Low grade dysplasia
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"Barrett's esophagus" AND "low grade dysplasia" AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading Article
PMID: 38763697
Here is a thorough overview of low-grade dysplasia (LGD) in Barrett's esophagus, drawn from multiple authoritative GI textbooks and the latest AGA guideline.
Low-Grade Dysplasia in Barrett's Esophagus
What is it?
Low-grade dysplasia (LGD) is one of the histological grades along the metaplasia-dysplasia-adenocarcinoma sequence in Barrett's esophagus. Dysplasia is the histological expression of the genetic and epigenetic changes that favor neoplastic cell growth - specifically the accumulation of mutations (beginning with p53 inactivation) that alter cell morphology in a way pathologists can recognize under the microscope.
Barrett metaplasia is classified into four grades:
- No dysplasia
- Indefinite for dysplasia
- Low-grade dysplasia (LGD)
- High-grade dysplasia (HGD)
- Yamada's Textbook of Gastroenterology, 7e, p. 946
Histopathology
The biopsy image below shows LGD (at 11 o'clock) alongside high-grade dysplasia (center). In LGD, cellular abnormalities are present but less pronounced than HGD - nuclear enlargement, crowding, and loss of normal polarity are seen but confined to the lower portions of the crypts.
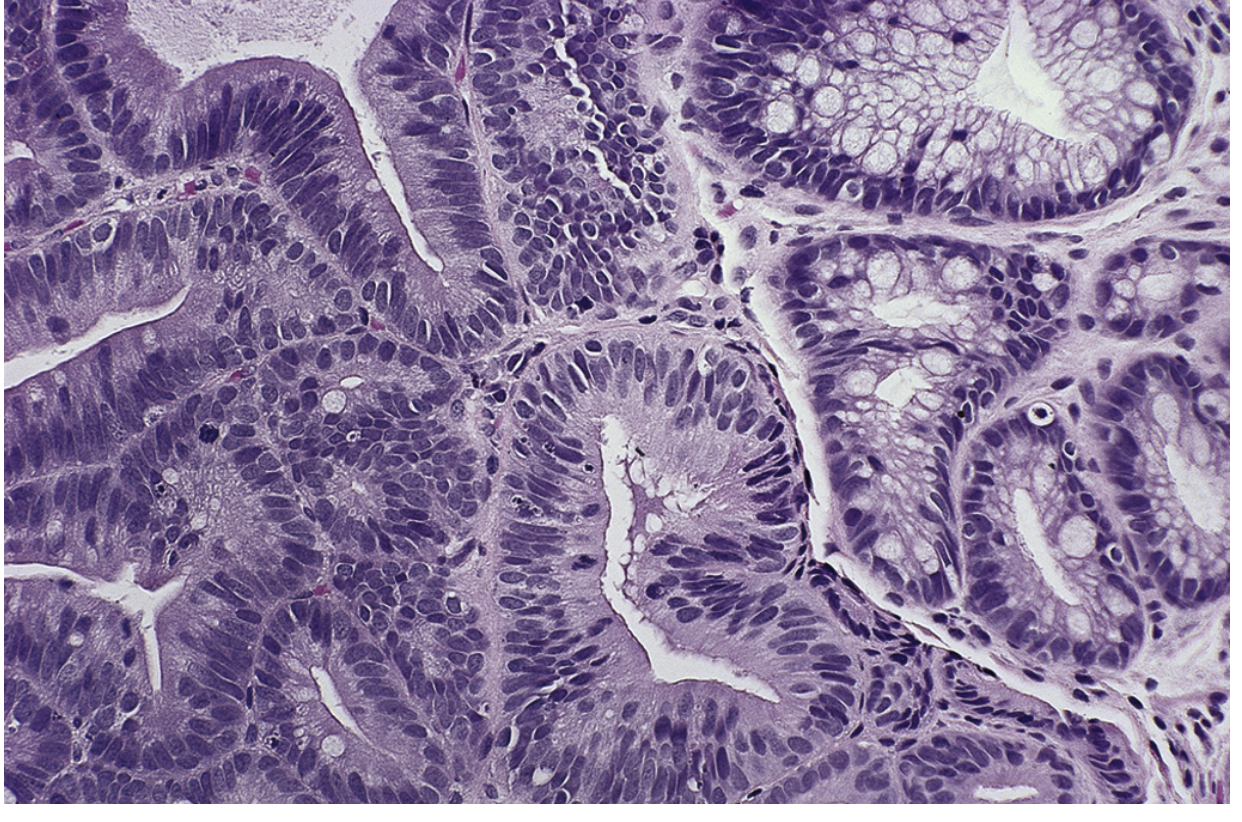
Fig. 47.4 - Sleisenger and Fordtran's GI and Liver Disease
The Diagnostic Challenge
LGD is notoriously difficult to diagnose reliably:
-
Histological changes of LGD can closely mimic reactive/regenerative changes from reflux esophagitis.
-
Interobserver agreement among pathologists is poor (<50%) for LGD.
-
A landmark Netherlands study found community pathologists diagnosed LGD, but expert GI pathologists confirmed it in only 15% of cases. However, in those confirmed cases, the cumulative risk of neoplastic progression reached 85% at 9 years.
-
By contrast, an American study of 210 LGD patients found progression of only 0.4% per year, with no association between diagnostic consensus and progression.
-
Because of this diagnostic variability, expert GI pathologist confirmation is mandatory before acting on an LGD diagnosis.
-
Yamada's Textbook of Gastroenterology, 7e, p. 946; Sleisenger and Fordtran's GI and Liver Disease
Natural History & Risk of Progression
| Finding | Annual Progression Risk |
|---|---|
| Non-dysplastic Barrett esophagus | ~0.25% per year to adenocarcinoma |
| Development of LGD from non-dysplastic BE | ~4.3% per year |
| LGD to adenocarcinoma | Variable: 0.4% (US data) to very high in confirmed cases |
| High-grade dysplasia to adenocarcinoma | ~6% per year |
The overall annual risk of progression from Barrett esophagus to esophageal adenocarcinoma is 0.29%, and the risk is significantly higher in patients who already have LGD at baseline.
- Mulholland and Greenfield's Surgery, 7e, p. 2066; Sleisenger and Fordtran's
Management
Step 1 - Confirm the diagnosis
Expert GI pathologist review is mandatory. If the diagnosis is "indefinite for dysplasia," give PPI therapy at 60-80 mg for 3 months and rebiopsy - severe inflammation makes histological interpretation unreliable.
Step 2 - Endoscopic evaluation
Any patient with dysplasia requires careful high-definition white-light endoscopy (HD-WLE). The Seattle biopsy protocol (4-quadrant biopsies every 1-2 cm) is standard but has real sampling limitations. Any visible mucosal irregularity, nodule, or ulceration should be removed by EMR (endoscopic mucosal resection) for histological staging before ablation.
Step 3 - Treatment decision
Endoscopic Eradication Therapy (EET) is the procedure of choice for LGD once the diagnosis is confirmed.
| Option | Role in LGD |
|---|---|
| Radiofrequency ablation (RFA) | Preferred ablation modality; can eradicate nearly 100% of LGD. Recommended to ablate all remaining Barrett metaplasia after any visible lesions are resected. |
| EMR | For any visible lesions; provides staging information; now considered mandatory before ablation in most guidelines |
| Surveillance endoscopy (every 6-12 months) | Acceptable alternative for patients who place higher value on avoiding procedure-related harms; shared decision making required |
| Nissen fundoplication | A reasonable alternative in selected patients - evidence shows LGD reverts to non-dysplastic intestinal metaplasia after fundoplication in most cases |
| Esophagectomy | Reserved for rare cases where EET fails; not recommended as primary treatment |
The 2024 AGA Clinical Practice Guideline (Rubenstein et al., Gastroenterology 2024) made a conditional recommendation in favor of EET in BE with LGD. Importantly, patients who place higher value on avoiding potential harms (esophageal stricture ~5.6%, bleeding ~1%, perforation ~0.6%) could reasonably choose endoscopic surveillance instead - shared decision making is central.
The 2025 AGA Surveillance Guideline (PMID: 41125322) further refines surveillance intervals for Barrett's esophagus.
EET Complications (RFA ± EMR)
From a systematic review of 9,200 patients:
-
Esophageal stricture: 5.6%
-
Bleeding: 1%
-
Perforation: 0.6%
-
Overall serious adverse events: 8.8%
-
Risk is significantly higher when RFA is combined with EMR (relative risk 4.4)
-
Sleisenger and Fordtran's GI and Liver Disease
Key Points Summary
- LGD diagnosis requires expert pathologist confirmation due to high rate of overdiagnosis.
- Once confirmed, LGD carries a meaningfully elevated cancer risk compared to non-dysplastic Barrett esophagus.
- EET (RFA ± EMR) is the preferred treatment for confirmed LGD - AGA 2024 gives a conditional recommendation in its favor.
- Surveillance endoscopy every 6-12 months is a reasonable alternative for patients who prefer it, through shared decision making.
- All residual Barrett metaplasia should be ablated after resection of visible lesions to reduce metachronous neoplasia.
- PPI therapy is maintained for acid suppression/chemoprevention throughout management.
This is a shared conversation. Sign in to Orris to start your own chat.