunction → loss of anorectal angle → fecal incontinence
- Pudendal nerve injury during delivery → damage to external anal and urethral sphincters
TOPIC 8: Perineum
The perineum is the region below the pelvic floor, between the thighs.
Boundaries (Diamond-shaped):
- Anteriorly: Pubic symphysis
- Posteriorly: Tip of coccyx
- Laterally: Ischial tuberosities
- Sides: Ischiopubic rami (anterior) and sacrotuberous ligaments (posterior)
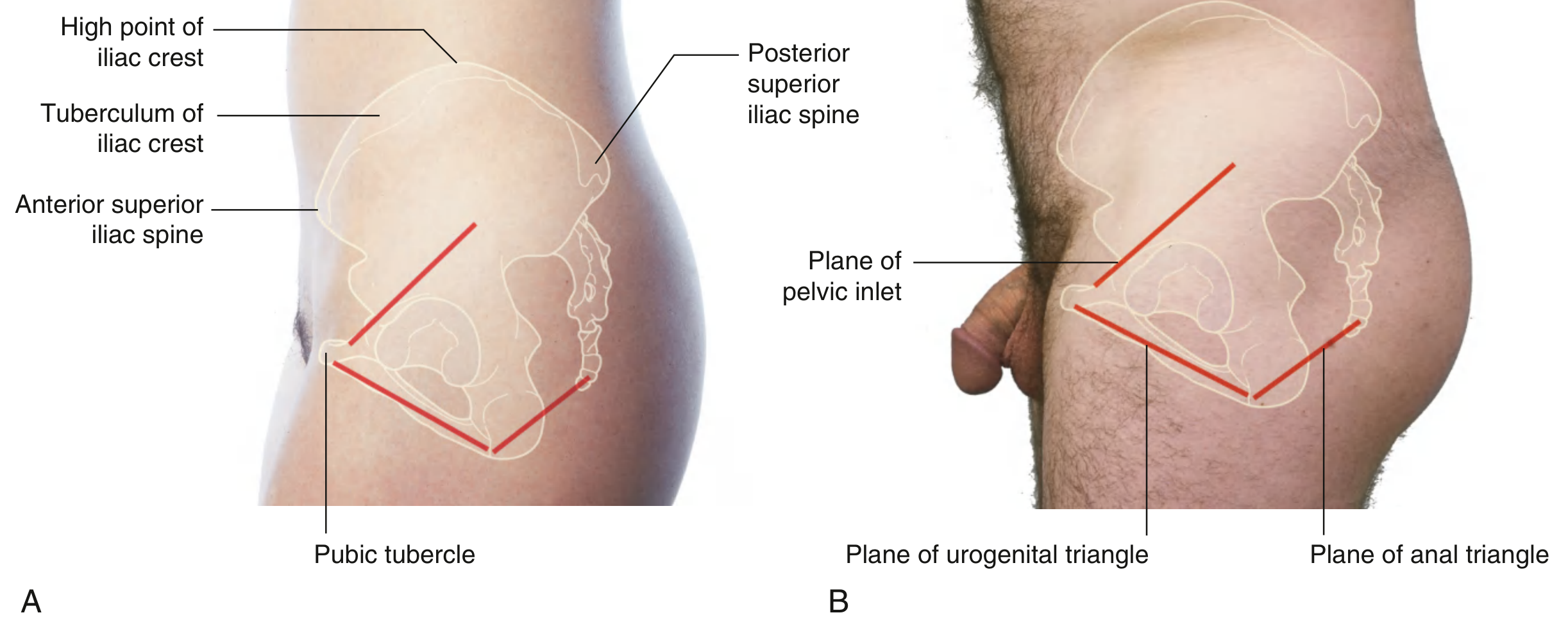
Division of Perineum:
A line drawn between the two ischial tuberosities divides the perineum into:
- Anterior - Urogenital triangle (nearly horizontal, faces inferiorly)
- Posterior - Anal triangle (more vertical, faces posteriorly)
Urogenital Triangle:
Contains:
- External genitalia (penis + scrotum in males; vulva in females)
- External urethral opening
- In females: Vaginal opening (introitus)
Anal Triangle:
Contains:
- Anal canal and anus
- Ischiorectal (ischoanal) fossae on each side
Ischiorectal (Ischoanal) Fossa:
- Wedge-shaped fat-filled space on each side of the anal canal
- Boundaries:
- Medially: External anal sphincter + levator ani
- Laterally: Obturator internus muscle and its fascia
- Roof: Pelvic floor (levator ani)
- Base: Skin
- Contents:
- Ischiorectal fat (allows distension during defecation)
- Pudendal nerve and internal pudendal vessels (in pudendal canal on lateral wall)
- Inferior rectal nerve and vessels
- Clinical: Common site of perianal/ischiorectal abscess; the two fossae communicate behind the anal canal through the postanal space - abscess can track from side to side creating a horseshoe abscess
Pudendal Canal (Alcock's Canal):
- A fascial canal within the lateral wall of the ischiorectal fossa
- Formed by splitting of the obturator internus fascia
- Contents: Pudendal nerve + internal pudendal artery and vein
- Pudendal nerve block is given here for perineal anesthesia during episiotomy
TOPIC 9: Pudendal Nerve
The pudendal nerve (S2, S3, S4) is the main nerve of the perineum and the most important nerve in the pelvis for MBBS exams.
Course:
- Arises from the sacral plexus (S2, S3, S4)
- Exits pelvis through the infrapiriform part of greater sciatic foramen
- Crosses behind the ischial spine and sacrospinous ligament
- Re-enters the perineum through the lesser sciatic foramen
- Runs forward in the pudendal canal (Alcock's canal) on the lateral wall of the ischiorectal fossa
Branches:
- Inferior rectal nerve - supplies external anal sphincter, anal skin, perianal skin
- Perineal nerve - supplies perineal muscles + scrotal/labial skin
- Dorsal nerve of penis/clitoris - sensory to glans penis/clitoris
Mnemonic: "Pudendal = S2, S3, S4"
Clinical:
- Pudendal nerve block: Needle directed to the ischial spine - used in obstetric procedures
- Pudendal nerve injury in childbirth → fecal and urinary incontinence
TOPIC 10: Pelvic Viscera
A. Urinary Bladder
Position: Lies in the anterior part of the lesser pelvis, posterior to the pubic symphysis
Parts:
- Apex - anterosuperiorly (connected to umbilicus by median umbilical ligament = obliterated urachus)
- Body
- Base (fundus) - posteroinferiorly
- Neck - at the bottom, continuous with urethra; in contact with prostate in males
Trigone:
- Triangular smooth area on the posterior wall of the bladder
- Boundaries: Two ureteric orifices (posterolateral corners) + urethral orifice (anterior apex)
- The interureteric crest/ridge runs between the two ureteric orifices
- Trigone is always smooth (no rugae) because it is formed from incorporated mesonephric duct tissue (different embryological origin)
- Clinically important: Tumors tend to occur here; first area examined on cystoscopy
Relations:
In males:
- Anteriorly: Pubic symphysis (retropubic space/cave of Retzius between them)
- Posteriorly: Seminal vesicles, vas deferens, rectum
- Inferiorly: Prostate gland
In females:
- Posteriorly: Uterus and vagina (vesico-uterine pouch between bladder and uterus)
- Inferiorly: Pelvic floor
Blood Supply:
- Superior vesical artery (from patent part of umbilical artery = internal iliac)
- Inferior vesical artery (males) / Vaginal artery (females) - from internal iliac
Nerve Supply:
- Parasympathetic (S2-S4) via pelvic splanchnic nerves - contracts detrusor, relaxes sphincter = micturition
- Sympathetic (T10-L2) via hypogastric plexus - fills bladder (relaxes detrusor, contracts sphincter = continence)
- Somatic: Pudendal nerve (S2-S4) - controls external urethral sphincter
B. Urethra
Male Urethra (~20 cm long):
| Part | Length | Features |
|---|---|---|
| Preprostatic | 1 cm | From bladder neck to prostate - contains internal urethral sphincter |
| Prostatic | 3 cm | Passes through prostate; seminal colliculus (verumontanum) with ejaculatory duct orifices open here; prostatic utricle in midline |
| Membranous | 1-2 cm | Passes through urogenital diaphragm (external urethral sphincter) - shortest, least dilatable, most vulnerable to rupture |
| Spongy (penile) | ~15 cm | Runs in corpus spongiosum; Bulbourethral (Cowper's) gland ducts open here; navicular fossa near external meatus |
Two bends in male urethra:
- Subclavicular bend (at junction of membranous and penile) - fixed
- Puboprostatic bend - can be straightened during catheterization
Three dilatations: Prostatic, bulb of urethra, navicular fossa
Three constrictions (narrowings): Internal urethral meatus, membranous urethra, external urethral meatus
Female Urethra (~4 cm): Short and straight; runs from bladder neck to external urethral orifice (anterior to vaginal opening); passes through urogenital diaphragm
Clinical: Female urethra being short explains the higher frequency of UTIs in females.
C. Rectum and Anal Canal
Rectum (~12 cm):
- Continuous with sigmoid colon at S3
- Three lateral flexures (curvatures): Right, Left, Right
- Three internal transverse folds (Houston's valves/rectal valves) correspond to the lateral flexures
- No mesentery, no haustrations, no taeniae coli (unlike colon)
- Ends at the anorectal junction (anorectal flexure), held by puborectalis sling
Anorectal angle:
- ~90° between rectum and anal canal, maintained by puborectalis sling
- When puborectalis relaxes during defecation, the angle straightens to ~130° allowing passage of feces
Anal Canal (~4 cm, below pelvic floor):
Divided into upper (endodermal) and lower (ectodermal) halves by the pectinate (dentate) line:
| Feature | Above Pectinate Line | Below Pectinate Line |
|---|---|---|
| Embryological origin | Endoderm (hindgut) | Ectoderm (proctodeum) |
| Epithelium | Columnar/transitional | Stratified squamous |
| Anal columns | Present (columns of Morgagni) | Absent |
| Lymphatics drain to | Internal iliac nodes | Superficial inguinal nodes |
| Venous drainage | Portal system (superior rectal) | Systemic (inferior rectal) |
| Arterial supply | Superior rectal (IMA) | Inferior rectal (pudendal) |
| Pain sensation | Visceral - poorly localized | Somatic - well localized, sharp |
Clinical significance of pectinate line:
- Internal hemorrhoids: Above pectinate line (painless, bleed)
- External hemorrhoids: Below pectinate line (painful, rarely bleed)
- Carcinoma above line: Spreads to internal iliac nodes
- Carcinoma below line: Spreads to inguinal nodes
Sphincters of Anal Canal:
- Internal anal sphincter (IAS): Involuntary (smooth muscle); thickened circular layer; innervated by autonomic nerves; maintains resting tone (~80% of resting anal pressure)
- External anal sphincter (EAS): Voluntary (skeletal muscle); three parts (subcutaneous, superficial, deep); innervated by inferior rectal nerve (branch of pudendal, S2-S4); important for voluntary control
D. Prostate Gland
- Male accessory sex gland, size of a walnut (4 x 3 x 2 cm; weight ~20g)
- Located below the bladder neck, surrounding the prostatic urethra
Lobes:
- Traditionally described: Anterior, Posterior, Two lateral lobes, Middle (median) lobe
- McNeal's zones:
- Peripheral zone (70%): Most gland; site of carcinoma and prostatitis
- Transition zone (5-10%): Surrounds urethra; site of BPH (benign prostatic hyperplasia)
- Central zone (25%): Around ejaculatory ducts
Relations:
- Superior: Bladder neck
- Inferior: Urogenital diaphragm / pelvic floor
- Anterior: Puboprostatic ligaments, retropubic space
- Posterior: Rectum (separated by Denonvilliers' fascia/rectovesical septum)
- On each side: Levator ani
Blood Supply: Inferior vesical + middle rectal arteries (from internal iliac)
Nerve supply:
- Parasympathetic (S2-S4): Secretomotor
- Sympathetic (T10-L2): Smooth muscle contraction (ejaculation)
Digital rectal exam (DRE): Posterior surface of prostate felt through anterior rectal wall; median sulcus felt in normal prostate; obliterated sulcus suggests cancer or BPH
E. Uterus
Shape and size: Pear-shaped; ~7.5 x 5 x 3 cm in adult
Parts:
- Fundus - dome above uterine tubes
- Body (corpus) - main part; uterine tubes enter at uterine cornu
- Isthmus - narrow part between body and cervix; becomes the lower uterine segment in pregnancy
- Cervix - lower cylindrical part; internal os (above) and external os (below); projects into vagina
Cavity: Triangular; lined by endometrium
Wall: Thick; middle layer = myometrium (smooth muscle)
Peritoneal covering:
- Anteriorly: Covers only the body (not the cervix)
- Posteriorly: Covers fundus, body, and upper cervix, then reflects onto rectum forming the Pouch of Douglas (recto-uterine pouch) - the most dependent part of the peritoneal cavity in females
Position of Uterus:
| Term | Meaning |
|---|---|
| Anteflexed | Body of uterus bent forward on cervix (normal) |
| Anteverted | Cervix bent forward on vagina (normal) - angle ~90° |
| Retroflexed | Body bent backward on cervix |
| Retroverted | Cervix bent backward on vagina |
Normal uterus is anteverted and anteflexed
Ligaments of Uterus:
| Ligament | Attachment | Function |
|---|---|---|
| Broad ligament | Lateral pelvic walls | Peritoneal fold; contains uterine tube, round ligament, ovarian ligament, vessels; NOT the main support |
| Round ligament | Uterine cornu → inguinal canal → labium majus | Maintains anteflexion; passes through inguinal canal (equivalent of gubernaculum testis) |
| Uterosacral ligaments | Cervix → sacrum | Main support; maintains retroversion if weak |
| Cardinal (Mackenrodt's/transverse cervical) ligaments | Cervix and upper vagina → lateral pelvic walls | Most important support of uterus; contains uterine artery |
| Pubocervical ligaments | Cervix → pubis | Support anteriorly |
Key exam point: The Cardinal (Mackenrodt's) ligament is the most important support of the uterus. Its weakness leads to uterine prolapse.
Blood Supply of Uterus:
- Uterine artery (main) - branch of internal iliac
- Ovarian artery - from aorta
- Important relation: The uterine artery crosses above the ureter at the base of the broad ligament, at the level of the cervix ("water under the bridge"). This is the landmark to avoid during hysterectomy - the ureter can be injured.
Lymphatic Drainage:
- Fundus → para-aortic nodes
- Body → iliac nodes
- Cervix → iliac and sacral nodes
F. Ovaries
- Almond-shaped; ~3 x 1.5 x 1 cm
- Located in the ovarian fossa (shallow depression on lateral pelvic wall, between external and internal iliac vessels)
- Not covered by peritoneum - the only pelvic organ not covered by peritoneum; covered by germinal epithelium (simple cuboidal/columnar)
Attachments:
- Mesovarium - posterior fold of broad ligament to hilum (vessels + nerves enter here)
- Ligament of the ovary - from medial pole to uterine cornu
- Suspensory ligament (infundibulopelvic ligament) - from lateral pole to pelvic brim; contains ovarian vessels and nerves
Blood Supply: Ovarian arteries from aorta at L2 (directly, not from internal iliac)
TOPIC 11: Blood Supply of the Pelvis
Internal Iliac Artery (Hypogastric Artery):
The main artery of the pelvis. Arises from the common iliac artery at L5, in front of the sacroiliac joint.
Divides into Anterior division and Posterior division:
Anterior Division:
Visceral branches:
- Superior vesical artery → bladder (patent part of umbilical artery)
- Inferior vesical artery (males) / Uterine artery (females)
- Obturator artery (sometimes from inferior epigastric - "aberrant obturator artery" = corona mortis)
- Middle rectal artery → rectum
- Vaginal artery (females)
- Internal pudendal artery → perineum (main artery)
Parietal branches:
- Obturator artery
- Inferior gluteal artery → gluteal region (inferior)
Posterior Division:
Parietal branches:
- Iliolumbar artery → iliacus + psoas
- Lateral sacral arteries → sacral canal
- Superior gluteal artery (largest branch of internal iliac) → gluteal region (superior)
Mnemonic for anterior division visceral branches:
"I Slipped, Under My Rug, Visiting Interesting Places"
- Iliolumbar (actually posterior), Superior vesical, Uterine/Inferior vesical, Middle rectal, Renal (no), Vaginal, Internal pudendal, Inferior gluteal (parietal)
Internal Iliac Vein:
Tributaries mirror the branches of the artery. The pelvic venous plexuses (vesical, prostatic, uterine, rectal) drain into the internal iliac vein.
TOPIC 12: Nerve Supply of the Pelvis
Sacral Plexus (L4, L5, S1, S2, S3):
Lies on the piriformis muscle in the posterior pelvic wall.
Major branches:
| Nerve | Roots | Exits | Supplies |
|---|---|---|---|
| Sciatic nerve | L4, L5, S1, S2, S3 | Infrapiriform | Entire lower limb (largest nerve in body) |
| Superior gluteal | L4, L5, S1 | Suprapiriform | Gluteus medius, minimus, tensor fasciae latae |
| Inferior gluteal | L5, S1, S2 | Infrapiriform | Gluteus maximus |
| Pudendal nerve | S2, S3, S4 | Infrapiriform → lesser sciatic | Perineum (see above) |
| Nerve to obturator internus | L5, S1 | Infrapiriform | Obturator internus |
| Posterior cutaneous nerve of thigh | S1, S2, S3 | Infrapiriform | Back of thigh |
| Nerve to levator ani | S3, S4 | Directly through pelvic floor | Levator ani |
| Pelvic splanchnic nerves (nervi erigentes) | S2, S3, S4 | Directly | Parasympathetic to pelvic viscera (micturition, erection, defecation) |
Autonomic Supply of Pelvic Viscera:
| Division | Nerve | Roots | Effect on Bladder | Effect on Rectum | Effect on Sex organs |
|---|---|---|---|---|---|
| Parasympathetic | Pelvic splanchnic (nervi erigentes) | S2, S3, S4 | Contracts detrusor (micturition) | Promotes defecation | Erection ("S2, 3, 4 keeps the floor + erection") |
| Sympathetic | Hypogastric nerve (from superior hypogastric plexus) | T10-L2 | Relaxes detrusor; contracts sphincter (filling) | Relaxes walls | Ejaculation |
Clinically important:
- Injury to pelvic splanchnic nerves (e.g., during AP resection of rectum) → erectile dysfunction + bladder dysfunction
- Sympathetic injury → retrograde ejaculation
Obturator Nerve:
- Arises from lumbar plexus (L2, L3, L4)
- Runs along lateral pelvic wall, exits through obturator canal
- Supplies: Adductor compartment of thigh + skin of medial thigh
- Clinical: Pelvic tumor or ovarian cyst can compress the obturator nerve → pain/numbness along medial thigh; also tender on hip adduction
TOPIC 13: Pelvic Peritoneum and Pouches
The peritoneum descends into the pelvis from the abdominal cavity and drapes over the pelvic viscera, forming clinically important pouches:
In Females (Anterior to Posterior):
- Anterior abdominal wall (median/medial umbilical folds over urachus/umbilical arteries)
- Bladder - peritoneum covers superior + posterior surfaces
- Vesico-uterine pouch - between bladder and uterus (NOT the most dependent pouch)
- Uterus - peritoneum covers anterosuperior body, fundus, posterior body, cervix → becomes broad ligament laterally
- Recto-uterine pouch (Pouch of Douglas) - between uterus + vagina posteriorly and rectum; MOST DEPENDENT part of peritoneal cavity in erect posture in females
- Rectum
In Males (Anterior to Posterior):
- Bladder
- Rectovesical pouch - between bladder and rectum; most dependent peritoneal recess in males
- Rectum
Clinical significance:
- Blood, pus, or peritoneal fluid collect in the Pouch of Douglas in females (ectopic pregnancy rupture, peritonitis)
- Can be drained by posterior colpotomy (needle through posterior vaginal fornix)
- Felt on per vaginal examination (tenderness = pelvic peritonitis)
TOPIC 14: Sacral Plexus - Quick Overview
Formed on the posterior wall of the pelvis (anterior surface of piriformis) by:
- Lumbosacral trunk (L4 + L5)
- Anterior rami of S1, S2, S3 + part of S4
All nerve roots converge into the sciatic nerve (L4-S3), the largest nerve in the body, which exits through the infrapiriform foramen.
Quick Revision Table - HIGH-YIELD EXAM POINTS
| Topic | Key Fact |
|---|---|
| Pelvic brim | Sacral promontory → arcuate line → pectineal line → pubic symphysis |
| Obstetric conjugate | ~11 cm (minimum 10 cm needed for vaginal delivery) |
| Diagonal conjugate | ~12.5 cm (clinically measurable); Obstetric = Diagonal - 1.5 cm |
| Widest pelvic inlet diameter | Transverse (~13 cm) |
| Female vs male subpubic angle | Female >90°, Male <90° |
| Pelvic floor main muscle | Levator ani (pubococcygeus + puborectalis + iliococcygeus) |
| Fecal continence key muscle | Puborectalis (maintains anorectal angle) |
| Pelvic floor nerve supply | S3, S4 (nerve to levator ani) |
| Pudendal nerve roots | S2, S3, S4 (exits infrapiriform, reenters lesser sciatic foramen) |
| Most important uterine support | Cardinal (Mackenrodt's) ligament |
| Uterine artery and ureter | Uterine artery crosses ABOVE ureter at base of broad ligament |
| Most dependent pouch (female) | Pouch of Douglas (recto-uterine pouch) |
| Trigone of bladder | Between 2 ureteric orifices + urethral orifice; smooth, no rugae |
| Pectinate line significance | Portal-systemic junction; internal vs external hemorrhoids |
| Lymph drainage above pectinate line | Internal iliac nodes |
| Lymph drainage below pectinate line | Superficial inguinal nodes |
| Parasympathetic to pelvic viscera | Pelvic splanchnic nerves (S2, S3, S4 = nervi erigentes) - erection |
| Sympathetic to pelvic viscera | Hypogastric nerve (T10-L2) - ejaculation, bladder filling |
| Ovarian artery origin | Directly from aorta at L2 |
| Piriformis exits | Greater sciatic foramen (divides it into suprapiriform and infrapiriform) |
| McNeal zones | BPH = Transition zone; Cancer = Peripheral zone |
| Gynaecoid pelvis | Round inlet, >90° arch - best for delivery (most common = 50%) |
| Alcock's canal contents | Pudendal nerve + internal pudendal artery and vein |
| Ischiorectal fossa clinical | Perianal abscess; horseshoe abscess (via post-anal space) |
All anatomical content sourced from: Gray's Anatomy for Students (9780323934237), General Anatomy and Musculoskeletal System - Thieme Atlas (9781626237186), Mulholland & Greenfield's Surgery (9781975143169), Campbell-Walsh Urology (9780323546423)
This is a shared conversation. Sign in to Orris to start your own chat.