Uti ,hematuria,urinary catheterization,uterine stone, prostate cancer ,bladder cancer , diffrence between bph and prostate cancer with detail information
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
All topics have been covered in detail above. Here is a quick summary of what was addressed:
Topics Covered:
-
UTI - Definition, pathogens, lower vs upper tract features, diagnosis, treatment (including pregnancy-specific management).
-
Hematuria - Gross vs microscopic, clinical significance (up to 25% signal cancer), pseudohematuria, localizing the source by stream timing and clot shape, evaluation protocol.
-
Urinary Catheterization - Types (intermittent, indwelling Foley, suprapubic), indications, technique tips, and complications (especially CAUTI).
-
Urinary Stones - Types (calcium oxalate most common; struvite/staghorn; uric acid; cystine), clinical features (renal colic), diagnosis (CT KUB gold standard), and management.
-
Prostate Cancer - Epidemiology, risk factors, Gleason grading, PSA screening, diagnosis, and treatment by stage.
-
Bladder Cancer - Epidemiology, risk factors (smoking #1), pathology (90% urothelial), symptoms (painless hematuria), diagnosis (cystoscopy + biopsy), and treatment by stage.
-
BPH vs Prostate Cancer (detailed) - A full side-by-side comparison covering zone of origin, DRE findings, PSA, symptoms, metastasis, histology, and treatment - with two clinical diagrams from Bailey and Love's Surgery.
Make OSCE cases on all this disease and which one is most possible asked in OSCE exam
Searching the Web
most common OSCE exam questions urology UTI hematuria BPH prostate cancer bladder cancer
Here are fully structured OSCE cases for every topic, followed by a ranking of which are most likely to appear in your exam.
OSCE Cases - Urology & Genitourinary Medicine
🏆 OSCE Frequency Ranking (Most to Least Likely)
| Rank | Topic | Why It's Commonly Asked |
|---|---|---|
| 🥇 1 | UTI (especially in young woman / pregnant woman) | Most common urological condition; tests history, diagnosis AND management |
| 🥇 1 | BPH vs Prostate Cancer (elderly man with LUTS) | Classic OSCE differentials; DRE, PSA interpretation, counselling |
| 🥈 2 | Painless Hematuria (bladder cancer work-up) | "Red flag" presentation; tests investigation pathway |
| 🥈 2 | Renal/Ureteral Stone (renal colic) | Classic emergency presentation; tests diagnosis and management |
| 🥉 3 | Prostate Cancer (PSA counselling / staging) | Communication OSCE favourite; shared decision-making |
| 🥉 3 | Bladder Cancer (history + cystoscopy explanation) | Hematuria work-up; investigations |
| 4 | Urinary Catheterization (practical station) | Common practical skills station |
CASE 1 - UTI in a Young Woman ⭐⭐⭐ (HIGHEST YIELD)
Station Instructions (to student)
You have 8 minutes. A 24-year-old woman presents to the GP with a 2-day history of burning pain on urination. Take a focused history, order relevant investigations, and outline your management.
Simulated Patient Script
Name: Sarah, 24 years old, office worker
Presenting complaint: "It burns when I pee, and I keep needing to go every 20 minutes."
History to reveal when asked:
- Dysuria for 2 days (burning, stinging)
- Urinary frequency - going every 20-30 minutes
- Urgency - has to rush to the toilet
- Suprapubic discomfort
- No fever, no back/flank pain, no nausea/vomiting
- No vaginal discharge, no external burning (rules out vulvovaginitis)
- Sexually active, new partner 1 week ago
- Last menstrual period: 2 weeks ago, regular cycles
- Not pregnant
- No allergies
- No previous UTIs
- No medical history
Mark Scheme
| Task | Marks |
|---|---|
| Introduces self, gains consent | 1 |
| Asks about dysuria, frequency, urgency | 1 |
| Asks about fever, loin pain (rule out pyelonephritis) | 1 |
| Asks about vaginal discharge / external burning (differential) | 1 |
| Takes sexual history appropriately | 1 |
| Rules out pregnancy | 1 |
| Asks about previous UTIs, allergies | 1 |
| Orders urinalysis / dipstick test | 1 |
| Orders MSU (midstream urine) for culture and sensitivity | 1 |
| Correct diagnosis: uncomplicated lower UTI | 1 |
| Correct treatment: e.g. nitrofurantoin 100 mg BD x 5 days | 1 |
| Advises adequate fluid intake, analgesia | 1 |
| Safety net: return if symptoms worsen, fever, or don't improve in 48h | 1 |
Model Answer
Diagnosis: Uncomplicated lower UTI (acute cystitis)
Investigations:
- Urine dipstick: leucocytes + nitrites positive
- MSU for culture and sensitivity (before starting antibiotics if possible)
- Pregnancy test (urine hCG) - to exclude pregnancy before prescribing
Treatment:
- Nitrofurantoin 100 mg modified-release BD for 5 days (first-line)
- Alternative: trimethoprim 200 mg BD for 7 days (if local resistance < 20%)
- Adequate hydration (2L+ water daily)
- Analgesia: paracetamol for suprapubic discomfort
Differentials to mention:
- Urethritis (chlamydia) - especially with new partner
- Vaginitis
- Interstitial cystitis
CASE 2 - UTI in Pregnancy ⭐⭐⭐ (HIGHEST YIELD)
Station Instructions
A 28-year-old woman at 14 weeks gestation attends her antenatal clinic. Her routine urine dipstick shows leucocytes++ and nitrites+. She has NO symptoms. Take a history and manage appropriately.
Key History Points
- Asymptomatic bacteriuria in pregnancy
- No dysuria, no frequency (no symptoms)
- First antenatal visit, 14 weeks pregnant
- No allergies, no previous UTIs in this pregnancy
Mark Scheme
| Task | Marks |
|---|---|
| Recognises this is asymptomatic bacteriuria | 2 |
| Explains risk: 30% will develop pyelonephritis if untreated | 1 |
| Orders MSU for culture | 1 |
| Treats appropriately: cephalexin 500mg BD x 7 days OR nitrofurantoin (avoid 3rd trimester) | 2 |
| Avoids TMP-SMX in 3rd trimester | 1 |
| Explains risk of preterm labour if untreated | 1 |
| Plans test-of-cure (repeat urine culture after treatment) | 1 |
| Safety net and follow-up | 1 |
Key Teaching Point
Asymptomatic bacteriuria in pregnancy MUST be treated because:
- 30% progress to pyelonephritis
- Risk of preterm labour and low birth weight
- USPSTF Grade A recommendation to screen at 12-16 weeks
CASE 3 - Elderly Man with LUTS: BPH vs Prostate Cancer ⭐⭐⭐ (HIGHEST YIELD)
Station Instructions
A 68-year-old man presents with a 6-month history of difficulty urinating. Take a history, perform a relevant examination, interpret investigations, and discuss management. You will be shown a DRE finding and PSA result.
Simulated Patient Script
Name: Mr. James, 68 years old, retired
Presenting complaint: "I've been having trouble with my waterworks for about 6 months."
History to reveal when asked:
- Poor urinary stream, takes time to start
- Intermittent stream (stops and starts)
- Sensation of incomplete emptying
- Nocturia x3 per night (wakes up 3 times)
- No fever, no dysuria, no haematuria
- No bone pain, no weight loss
- No previous urological history
- Father had prostate cancer (age 74)
- Non-smoker, no medications
Investigation Results (shown to student)
| Test | Result | Normal |
|---|---|---|
| PSA | 12.5 ng/mL | < 4.0 ng/mL |
| Free PSA ratio | 8% | > 25% = BPH likely |
| Uroflowmetry | Peak flow 8 mL/s | Normal > 15 mL/s |
| Post-void residual | 180 mL | Normal < 50 mL |
| DRE finding | Hard, irregular nodule on right lobe | Normal = smooth, rubbery |
Mark Scheme
| Task | Marks |
|---|---|
| Systematic LUTS history (voiding + storage symptoms) | 2 |
| Asks about haematuria, bone pain, weight loss (red flags) | 1 |
| Asks family history (prostate cancer risk) | 1 |
| Interprets PSA as significantly elevated | 1 |
| Notes LOW free PSA ratio (< 25% suspicious for cancer) | 1 |
| Interprets DRE correctly as suspicious for cancer (hard, nodular) | 1 |
| Correct differential: prostate cancer > BPH | 1 |
| Orders: TRUS-guided biopsy OR mpMRI of prostate | 1 |
| Mentions bone scan + CT if cancer confirmed | 1 |
| Counsels patient sensitively about findings | 1 |
| Correct referral: urgent urology referral (2-week-wait) | 1 |
Model Answer
Most Likely Diagnosis: Prostate cancer (PSA 12.5, low free PSA ratio, hard nodular DRE)
BPH features that ARE present: Obstructive LUTS, age > 50, poor flow, high post-void residual
Cancer features making this MORE suspicious:
- PSA > 10 ng/mL
- Free:total PSA ratio of 8% (< 25% is suspicious)
- DRE: hard, irregular nodule
Next step: mpMRI prostate followed by TRUS-guided or MRI-targeted biopsy
Staging if confirmed: PSA 12.5 - bone scan + CT abdomen/pelvis
CASE 4 - Painless Hematuria in a 58-Year-Old Smoker ⭐⭐⭐ (HIGH YIELD)
Station Instructions
Mr. Chen, 58 years old, attends A&E with a 1-week history of blood in his urine. He is not in pain. Take a history, order investigations, and explain the most likely diagnosis.
Simulated Patient Script
Name: Mr. Chen, 58-year-old male, factory worker (dye industry for 20 years)
Presenting complaint: "My urine has been red/pink for about a week. It doesn't hurt at all."
History to reveal when asked:
- Painless, total (entire stream) haematuria
- No clots passed
- No dysuria, no fever
- No flank pain
- Smoker: 30 pack-year history
- Occupational exposure: worked in chemical dye factory for 20 years
- No anticoagulants, no recent urological procedures
- No recent trauma
- Weight loss of 4 kg in 2 months
- No family history of urological cancers
Mark Scheme
| Task | Marks |
|---|---|
| Clarifies painless haematuria (key red flag feature) | 1 |
| Asks about clots and their shape | 1 |
| Asks smoking history | 1 |
| Asks occupational history (chemical/dye exposure) | 1 |
| Asks about medications (anticoagulants) | 1 |
| Asks systemic symptoms (weight loss = red flag) | 1 |
| Correct investigations: MSU, urine cytology, FBC, U&E, USS or CT urogram | 2 |
| Identifies cystoscopy + biopsy as definitive investigation | 1 |
| Correct diagnosis: bladder cancer until proven otherwise | 1 |
| Explains findings sensitively to patient | 1 |
| Urgent urology referral | 1 |
Model Answer
Diagnosis: Bladder cancer (transitional cell carcinoma) - until proven otherwise
Red flags present:
- Age > 50 + male gender
- Painless total haematuria
- Heavy smoking history (30 pack-years)
- Chemical dye industry exposure (aromatic amines)
- Weight loss
Investigations:
- Urine dipstick + MSU (exclude UTI first)
- Urine cytology (high specificity for high-grade TCC)
- FBC, U&E, creatinine
- CT urogram (upper tract + bladder)
- Cystoscopy + biopsy = gold standard
Management: TURBT (transurethral resection of bladder tumour) for staging and treatment if superficial; radical cystectomy if muscle-invasive.
CASE 5 - Renal Colic ⭐⭐ (HIGH YIELD)
Station Instructions
A 35-year-old man arrives in A&E in severe pain. Assess and manage him.
Simulated Patient Script
Name: Mr. Ahmed, 35 years old
Presenting complaint: "This is the worst pain I've ever had. It started in my left side and is going into my groin."
History to reveal when asked:
- Sudden onset severe left loin-to-groin pain
- Colicky in nature (comes and goes in waves)
- Pain score 9/10
- Nausea and vomiting
- Cannot find a comfortable position (rolling around)
- Haematuria: pink-tinged urine today
- No fever, no rigors (not infected)
- Not pregnant
- Previous similar episode 2 years ago (passed a stone spontaneously)
- Drinks only 1 glass of water per day, lives in a hot climate
- No medications, no allergies
Mark Scheme
| Task | Marks |
|---|---|
| Correctly identifies loin-to-groin colicky pain | 1 |
| Asks about haematuria | 1 |
| Asks about fever (infected stone = emergency) | 1 |
| Asks about previous stones | 1 |
| Asks about fluid intake and diet | 1 |
| Orders: Urine dipstick (haematuria), urine pregnancy test (female), FBC, U&E, Ca, urate | 2 |
| Orders non-contrast CT KUB as gold standard imaging | 1 |
| Provides adequate analgesia: IV/IM diclofenac (NSAID) + opioid backup | 1 |
| Considers medical expulsive therapy: tamsulosin (alpha-blocker) | 1 |
| Knows when to escalate: fever + obstruction = emergency ureteroscopy + stent | 1 |
| Stone prevention advice | 1 |
Model Answer
Diagnosis: Left ureteral calculus causing renal colic
Investigations:
- Urine dipstick: haematuria (90% of cases)
- Non-contrast CT KUB: gold standard (>95% sensitivity)
- FBC, U&E, calcium, uric acid, creatinine
- Urine culture (if febrile)
- Stone analysis if passed
Management:
- IV/IM diclofenac 75mg (NSAIDs are first-line for analgesia)
- IV morphine if NSAIDs insufficient
- IV hydration
- Tamsulosin 0.4 mg daily (alpha-blocker as medical expulsive therapy for stones < 10mm)
- Stones < 5 mm: 95% pass spontaneously
- Stones 5-10 mm: ureteroscopy or ESWL
- Stones > 10 mm or staghorn: PCNL
Emergency if: fever + obstruction = septic obstructed system → emergency stent/nephrostomy + broad-spectrum IV antibiotics
CASE 6 - Prostate Cancer Counselling / PSA Discussion ⭐⭐ (HIGH YIELD - COMMUNICATION STATION)
Station Instructions
Mr. Thompson, 62 years old, attends for his PSA result. His PSA is 7.2 ng/mL. He has no urinary symptoms. Explain the result and counsel him appropriately. He has previously had a normal PSA of 3.1 one year ago.
Mark Scheme
| Task | Marks |
|---|---|
| Checks patient's identity and confirms he is ready to receive results | 1 |
| Explains what PSA is in lay terms | 1 |
| Explains PSA is elevated at 7.2 (normal < 4.0) and has risen from 3.1 | 1 |
| Explains PSA can be raised by BPH, prostatitis, or cancer | 1 |
| Notes the PSA velocity (rise from 3.1 to 7.2 in 1 year = significant) | 1 |
| Does NOT diagnose cancer (PSA alone is not diagnostic) | 1 |
| Explains need for further investigation: DRE + mpMRI + possible biopsy | 1 |
| Explains biopsy procedure simply (TRUS-guided or MRI-targeted) | 1 |
| Acknowledges patient's concerns/anxiety | 1 |
| Explains the range of outcomes and that many prostate cancers are slow-growing | 1 |
| Arranges urgent urology referral | 1 |
Key Phrases to Use
- "A raised PSA can be caused by several things - an enlarged prostate, inflammation, or in some cases a cancer. We need more tests to find out which is causing this."
- "This test on its own does not tell us you have cancer."
- "We are going to refer you to a specialist - a urologist - who will arrange a scan and possibly a biopsy of the prostate."
CASE 7 - Urinary Catheterization Practical Station ⭐⭐ (PRACTICAL SKILLS)
Station Instructions
You are asked to perform male urethral catheterization on a manikin. The patient is a 70-year-old man with acute urinary retention.
Mark Scheme
| Step | Marks |
|---|---|
| Introduces self, checks patient identity | 1 |
| Explains procedure and gains verbal consent | 1 |
| Gathers equipment: catheter (14-16 Fr), catheter bag, sterile drape, cleaning solution, sterile gloves, 10mL syringe of sterile water, anaesthetic gel (lidocaine 2%) | 1 |
| Positions patient supine with legs flat | 1 |
| Washes hands, applies sterile gloves | 1 |
| Cleans glans penis with antiseptic, retracts foreskin | 1 |
| Applies anaesthetic gel into urethra, waits 3-5 minutes | 1 |
| Inserts catheter gently until urine flows freely | 1 |
| Inflates balloon with 10 mL sterile water ONLY AFTER urine drains freely | 1 |
| Gently retracts catheter until resistance felt (balloon at bladder neck) | 1 |
| Connects catheter to drainage bag | 1 |
| Replaces foreskin (prevents paraphimosis) | 1 |
| Documents size of catheter and residual volume | 1 |
| Disposes sharps safely | 1 |
Common Mistakes in OSCE
- ❌ Inflating the balloon before urine drains (causes urethral trauma)
- ❌ Forgetting to replace foreskin
- ❌ Not using anaesthetic gel (lidocaine) especially in men
- ❌ Incorrect catheter size (14-16 Fr standard; 12 Fr if urethral stricture suspected)
- ❌ Using a curved Coude tip for BPH without documentation
CASE 8 - Upper UTI / Pyelonephritis ⭐⭐ (HIGH YIELD)
Station Instructions
A 26-year-old woman presents to A&E with 3 days of fever, right loin pain, and vomiting. Take a history and manage her.
Simulated Patient Script
- Fever 38.9°C, rigors
- Right-sided loin/flank pain - constant ache
- Nausea and vomiting, unable to keep fluids down
- Dysuria and frequency started 5 days ago (lower UTI preceded upper UTI)
- No haematuria
- Sexually active, using contraceptive pill, not pregnant
- No previous UTIs
- No allergies
Mark Scheme
| Task | Marks |
|---|---|
| Identifies upper UTI / pyelonephritis correctly | 1 |
| Asks about antecedent lower UTI symptoms | 1 |
| Checks pregnancy status | 1 |
| Orders: MSU, blood cultures (if febrile/septic), FBC, CRP, U&E, creatinine | 2 |
| Imaging: renal ultrasound (to exclude abscess or obstruction) | 1 |
| IV access, IV fluids, antiemetics | 1 |
| IV ceftriaxone 1g daily (or IV ciprofloxacin) | 1 |
| Hospital admission | 1 |
| Step down to oral antibiotics when afebrile and tolerating fluids | 1 |
| Total antibiotic course: 10-14 days | 1 |
Overall OSCE Tips for These Topics
The "Spot Diagnosis" Clues to Memorize
| Clue in Stem | Think |
|---|---|
| Young woman + dysuria + frequency + no fever | Lower UTI / cystitis |
| Young woman + fever + loin pain + dysuria | Pyelonephritis |
| Pregnant woman + positive dipstick + NO symptoms | Asymptomatic bacteriuria - TREAT |
| Elderly man + LUTS + smooth rubbery prostate + PSA 3.5 | BPH |
| Elderly man + LUTS + hard nodular prostate + PSA > 10 + low free PSA | Prostate cancer |
| Middle-aged man + painless total haematuria + smoker | Bladder cancer until proven otherwise |
| Young adult + severe loin-to-groin pain + cannot keep still + haematuria | Renal colic / ureteral stone |
| 70-year-old man + unable to pass urine + distended bladder | Acute urinary retention (likely BPH) |
| Elderly man + haematuria + obstructive LUTS + bone pain + raised ALP | Metastatic prostate cancer |
What Examiners Are Looking For
- Red flag recognition: painless haematuria, weight loss, bone pain, PSA > 10 = urgent referral
- Differentiating BPH vs cancer: DRE findings + PSA + free PSA ratio
- Safe prescribing: correct antibiotic, correct dose, correct duration, check for contraindications (e.g. TMP-SMX in 3rd trimester pregnancy)
- Communication: breaking bad news, PSA counselling, explaining cystoscopy or biopsy
- Investigations in the right order: dipstick → MSU → imaging → endoscopy/biopsy
- Safety netting: always tell patients when to come back urgently
All clinical content sourced from Campbell Walsh Wein Urology, Bailey and Love's Surgery, Rosen's Emergency Medicine, and Textbook of Family Medicine.
1.Renal colic lab test to order and treatment option
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive textbook data. Here is the full detailed answer.
Renal Colic - Complete Lab Tests & Treatment Options
Pathophysiology (Quick Recap)
Renal colic occurs when a stone obstructs the ureter, causing sudden increased pressure in the collecting system, ureteral spasm, and intense colicky pain radiating from loin to groin. The pain is due to ureteral smooth muscle spasm and capsular distension - not peristalsis of the bowel, which is why the patient is restless and cannot find a comfortable position.
PART 1 - LABORATORY INVESTIGATIONS
A. Immediate / Emergency Labs (Every Patient with Renal Colic)
| Test | What You're Looking For | Clinical Significance |
|---|---|---|
| Urine dipstick | Haematuria (blood), leucocytes, nitrites | Blood in 90% of stone cases; leucocytes + nitrites = infection |
| Urine microscopy (MSU) | RBCs, WBCs, casts, bacteria, crystals | Confirms haematuria; crystal type hints at stone type |
| Urine culture | Bacterial growth + sensitivities | MANDATORY if fever present - infected obstruction = emergency |
| Urine pH | pH value | pH > 7.0 = struvite or urea-splitting bacteria; pH < 5.5 = uric acid stones |
| Serum creatinine + eGFR | Renal function | Obstruction can acutely impair function; baseline for monitoring |
| Serum electrolytes (Na, K, Cl, HCO₃) | Electrolyte balance | Especially if vomiting + dehydrated |
| FBC (Full Blood Count) | WBC count | Leukocytosis suggests infection; anaemia if haematuria severe |
| Serum calcium | Hypercalcaemia | High calcium → calcium stone formation (hyperparathyroidism, sarcoidosis) |
| Serum uric acid | Hyperuricaemia | Elevated in gout → uric acid stones |
| CRP / ESR | Inflammatory markers | Elevated if associated infection; helps assess sepsis severity |
| Coagulation screen (INR/PT) | Bleeding risk | Before any interventional procedure |
| Pregnancy test (urine βhCG) | Pregnancy | MANDATORY in all women of childbearing age before CT scan |
B. Extended / Metabolic Workup (For Recurrent Stones, First Stone in Young Patient, Bilateral Stones, Family History)
This is done after the acute episode resolves, on the patient's normal outpatient diet. Do NOT collect 24-hour urine during the acute hospitalization.
| Test | What You're Looking For |
|---|---|
| Serum PTH (parathyroid hormone) | Primary hyperparathyroidism → hypercalciuria → calcium stones |
| Serum phosphate | Low in hyperparathyroidism |
| Serum magnesium | Low magnesium reduces citrate excretion |
| Serum vitamin D (25-OH) | Excessive vitamin D → hypercalcaemia → calcium stones |
| Thyroid function (TFTs) | Hyperthyroidism can cause hypercalciuria |
| Passed stone analysis | Definitive stone type - guides prevention |
24-Hour Urine Collection (Comprehensive Stone Screen)
Measures: Volume, pH, Calcium, Sodium, Phosphate, Uric acid, Citrate, Oxalate, Cystine
| Urine Finding | Implication | Stone Type |
|---|---|---|
| High calcium (> 200 mg/day) | Hypercalciuria | Calcium oxalate/phosphate |
| Low citrate | Hypocitraturia | Calcium oxalate |
| High oxalate | Hyperoxaluria | Calcium oxalate |
| High uric acid | Hyperuricosuria | Uric acid or calcium oxalate |
| Low volume (< 1.5 L/day) | Concentrated urine | All stone types |
| High cystine | Cystinuria (genetic) | Cystine stones |
| Alkaline pH (>7) + ammonia | Urease-producing bacteria | Struvite stones |
C. Crystal Morphology on Urine Microscopy (Quick Reference)
| Crystal Type | Appearance | Stone Type |
|---|---|---|
| Envelope / dumbbell shaped | Calcium oxalate dihydrate | Calcium oxalate |
| Coffin lid shaped | Struvite (triple phosphate) | Struvite / infection stones |
| Rhomboid / needle shaped | Uric acid | Uric acid |
| Hexagonal | Cystine | Cystine |
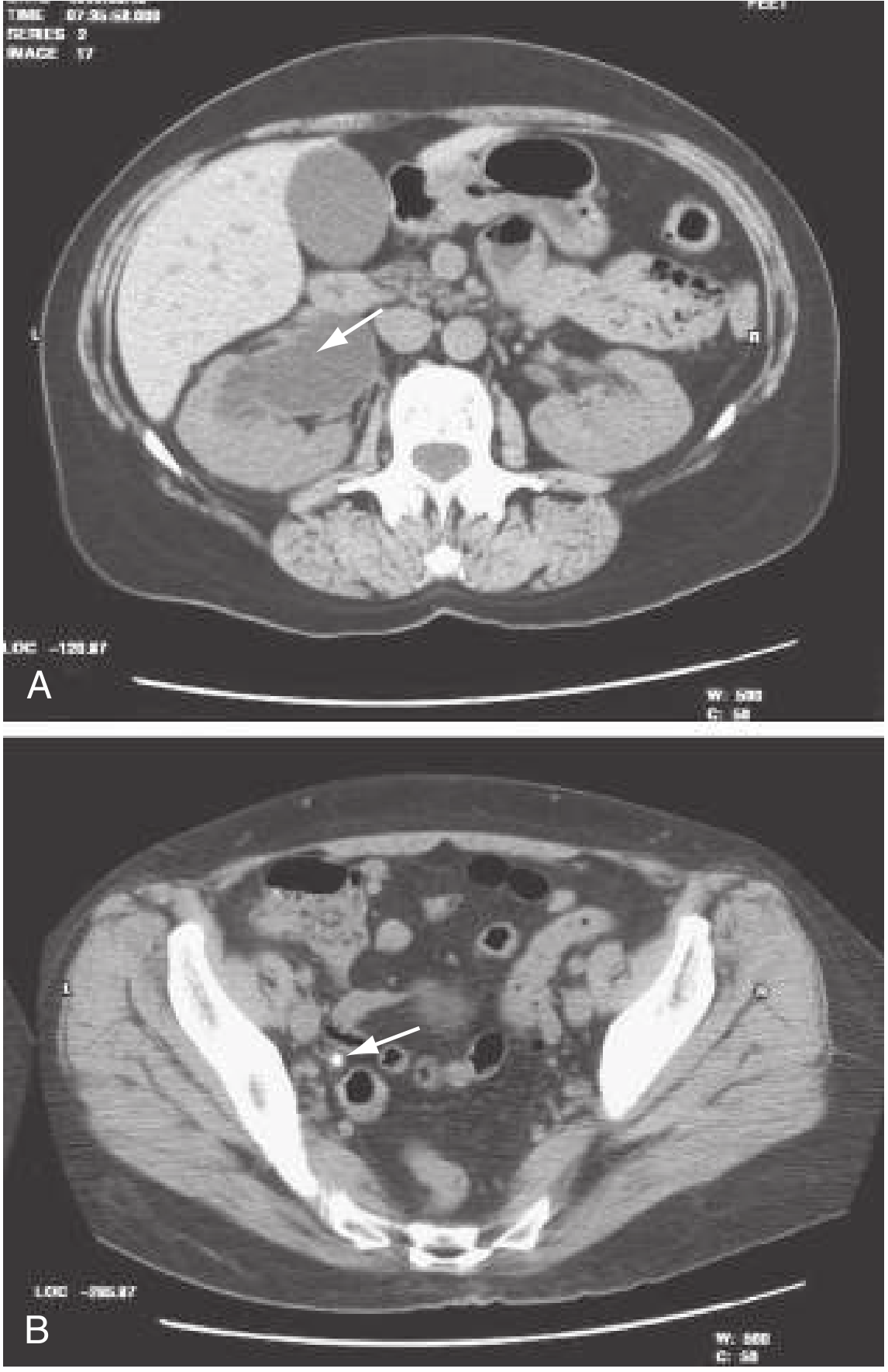
PART 2 - IMAGING
| Modality | Details | When to Use |
|---|---|---|
| Non-contrast CT KUB (NCCT) | Gold standard - sensitivity 94-100%, specificity 92-99%. Detects all stone types including radiolucent uric acid stones. Can detect stones as small as 1 mm. Determines stone density (Hounsfield units - guides ESWL suitability) | First-line in adults with acute renal colic |
| Ultrasound (USS) | Safe, no radiation. Detects hydronephrosis and stones > 3 mm. Cannot reliably see ureteral stones directly | First-line in pregnancy and children; bedside triage |
| Plain X-ray KUB | Detects radiopaque stones (calcium, struvite, cystine). Misses radiolucent uric acid stones. Sensitivity 59%, specificity 71% | Follow-up of known radiopaque stones; NOT for diagnosis |
| IVP (Intravenous pyelogram) | Historic gold standard. Provides anatomic detail of collecting system | Now largely replaced by NCCT; used pre-operatively for mapping |
| MRI Urography | No radiation; limited stone detection but shows obstruction well | Pregnancy when USS inadequate |
PART 3 - TREATMENT OPTIONS
Step 1: Acute Pain Management (IMMEDIATE PRIORITY)
The first priority is adequate analgesia.
1. NSAIDs - FIRST LINE
| Drug | Dose | Route |
|---|---|---|
| Ketorolac | 30 mg IV | IV (rapid onset) |
| Diclofenac | 75 mg IM | IM injection |
| Ibuprofen | 400-600 mg | Oral (mild cases) |
Mechanism: Reduce ureteral spasm AND lower GFR in the obstructed kidney → decrease renal capsular pressure → dual analgesic effect.
Cautions: Avoid in renal impairment (eGFR < 30), peptic ulcer disease, dehydration, elderly with cardiovascular risk.
2. Opioids - SECOND LINE / ADJUNCT
| Drug | Dose | Route |
|---|---|---|
| Morphine | 0.1 mg/kg IV | IV titrated |
| Fentanyl | 1-2 μg/kg IV | IV (fastest onset) |
| Codeine/Tramadol | Standard doses | Oral (mild-moderate) |
Note: The combination of NSAID + opioid is more effective than either alone and reduces ED length of stay.
3. Antiemetics (for nausea/vomiting)
| Drug | Dose | Route |
|---|---|---|
| Ondansetron | 4 mg IV | IV |
| Metoclopramide | 10 mg IV | IV |
| Cyclizine | 50 mg IM | IM |
4. IV Hydration
- Give IV fluids if patient cannot tolerate oral intake.
- Note: There is NO evidence that aggressive high-volume IV fluid therapy speeds stone passage or improves outcomes - give enough to maintain hydration only.
Step 2: Medical Expulsive Therapy (MET) - To Help Stone Pass
Alpha-1 Blockers - RECOMMENDED for distal ureteral stones < 10 mm
| Drug | Dose | Evidence |
|---|---|---|
| Tamsulosin | 0.4 mg orally once daily | Most studied; Cochrane review (67 studies, 10,509 patients) confirms efficacy |
| Alfuzosin | 10 mg orally once daily | Alternative alpha-blocker |
Mechanism: Relax ureteral smooth muscle → reduce tone and frequency of peristaltic contractions → facilitate stone passage down the ureter.
AUA guideline: MET recommended for stones < 10 mm.
EAU guideline: MET recommended for stones > 5 mm.
Effect: Alpha-blockers are less effective for stones ≤ 5 mm (because these already have a high spontaneous passage rate) but significantly improve passage for stones 5-10 mm.
Tamsulosin has been shown superior to nifedipine (calcium channel blocker) for MET.
Step 3: Watchful Waiting / Observation (Conservative Management)
Spontaneous Passage Rates by Stone Size
| Stone Size | Spontaneous Passage Rate |
|---|---|
| < 4 mm | ~55% - high; most pass spontaneously |
| 4-6 mm | ~35% |
| > 6 mm | ~8% - unlikely to pass |
Spontaneous Passage Rates by Location
| Location | Spontaneous Passage Rate |
|---|---|
| Proximal ureter | 12% |
| Mid ureter | 22% |
| Distal ureter | 45% (most likely to pass) |
AUA recommendation: Allow 4-6 weeks of conservative observation for stones < 10 mm with:
- Adequate pain control
- No infection
- No significant obstruction
- Normal or preserved renal function on the affected side
Step 4: Surgical / Interventional Treatment (When Conservative Fails)
Indications for Intervention
- Stone > 10 mm (unlikely to pass spontaneously)
- Failure to pass after 4-6 weeks observation
- Intractable pain not controlled by analgesia
- Persistent vomiting / unable to maintain hydration
- Impaired or solitary kidney with obstruction
- Infection + obstruction = UROLOGIC EMERGENCY (see below)
- Bilateral ureteral obstruction
Interventional Options
1. Ureteroscopy (URS) + Laser Lithotripsy
- Flexible ureteroscope passed up the urethra → bladder → ureter
- Holmium-YAG laser fragments the stone
- Basket extraction of fragments
- Used for stones in ureter or kidney < 2 cm
- Stone-free rate HIGHER than ESWL and lower retreatment rate
- A JJ stent may be left post-procedure to keep the ureter open
2. Extracorporeal Shock Wave Lithotripsy (ESWL)
- Focused high-energy shock waves directed at the stone from outside the body
- Fragments the stone into smaller pieces that pass spontaneously
- Used for stones < 2 cm in kidney or proximal ureter
- Non-invasive; done under sedation/anaesthesia
- Stone density on CT (Hounsfield units) predicts ESWL success - harder stones (e.g. calcium oxalate monohydrate, cystine) respond poorly
- Lower stone-free rate than ureteroscopy but less invasive
3. Percutaneous Nephrolithotomy (PCNL)
- A tract is dilated from skin directly into the renal collecting system
- Stone removed directly through the tract
- Used for stones > 2 cm, staghorn calculi, ESWL-refractory stones, multiple stones, hard stones
- Most invasive of the three but most effective for large stones
- Risk: bleeding, infection, urine leak
Comparison of Interventional Methods
| Method | Stone Size | Location | Stone-free Rate | Invasiveness |
|---|---|---|---|---|
| ESWL | < 2 cm | Kidney / proximal ureter | Moderate | Non-invasive |
| Ureteroscopy + laser | < 2 cm | Any part of ureter or kidney | High (better than ESWL) | Minimally invasive |
| PCNL | > 2 cm / staghorn | Kidney | Highest | Invasive (percutaneous) |
| Open surgery | Any | Any | Highest | Major surgery (last resort) |
Step 5: EMERGENCY - Infected Obstructed Stone (Sepsis + Obstruction)
This is the most dangerous scenario in urolithiasis - a true urologic emergency.
Recognition
- Fever + loin pain + signs of sepsis (tachycardia, hypotension, rigors)
- CT showing stone + hydronephrosis
- Positive urine culture or leukocytosis
Management (IMMEDIATE)
- IV broad-spectrum antibiotics: Ceftriaxone 1 g IV (or piperacillin-tazobactam if septic)
- IV fluid resuscitation
- Urgent urologic consultation
- Emergency drainage - either:
- Ureteral stent (JJ stent placed cystoscopically) OR
- Percutaneous nephrostomy (nephrostomy tube placed radiologically under USS/fluoroscopy)
- Definitive stone treatment (ureteroscopy or PCNL) is deferred until infection is treated and patient is stabilized
⚠️ Do NOT attempt to remove the stone in an infected system - drain first, treat later.
Step 6: Stone-Specific Prevention (Long-Term Treatment)
| Stone Type | Prevention Strategy |
|---|---|
| Calcium oxalate | High fluid intake (> 2.5 L/day); low sodium diet (< 2.3 g/day); low animal protein; normal dietary calcium (do NOT restrict); thiazide diuretics if hypercalciuria; potassium citrate if hypocitraturia; avoid spinach/rhubarb if hyperoxaluria |
| Uric acid | Urinary alkalinization with potassium citrate (target urine pH 6-6.5); low protein diet; allopurinol or febuxostat if hyperuricosuria |
| Struvite | Surgical removal (PCNL); treat underlying infection; monthly urine cultures; acetohydroxamic acid (urease inhibitor) |
| Cystine | High fluid intake (3.5-5 L/day including overnight); sodium restriction; urinary alkalinization to pH 7.0-7.5; tiopronin (breaks disulfide bonds) |
Summary Algorithm
RENAL COLIC
│
├── IMMEDIATE: Analgesia (IV NSAID ± opioid) + Antiemetic + IV fluids
│
├── IMAGING: Non-contrast CT KUB (gold standard)
│ Ultrasound in pregnancy/children
│
├── LABS: Dipstick → MSU/culture → Creatinine → FBC → Ca/Urate → βhCG
│
├── Stone < 10mm + No infection + Pain controlled
│ └── CONSERVATIVE: MET (Tamsulosin 0.4mg/day) + analgesia x 4-6 weeks
│ ├── Passed → Strain urine, send stone for analysis
│ └── Not passed → Ureteroscopy or ESWL
│
├── Stone > 10mm or failed conservative → ESWL / Ureteroscopy / PCNL
│
└── FEVER + OBSTRUCTION = EMERGENCY
└── IV antibiotics + Urgent ureteral stent OR nephrostomy
Sources: Brenner and Rector's The Kidney; Rosen's Emergency Medicine; Washington Manual of Medical Therapeutics; Bailey and Love's Short Practice of Surgery; Campbell Walsh Wein Urology
Pregnant women pain in the back with fever and dysuria what is happening and next step management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have everything needed. Here is the complete, textbook-based answer.
Pregnant Woman with Back Pain + Fever + Dysuria
What Is Happening?
This is Acute Pyelonephritis in Pregnancy - an upper urinary tract infection involving the renal parenchyma, pelvis, and calyces.
This is not a simple UTI (cystitis). The triad of:
- Fever (>38.5°C)
- Back/flank pain (costovertebral angle tenderness)
- Dysuria (lower urinary tract symptoms preceding the upper tract infection)
...in a pregnant woman = pyelonephritis until proven otherwise.
This is one of the most serious medical complications of pregnancy and a common cause of septic shock in pregnant women.
Why Is Pregnancy a Special Risk?
Pregnancy creates unique anatomical and physiological changes that make women highly vulnerable to ascending UTI:
| Factor | Effect |
|---|---|
| Progesterone | Relaxes ureteral smooth muscle → impairs ureteral peristalsis → urine stasis |
| Uterine compression | Physically compresses ureters (especially RIGHT ureter due to dextrorotation of uterus) → hydronephrosis → urinary stasis |
| Alkaline urine | Increased bicarbonate excretion raises urinary pH → favors bacterial growth |
| Glycosuria | Common in pregnancy → glucose in urine feeds bacteria |
| Increased estrogen | Accelerates growth of uropathogenic E. coli strains |
| Bladder pressure | Incomplete emptying → residual urine → bacterial colonization |
Why predominantly right-sided? The sigmoid colon pushes the uterus to the right (dextrorotation), causing greater mechanical compression of the right ureter. In ≥75% of cases, pyelonephritis in pregnancy is right-sided.
Causative Organisms
| Organism | Frequency |
|---|---|
| Escherichia coli | 70-80% (dominant) |
| Klebsiella pneumoniae | ~7% |
| Staphylococcus aureus | ~7% |
| Proteus mirabilis | ~2% |
| Group B Streptococcus (GBS) | ~10% |
| Enterobacter species | Small % |
E. coli attaches to uroepithelium via P fimbriae (papG adhesins) and type 1 pili - the virulence factors that drive ascent from bladder to kidney.
Why This Starts as Dysuria (Lower Tract Infection)
The infection almost always begins as asymptomatic bacteriuria or cystitis in the bladder. Without treatment, bacteria ascend the ureter (aided by the hormonal and mechanical changes above) to reach the renal pelvis and parenchyma, causing pyelonephritis. This is why:
- Up to 30% of pregnant women with untreated asymptomatic bacteriuria develop pyelonephritis
- Treating bacteriuria early is a USPSTF Grade A recommendation
Dangerous Complications in Pregnancy (Why This Must Be Treated Aggressively)
Up to 20% of pregnant women with pyelonephritis develop multi-organ involvement from endotoxemia and sepsis:
| Complication | Details |
|---|---|
| Septic shock | Pyelonephritis is one of the most common causes of septic shock in pregnancy |
| ARDS (Acute Respiratory Distress Syndrome) | Occurs in 2-8%; cytokine-mediated capillary injury → pulmonary edema → hypoxia |
| Hemolytic anaemia | Endotoxin-mediated RBC destruction |
| Acute renal dysfunction | Occurs in ~7-20%; usually transient but serious |
| Disseminated Intravascular Coagulation (DIC) | Rare but life-threatening |
| Preterm labour | Cytokines stimulate uterine contractions - pyelonephritis is one of the most important identifiable causes of preterm labour |
| Fetal risk | Hyperthermia is teratogenic (especially 1st trimester); preterm birth; low birth weight |
⚠️ ARDS predictors: Heart rate >110/min, temperature ≥103°F in first 24 hours, use of ampicillin alone, tocolytic use, fluid overload. Watch for tachypnea and oxygen desaturation.
Next Step Management
Step 1: Immediate Assessment
Clinical Examination
- Vital signs: Temperature, HR, BP, RR, SpO₂ (pulse oximetry mandatory)
- Costovertebral angle (CVA) tenderness: Punch/percussion tenderness over the flank = hallmark of pyelonephritis
- Abdominal examination: Uterine fundal height, uterine irritability/contractions
- Assess hydration status: Dry mucous membranes, skin turgor, urine output
Step 2: Investigations
Urine Tests (MANDATORY)
| Test | Purpose |
|---|---|
| Urine dipstick | Leucocytes, nitrites, blood - rapid screening |
| Urinalysis + microscopy (MSU) | Pyuria (>5 WBC/hpf); WBC casts are HIGHLY predictive of pyelonephritis; bacteria; RBCs |
| Urine culture + sensitivity | Identifies organism and antibiotic sensitivities; guides therapy; COLLECT BEFORE antibiotics |
Blood Tests
| Test | Purpose |
|---|---|
| FBC (Full Blood Count) | Leukocytosis confirms infection; anaemia from haemolysis |
| Serum Creatinine + eGFR | Renal function baseline; impairment in 7-20% |
| Electrolytes (Na, K, HCO₃) | Dehydration, acid-base disturbance from vomiting |
| CRP / ESR | Severity of inflammatory response |
| Blood cultures | If: high fever, signs of severe sepsis, no response to initial therapy, immunosuppressed |
| Serum urea | Renal function |
| LFTs | Differential (cholecystitis, hepatitis can mimic) |
| Coagulation screen | If sepsis / DIC suspected |
| Blood glucose | Diabetic ketoacidosis can mimic; diabetes is a risk factor |
Imaging
| Test | Purpose |
|---|---|
| Renal ultrasound (USS) | First-line imaging in pregnancy (no radiation). Detects hydronephrosis, perinephric abscess, stones. Physiologic ureteral dilation is normal in pregnancy - do not over-interpret |
| Chest X-ray | If dyspnoea, tachypnoea, SpO₂ dropping → rule out ARDS / pulmonary oedema |
| Arterial Blood Gas (ABG) | If respiratory symptoms → assess hypoxaemia, acidosis |
CT scan: Avoid in pregnancy unless absolutely necessary (radiation risk). Ultrasound is preferred.
Obstetric Monitoring (≥24 weeks gestation)
- CTG (Cardiotocography): Monitor fetal heart rate and uterine activity
- Uterine contractions in pyelonephritis are common and can progress to preterm labour
Step 3: Hospitalisation Decision
| Admit to Hospital | Outpatient Possible |
|---|---|
| Second half of pregnancy (≥20 weeks) - almost always admit | First half of pregnancy, only if mildly ill |
| High fever | Low-grade fever |
| Nausea and vomiting | No vomiting, tolerating oral fluids |
| Signs of sepsis | Normal/near-normal WBC |
| Dehydration | No comorbidities |
| No response to initial observation | Expected to be compliant with oral antibiotics |
| Immunocompromised, diabetic | No uterine irritability |
General rule: Most pregnant women with acute pyelonephritis should be hospitalised for at least 12-24 hours of observation even if initially mild. This is because of the risk of rapid deterioration, preterm labour, and ARDS.
Step 4: Treatment
A. IV Fluid Resuscitation (CRITICAL)
- Start isotonic crystalloid (Normal saline or Hartmann's solution) IV
- Target urine output: 30-50 mL/hour or more
- Aggressive hydration reduces renal dysfunction rate from 20% → 7%
- ⚠️ Balance fluid carefully: Over-hydration risks pulmonary oedema especially with associated capillary injury → monitor SpO₂ throughout
B. Antibiotic Therapy
Parenteral (IV) Regimens - For Moderate to Severe Disease
| Drug | Dose | Notes |
|---|---|---|
| Ceftriaxone ✅ FIRST LINE | 1-2 g IV every 24 hours | Broad spectrum; covers all major uropathogens except Enterococcus; preferred because E. coli resistance to ampicillin is high |
| Cefotaxime | 1-2 g IV every 8 hours | Alternative cephalosporin |
| Cefepime | 2 g IV every 8 hours | Extended spectrum; if resistant organisms suspected |
| Piperacillin-tazobactam | 3.75 g IV every 6-8 hours | For severe sepsis or resistant organisms |
| Ampicillin + Gentamicin | Ampicillin 2 g IV q6h + Gentamicin 5 mg/kg IV q24h | Combination for critically ill; use aminoglycosides with caution (nephrotoxicity + fetal ototoxicity) |
| Aztreonam | 1-2 g IV every 8-12 hours | Use INSTEAD of gentamicin if renal dysfunction present |
| Ampicillin-sulbactam | 1.5 g IV every 6 hours | If enterococcal infection suspected |
❌ Avoid: Fluoroquinolones (ciprofloxacin, levofloxacin) - contraindicated in pregnancy (cartilage toxicity) ❌ Avoid: TMP-SMX in first trimester (folate antagonism → neural tube defects) and third trimester (kernicterus risk) ❌ Avoid: Aminoglycosides as first choice (nephrotoxicity, fetal VIII nerve damage) ❌ Avoid: Ampicillin alone - high E. coli resistance rates
Oral (Outpatient) Regimens - Step-Down or Mild Cases
| Drug | Dose | Duration |
|---|---|---|
| Amoxicillin-clavulanate ✅ | 875/125 mg twice daily | 10-14 days |
| Cephalexin | 500 mg four times daily | 10-14 days |
| TMP-SMX DS | 1 tablet twice daily | 10-14 days (avoid 1st and 3rd trimester) |
| Amoxicillin | 500 mg three times daily | 10-14 days (check local resistance) |
Step-down criteria: Patient afebrile and asymptomatic for 24-48 hours on IV antibiotics → switch to oral to complete 10-14 day total course.
C. Antipyretic Therapy
- Paracetamol (acetaminophen) 1 g orally/IV every 6-8 hours
- Use cooling blanket if very high fever
- Important: Reduce fever promptly because:
- Hyperthermia is teratogenic (especially in first trimester)
- Increases fetal metabolic demands
- Drives uterine contractions
❌ Avoid NSAIDs (ibuprofen, diclofenac) in pregnancy - cause premature closure of ductus arteriosus (especially third trimester)
D. Monitoring During Admission
| Parameter | Frequency |
|---|---|
| Vital signs (Temp, HR, BP, RR) | Every 4 hours |
| Pulse oximetry (SpO₂) | Continuous or every 4 hours |
| Urine output | Hourly (catheterise if necessary) |
| Fetal heart rate + uterine contractions (CTG) | Every 4-8 hours at ≥24 weeks |
| Repeat FBC + creatinine | After 48 hours if not improving |
| Repeat urine culture | 1 week after treatment to confirm clearance |
E. If No Improvement After 48-72 Hours
- Suspect: urinary obstruction, resistant organism, perinephric/renal abscess
- Repeat renal ultrasound or consider MRI (non-radiation alternative to CT in pregnancy)
- Review culture sensitivities and adjust antibiotics accordingly
- Urology and nephrology consultation
F. Preterm Labour Management
If uterine contractions develop:
- Rehydrate first (contractions may resolve with hydration)
- If contractions persist → tocolysis:
- Nifedipine (calcium channel blocker) - first choice tocolytic
- Indomethacin (NSAID) - usable before 32 weeks
- ⚠️ Use tocolytics cautiously in sepsis due to synergistic cardiovascular effects (vasodilation + sepsis = risk of severe hypotension)
- ⚠️ Magnesium sulphate: Caution in severe sepsis (cardiovascular interactions)
Step 5: After Recovery - Prevention of Recurrence
- Test of cure: Repeat urine culture 1 week after completing antibiotics and again monthly throughout pregnancy
- Suppressive antibiotic therapy for the rest of pregnancy if recurrent UTI:
- Nitrofurantoin 50-100 mg at night (avoid near term - third trimester)
- Cephalexin 125-250 mg at night
- Encourage high fluid intake (>2 L/day)
- Regular antenatal attendance and urine screening at every visit
Summary Flowchart
Pregnant woman + Fever + Back/flank pain + Dysuria
│
▼
DIAGNOSIS: Acute Pyelonephritis in Pregnancy
│
▼
IMMEDIATE STEPS
├── Vital signs (HR, BP, Temp, RR, SpO₂)
├── Urine dipstick → MSU for C&S (before antibiotics)
├── FBC, creatinine, electrolytes, CRP
├── Blood cultures (if septic)
├── Renal USS (not CT)
└── CTG if ≥24 weeks
│
▼
IV Fluid Resuscitation (target UO >30 mL/hr)
+
IV Ceftriaxone 1-2 g daily (first-line)
+
Paracetamol (fever reduction)
+
Antiemetics
│
▼
Hospital admission (12-24 hours minimum)
Continuous SpO₂ monitoring (ARDS risk)
Fetal monitoring (preterm labour risk)
│
▼
Afebrile + stable for 24-48h?
├── YES → Step down to oral antibiotics → discharge
│ Complete 10-14 day course
│ Repeat urine culture in 1 week
└── NO → Renal USS for abscess/obstruction
Review antibiotic sensitivities
Urology consultation
Sources: Creasy & Resnik's Maternal-Fetal Medicine (Principles and Practice); Rosen's Emergency Medicine; Brenner & Rector's The Kidney
70 yr old drunk man with urine retention what is the next step ,what we see in diagnostic test and what are the tactic
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Excellent - I have comprehensive textbook data. Here is the full clinical answer.
70-Year-Old Intoxicated Man with Urinary Retention
What Is Happening? (Clinical Diagnosis)
This is Acute Urinary Retention (AUR) - a sudden, complete inability to pass urine despite a painfully full bladder.
In a 70-year-old man, the most likely underlying cause is Benign Prostatic Hyperplasia (BPH) with the acute episode precipitated by alcohol intoxication.
This is classified as Precipitated AUR (triggered by a specific event - alcohol) on a background of likely pre-existing BPH/bladder outlet obstruction.
Why Alcohol Caused/Precipitated This
Alcohol contributes to AUR through several mechanisms:
| Mechanism | Explanation |
|---|---|
| Diuretic effect | Alcohol inhibits ADH (antidiuretic hormone) → rapid diuresis → rapid bladder filling → overdistension |
| Bladder overdistension | Severely overfilled bladder → detrusor muscle overstretched → loses contractile force → cannot generate enough pressure to overcome prostatic obstruction |
| CNS depression | Blunts the urge to void → patient ignores filling signals until retention is complete |
| Alpha-adrenergic stimulation | Alcohol can increase sympathetic tone → increased urethral and prostatic smooth muscle tone → raised outflow resistance |
| Dehydration | Paradoxically, post-alcohol dehydration reduces effective voiding |
| Sedation | Reduced mobility and awareness of bladder fullness |
BPH is present in 80% of men in their 70s. AUR occurs in 10% of men in their 70s and up to 33% of men in their 80s. Alcohol, bed rest, medications (anticholinergics, opioids, antihistamines), constipation, and surgery are classic precipitating triggers.
Two Types of AUR - Important Clinical Distinction
| Type | Definition | Prognosis |
|---|---|---|
| Spontaneous AUR | No identifiable trigger; natural progression of BPH | 75% will eventually need surgery; 15% have recurrent AUR |
| Precipitated AUR | Triggered by alcohol, drugs, anaesthesia, UTI, overdistension | Better prognosis; only 9% have spontaneous AUR later; only 26% need surgery |
This patient has precipitated AUR from alcohol - this is actually a better prognostic sign. Once catheterised and alcohol cleared, he has a reasonable chance of successful voiding.
Key Clinical Features
- Suprapubic pain (often severe - "cannot pass urine despite desperate urge")
- Distended bladder palpable above the pubic symphysis (dull to percussion)
- Restlessness and distress
- No urine output for hours despite feeling urgently full
- Overflow incontinence may occur in chronic/painless retention (dribbling small amounts despite full bladder)
- Note: Intoxicated patients may be less aware of pain - the bladder may be enormous before presentation
⚠️ A distended palpable bladder above the umbilicus = large volume retention (often >500 mL, sometimes >1-2 litres). If untreated → acute renal failure from back-pressure.
PART 1: Diagnostic Tests
A. Bedside / Immediate Assessment
| Test | Purpose | What to Expect |
|---|---|---|
| Bladder ultrasound / Bladder scanner | Confirms urinary retention; measures retained volume | Retention confirmed if > 300 mL (often > 600-800 mL in acute retention) |
| Renal USS | Assess for hydronephrosis (upper tract obstruction if chronic) | May show bilateral hydronephrosis if long-standing |
| Post-void residual (PVR) | After draining by catheter - measured with bladder scan | Normal < 50 mL; >200 mL = significant retention |
B. Urine Tests
| Test | Purpose | What to Expect |
|---|---|---|
| Urine dipstick | Blood (haematuria), leucocytes, nitrites | May have haematuria from congested prostatic veins; leucocytes if UTI coexists |
| MSU (Midstream urine culture) | Exclude/detect UTI - common in retained urine | Possible growth of E. coli or gram-negatives if retention has been prolonged |
| Urine cytology | If haematuria present - bladder cancer screen | Can be done later as outpatient |
C. Blood Tests
| Test | Purpose | What to Expect |
|---|---|---|
| Serum creatinine + eGFR | Assess renal function - back-pressure from chronic retention may cause AKI | May be elevated if chronic retention present |
| Serum electrolytes (Na, K, HCO₃) | Electrolyte balance; post-obstructive diuresis can cause electrolyte shifts | Monitor closely after catheter placed |
| FBC | WBC for infection; Hb for anaemia (haematuria) | Leukocytosis if UTI/infection |
| PSA (Prostate-Specific Antigen) | Screen for prostate cancer underlying the obstruction | Note: PSA is FALSELY elevated in AUR and instrumentation - wait 4-6 weeks after catheterisation before interpreting PSA reliably |
| Serum glucose | Diabetic neuropathy can cause retention | Check in elderly |
| Blood alcohol level | Confirms intoxication; guides timing of TWOC | Document for clinical decision-making |
| Coagulation (INR/PT) | If haematuria present or surgery planned | Alcoholic patients may have coagulopathy from liver disease |
| LFTs | Alcohol-related liver disease assessment | Chronic alcohol use → cirrhosis |
| Blood culture | If fever present alongside retention | Retention + fever = possible infected obstruction |
⚠️ Important: In chronic painless retention (often seen with neurogenic bladder or slowly progressive BPH), renal failure can be present at presentation without the patient being aware. Always check creatinine.
D. Imaging
| Modality | Purpose | Finding |
|---|---|---|
| Bladder ultrasound | Volume measurement; confirm retention | Distended bladder, large PVR |
| Renal USS | Hydronephrosis, renal size, perinephric abnormality | Bilateral hydronephrosis if chronic obstruction |
| TRUS (Transrectal Ultrasound) | Measure prostate volume accurately | Enlarged prostate (>30 mL increases AUR risk) |
| X-ray KUB | Bladder stones, calcification | Phleboliths vs stones |
| CT scan | If carcinoma, obstruction from other causes suspected | Not routine first-line |
E. After Stabilisation - Further BPH Work-Up
| Test | Purpose |
|---|---|
| IPSS (International Prostate Symptom Score) | Quantify severity of LUTS; guides treatment decision |
| Uroflowmetry | Measure peak urine flow rate; < 10 mL/sec = significant obstruction |
| Pressure-flow urodynamic study | Gold standard for confirming BOO if surgery planned |
| Flexible cystoscopy | If haematuria, suspected urethral stricture, or before TURP |
| DRE (Digital Rectal Examination) | Assess prostate size, consistency - smooth/rubbery = BPH; hard/nodular = cancer |
| PSA (4-6 weeks post-catheter) | Rule out prostate cancer as cause of obstruction |
PART 2: Immediate Next Steps (Management Tactics)
STEP 1: IMMEDIATE - Catheterisation (RELIEVE RETENTION NOW)
This is the first and most urgent step - do NOT delay while waiting for test results.
Urethral Catheterisation
| Detail | What to Do |
|---|---|
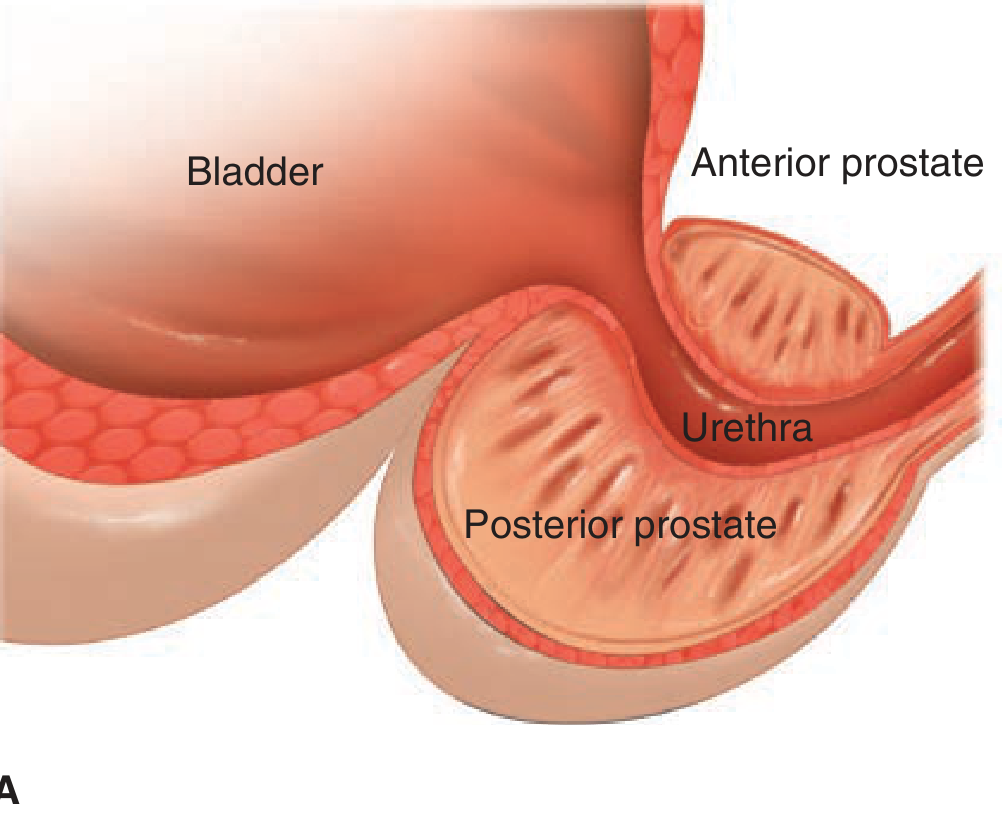
| Catheter type | Coude (curved-tip) catheter - PREFERRED in men with BPH. The curved tip negotiates the angulation of the prostatic urethra |
| Size | Use 18-20 Fr (larger = stiffer = pushes through prostatic urethra rather than curling; do NOT use small catheter for BPH) |
| Technique | Coude tip always at 12 o'clock position during insertion |
| Anaesthetic gel | Instil lidocaine 2% gel, wait 3-5 minutes before inserting catheter |
| Confirm placement | Free flow of urine before inflating balloon |
| Balloon | Inflate with 10 mL sterile water only after urine flows freely |
| Measure and record | Volume of urine drained - this has prognostic and monitoring significance |
If Urethral Catheterisation Fails
| Scenario | Action |
|---|---|
| Resistance at prostate (BPH) | Use larger Coude catheter; try 20-22 Fr |
| Resistance near meatus (stricture) | Use smaller 12-14 Fr catheter for urethral stricture |
| Still fails | Urological consultation for: cystoscope + guidewire + dilators (Seldinger technique) OR suprapubic catheter |
| Suprapubic catheter (SPC) | Inserted 2 fingerbreadths above pubic symphysis under USS guidance; used if urethral route impossible |
STEP 2: MONITOR DRAINAGE - Beware Post-Obstructive Diuresis
After the catheter drains the bladder, a large residual volume (>1 litre) in an elderly man who has likely had chronic partial retention triggers post-obstructive diuresis:
Post-Obstructive Diuresis (POD)
- Mechanism: After relieving back-pressure, kidneys suddenly excrete the accumulated solutes (urea, sodium, water) - urine output can be 200-500 mL/hour
- Risk: Rapid fluid/electrolyte loss → hyponatraemia, hypokalaemia, hypomagnesaemia, dehydration, hypotension
- Management:
- Hourly urine output monitoring
- IV fluid replacement if urine output > 200 mL/hour (replace ~50-75% of output with normal saline or Hartmann's)
- Serial electrolytes every 4-6 hours until diuresis settles
- Do NOT clamp the catheter periodically - no evidence this prevents POD or haematuria
⚠️ If >3 litres drained at catheterisation: admit and monitor for POD.
STEP 3: ADDRESS THE ALCOHOL + ACUTE ISSUES
| Task | Action |
|---|---|
| Alcohol intoxication | Keep patient safe, fall prevention, aspiration risk if vomiting |
| IV access + fluids | If dehydrated from alcohol + urinary retention |
| Blood glucose | Hypoglycaemia risk in alcoholics |
| Thiamine (B1) | Wernicke's encephalopathy prevention in chronic alcoholic - IV Pabrinex before IV glucose |
| Treat infection | If UTI confirmed: appropriate antibiotics (e.g. co-amoxiclav or nitrofurantoin) |
| Antiemetics | If nausea/vomiting from alcohol + pain |
STEP 4: START ALPHA-BLOCKER THERAPY (Before TWOC)
Once catheter is in place, start:
| Drug | Dose | Mechanism |
|---|---|---|
| Tamsulosin (first choice) | 0.4 mg orally once daily | Alpha-1 receptor blocker → relaxes smooth muscle in prostate, urethra, and bladder neck → reduces outflow resistance |
| Alfuzosin | 10 mg orally once daily | Alternative |
| Silodosin | 8 mg orally once daily | Highly selective alpha-1A blocker |
Evidence: Alpha-blockers significantly increase the success rate of TWOC (Trial Without Catheter). Tamsulosin started before TWOC improves voiding success rate from ~40% to ~55-65%.
❌ Do NOT start 5-alpha reductase inhibitors (finasteride, dutasteride) acutely - they take 3-6 months to reduce prostate size and have no benefit in the short term.
STEP 5: TWOC - Trial Without Catheter (3-5 Days Later)
What Is TWOC?
- Remove the catheter after 3-5 days (median 5 days in clinical practice)
- Patient attempts to void spontaneously
- Check post-void residual with bladder scanner after voiding attempt
TWOC Success Rates
| Outcome | Rate |
|---|---|
| Successful voiding on first TWOC | ~61% |
| Fail first TWOC → second attempt success | ~29.5% |
| Fail second → third attempt success | ~26.4% |
| Up to 3 TWOCs can be attempted before recommending surgery |
Factors Predicting TWOC Failure
- Age > 70 (this patient's age!)
- Large volume drained at catheterisation (≥ 1 litre)
- Severe LUTS (high IPSS score)
- Spontaneous AUR (vs precipitated - alcohol is precipitated, which is better)
- Large prostate volume
TWOC Options After Catheter Removal
- Bladder scanner check: If post-void residual > 200 mL → another episode of AUR likely → repeat TWOC or consider surgery
- Clean Intermittent Self-Catheterisation (CISC): Patient catheterises himself every 4-6 hours; reduces infection risk vs indwelling catheter; preferred by urologists but patients are often reluctant
STEP 6: DEFINITIVE MANAGEMENT OF UNDERLYING BPH
If TWOC fails (3 attempts) or patient has high-risk features:
Medical (Long-Term BPH Management)
| Drug Class | Drug | Effect |
|---|---|---|
| Alpha-blockers | Tamsulosin, alfuzosin, doxazosin | Relax prostate/urethral smooth muscle; fast acting (days) |
| 5-Alpha reductase inhibitors | Finasteride, dutasteride | Shrink prostate; reduce AUR risk by 50% long-term; take 3-6 months |
| Combination | Tamsulosin + dutasteride (CombAT trial) | Superior to monotherapy in men with large prostates; reduces AUR and surgery risk |
| PDE-5 inhibitors | Tadalafil 5 mg daily | If LUTS + erectile dysfunction coexist |
| Antimuscarinics + alpha-blocker | For mixed storage + voiding symptoms | Caution - can worsen retention if used alone |
Surgical (When Medical Fails / TWOC Fails)
| Procedure | Indication | Notes |
|---|---|---|
| TURP (Transurethral Resection of Prostate) | Gold standard for BPH surgery | Removes obstructing prostatic tissue endoscopically; curative |
| Laser prostatectomy (HoLEP, PVP) | Alternative to TURP; less bleeding | Good for anticoagulated patients |
| Bipolar TURP | Reduces risk of TUR syndrome vs monopolar | Modern alternative |
| Open prostatectomy | Very large prostate (>80-100 mL) | Rarely needed |
| Urethral stent | Unfit for surgery (high anaesthetic risk) | Temporary measure |
STEP 7: COUNSEL + ADDRESS ALCOHOL
This is important and often overlooked:
- Alcohol is a clear precipitating factor - counsel about reducing/stopping alcohol
- Address alcohol dependence if chronic (AUDIT score, CAGE questionnaire)
- Alcohol causes: diuresis (bladder overdistension) + sympathetic tone increase + CNS sedation - triple mechanism for AUR
Summary Algorithm
70yr old drunk man + unable to void + distended bladder
│
▼
DIAGNOSIS: Acute Urinary Retention (AUR)
Most likely cause: BPH + precipitated by alcohol
│
▼
STEP 1: IMMEDIATE → Urethral catheterisation
• Coude catheter (18-20 Fr) for BPH
• Lidocaine gel first
• Record volume drained
• Fails? → Suprapubic catheter / urology consult
│
▼
STEP 2: MONITOR → Post-obstructive diuresis
• Hourly urine output
• IV fluids if UO >200 mL/hr
• Electrolytes q4-6h
• Creatinine baseline
│
▼
STEP 3: BLOODS + URINE
• Creatinine, eGFR, electrolytes, FBC
• Urine dipstick + MSU
• PSA (note: interpret 4-6 weeks post-catheter)
• Renal USS (hydronephrosis?)
• DRE (prostate assessment)
│
▼
STEP 4: Start TAMSULOSIN 0.4mg daily
(increases TWOC success rate)
│
▼
STEP 5: TWOC at 3-5 days
61% success → discharge on tamsulosin
Fail → repeat (up to 3 attempts)
All fail → TURP or laser prostatectomy
│
▼
STEP 6: Address ALCOHOL (precipitating factor)
Counsel / refer to addiction services
Sources: Campbell Walsh Wein Urology (9780323546423); Schwartz's Principles of Surgery (9781259835346); Symptom to Diagnosis Evidence-Based Guide (9781260121117); Rosen's Emergency Medicine (9780323757898)
Fever sometimes in past few days hematuria And difficulty in urine young women in er what should be done
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
I now have all I need from the textbooks. Here is the full structured answer.
Young Woman in ER: Fever + Hematuria + Difficulty Urinating (Past Few Days)
First - What Is the Clinical Picture Telling You?
This triad in a young woman with symptoms over several days is a classic presentation that sits at the intersection of infectious, inflammatory, and (rarely) structural urological disease. The fever is the most critical differentiating factor - it lifts this above a simple lower UTI.
The three most likely diagnoses, in order of probability:
| Priority | Diagnosis | Why |
|---|---|---|
| 🥇 Most likely | Acute Pyelonephritis (upper UTI) | Fever + dysuria + hematuria lasting days; lower UTI has ascended to kidneys |
| 🥈 Very possible | Haemorrhagic Cystitis (severe lower UTI) | Dysuria + visible hematuria + fever from intense bladder inflammation |
| 🥉 Must not miss | IgA Nephropathy (Berger Disease) | Young patient + hematuria after recent infection + fever; glomerular cause |
| ⚠️ Consider | Urinary Tract Stone + UTI | Can cause all three symptoms; fever = infected obstruction = emergency |
| ⚠️ Consider | STI (Chlamydia/Gonorrhoea + urethritis) | Young woman + dysuria; mimics UTI |
| ⚠️ Exclude | Ectopic pregnancy / pelvic inflammatory disease | Fever + pelvic pain in young woman |
Step 1: Immediate Assessment in the ER
Rapid ABC + Triage
First things first - assess how sick she is:
| Parameter | Red Flag Values | Significance |
|---|---|---|
| Temperature | > 38.5°C (high fever) | Systemic infection / sepsis |
| Heart rate | > 100 bpm | Sepsis, dehydration |
| Blood pressure | < 90/60 mmHg | Septic shock |
| Respiratory rate | > 20/min | Possible ARDS (if septic) |
| SpO₂ | < 95% | Pulmonary involvement |
| GCS / mental status | Confused, drowsy | Urosepsis |
⚠️ If she is tachycardic + hypotensive + febrile = sepsis → immediate IV access, blood cultures, IV antibiotics within 1 hour (Sepsis 6 protocol)
Step 2: Focused History (Key Questions)
About the Hematuria
- Is it visible (gross) or only found on dipstick (microscopic)?
- Is it the whole stream, initial, or terminal?
- Are there clots? What shape? (Worm-shaped = upper tract; cuboid = bladder)
- Is it painless or painful?
About the Dysuria / Voiding Difficulty
- Burning on urination? (cystitis/urethritis)
- Urgency, frequency?
- Inability to void / incomplete emptying?
- Suprapubic pain or cramping?
About the Fever
- How high? Gradual or sudden onset?
- Any rigors (shaking chills)? → Strongly suggests bacteraemia/sepsis
- Loin/flank pain? (upper UTI)
- Costovertebral angle pain?
Background History
- Last menstrual period - MANDATORY (exclude pregnancy)
- Sexual history - multiple partners, new partner, unprotected sex → STI risk
- Previous UTIs - recurrent UTI history?
- Recent upper respiratory tract infection → IgA nephropathy trigger
- Medications: analgesics, cyclophosphamide (drug causes haemorrhagic cystitis)
- Family history: renal disease, deafness → Alport syndrome
- Rash, joint pain, oral ulcers → Lupus nephritis (SLE)
- Trauma - any recent injury?
- Contraception - diaphragm use increases UTI risk
Step 3: Physical Examination
| Examination | What to Look For | Significance |
|---|---|---|
| Vitals | Temperature, HR, BP, RR, SpO₂ | Assess severity / sepsis |
| Abdominal exam | Suprapubic tenderness | Cystitis |
| Flank / loin exam | Costovertebral angle (CVA) tenderness - punch test | Pathognomonic for pyelonephritis |
| Pelvic exam | Vaginal discharge, cervical excitation tenderness | STI / PID |
| Skin | Rash, purpura | SLE, IgA nephropathy (Henoch-Schönlein), vasculitis |
| Joints | Swelling, tenderness | SLE, reactive arthritis |
| Eyes | Periorbital oedema | Nephrotic syndrome |
| Throat | Pharyngitis / tonsillitis | Recent URTI → post-infectious GN or IgA nephropathy trigger |
| Bimanual pelvic exam | Uterine / adnexal tenderness | PID, ectopic pregnancy |
Step 4: Investigations
Urine Tests (MOST IMPORTANT - Order Immediately)
| Test | Purpose | What to Expect / Look For |
|---|---|---|
| Urine dipstick | Fast screen - blood, leucocytes, nitrites, protein, glucose | Blood + leucocytes + nitrites = UTI; Blood + protein = glomerular disease |
| Urine microscopy (MSU) | Characterise RBCs - KEY test | Round RBCs = urological source (UTI, stone, tumour); Dysmorphic RBCs + RBC casts = glomerular disease (IgA nephropathy, GN) |
| Urine culture + sensitivity | Identify organism; guide antibiotic choice | COLLECT BEFORE starting antibiotics |
| Urine protein (dipstick or PCR/ACR) | Quantify proteinuria | Significant proteinuria (2-3+) = glomerular disease → nephrology referral |
| Urine pH | Clue to stone type if renal colic suspected | - |
| Urine pregnancy test (βhCG) | MANDATORY in any woman of childbearing age | Excludes ectopic pregnancy; changes management if positive |
| STI swabs | Chlamydia / gonorrhoea | If sexual history positive or pelvic exam abnormal |
Microscopy Decision Tree
Urine microscopy result
│
├── Dysmorphic RBCs + RBC casts + proteinuria
│ → GLOMERULAR DISEASE (IgA nephropathy, GN, SLE, Goodpasture)
│ → Nephrology referral + further serology
│
├── Round (non-dysmorphic) RBCs + WBCs + bacteria
│ → INFECTION (cystitis / pyelonephritis)
│ → Urine culture + antibiotics
│
└── Round RBCs only (no WBCs, no bacteria)
→ STRUCTURAL/UROLOGICAL cause (stone, tumour, trauma)
→ CT KUB + urology
Blood Tests
| Test | Purpose | Clinical Relevance |
|---|---|---|
| FBC (Full Blood Count) | WBC count, Hb, platelets | Leukocytosis → infection; anaemia → chronic haematuria; thrombocytopaenia → SLE/TTP |
| CRP / ESR | Systemic inflammation marker | Elevated in infection, GN, SLE |
| Serum creatinine + eGFR | Renal function | Impaired → upper tract disease or glomerulonephritis |
| Serum electrolytes | Na, K, HCO₃ | Electrolyte disturbance with renal impairment |
| Urine protein:creatinine ratio (PCR) or 24h urine protein | Quantify proteinuria | > 0.3 = significant → glomerular work-up |
| Blood cultures x2 | If systemic sepsis / high fever / rigors | Bacteraemia in pyelonephritis; guide IV antibiotic choice |
| Serum LDH + haptoglobin | Haemolytic anaemia | If HUS/TTP suspected (Escherichia coli O157:H7) |
| Serology (if glomerular disease suspected) | ANA, anti-dsDNA (SLE); ANCA (vasculitis); anti-GBM (Goodpasture); ASO titre (post-strep); complement C3/C4; IgA level | Target based on clinical clues |
| Coagulation screen (PT/INR) | Bleeding diathesis | Could contribute to haematuria if coagulopathic |
| βhCG (blood) | Confirm/exclude pregnancy | If urine test equivocal |
Imaging
| Test | When to Use | What to Look For |
|---|---|---|
| Renal ultrasound (USS) | First-line in ER | Hydronephrosis, renal stones, renal size, echogenicity (GN = echogenic kidneys), perinephric collection/abscess |
| CT KUB (non-contrast) | If renal stone suspected (loin-to-groin pain, colicky) | Stone location and size, degree of obstruction |
| Pelvic USS | If PID or ectopic pregnancy suspected | Adnexal mass, free fluid, tubo-ovarian abscess |
| Chest X-ray | If fever + respiratory symptoms | Pulmonary involvement (Goodpasture = pulmonary haemorrhage; septic emboli) |
Step 5: Working Diagnosis Framework
Based on what you find, here is how to stratify:
Scenario A: Urine = WBCs + bacteria + round RBCs, CVA tenderness, HIGH fever (38.5°C+), rigors
DIAGNOSIS: Acute Pyelonephritis
This is the most likely diagnosis in this case.
Management:
- Admit to hospital (young woman with fever, hematuria, and days of symptoms = not mild)
- IV access + blood cultures + urine culture (before antibiotics)
- IV ceftriaxone 1 g daily - first-line (broad spectrum, covers E. coli; ampicillin resistance is high)
- IV fluid resuscitation - maintain urine output > 30 mL/hour
- IV paracetamol for fever and pain
- IV antiemetics (ondansetron 4 mg IV) if nausea
- Renal USS - exclude abscess or obstruction
- Monitor: vitals, urine output, temperature chart, creatinine
- Step down to oral antibiotics when afebrile for 24-48 hours
- Total antibiotic course: 10-14 days (co-amoxiclav, ciprofloxacin, or TMP-SMX oral - guided by culture sensitivities)
- Repeat urine culture 1 week after completing antibiotics
Scenario B: Urine = WBCs + bacteria + round RBCs, SUPRAPUBIC pain, LOW fever, no CVA tenderness
DIAGNOSIS: Haemorrhagic Cystitis (severe lower UTI with mucosal bleeding)
Management:
- Oral antibiotics if no systemic toxicity:
- Nitrofurantoin 100 mg BD x 5 days (first-line)
- Trimethoprim 200 mg BD x 7 days (if local resistance < 20%)
- Co-amoxiclav 625 mg TDS x 7 days (if above not suitable)
- High fluid intake (> 2 L/day) to flush bladder
- Analgesia: paracetamol; phenazopyridine (bladder analgesic) if available
- Repeat urine culture in 48 hours if not improving
- If no improvement after 48h → IV antibiotics + re-evaluate for upper tract involvement
Scenario C: Dysmorphic RBCs + RBC casts + significant proteinuria, recent URTI, young patient
DIAGNOSIS: Glomerulonephritis - Most likely IgA Nephropathy (Berger Disease)
IgA nephropathy is the most common glomerular disease and most common cause of glomerular haematuria (30% of cases). It classically presents:
- Young patient (15-35 years, male predominance but occurs in women)
- Haematuria appearing 24-72 hours after a sore throat or upper respiratory infection ("synpharyngitic haematuria")
- Low-grade fever
- Cola/brown coloured urine (not bright red)
- No or minimal oedema
- Possible mild proteinuria
Management (ER):
- Nephrology referral
- Serology: IgA levels, complement C3/C4, ANA, anti-dsDNA, ANCA, ASO titre
- 24-hour urine protein / urine PCR
- Monitor BP (hypertension worsens prognosis)
- Renal USS
- Renal biopsy is required for definitive diagnosis (shows IgA + IgG deposits in mesangial cells on immunofluorescence)
- No curative treatment; ACE inhibitors for proteinuria; steroids in selected cases
- Most patients maintain stable renal function; ~25% develop renal insufficiency over decades
Scenario D: Positive βhCG (pregnant) + above symptoms
DIAGNOSIS: UTI/Pyelonephritis in Pregnancy → HIGH RISK SITUATION
- Admit immediately
- IV ceftriaxone + IV fluids + obstetric consultation
- Monitor fetal heart rate if ≥ 24 weeks
- Avoid NSAIDs, fluoroquinolones, TMP-SMX in 3rd trimester
- Full management as per pyelonephritis in pregnancy protocol
Scenario E: Vaginal discharge + cervical excitation + fever + dysuria
DIAGNOSIS: STI (Chlamydia / Gonorrhoea + Urethritis / Pelvic Inflammatory Disease)
- Send: endocervical swab for gonorrhoea culture + NAAT for chlamydia
- Urine NAAT for chlamydia/gonorrhoea
- Treat empirically: Ceftriaxone 500 mg IM (single dose) + azithromycin 1 g oral (single dose) or doxycycline 100 mg BD x 14 days for chlamydia
- Contact tracing
Step 6: Red Flags That Change the Urgency
| Red Flag | Concern | Action |
|---|---|---|
| Loin pain + fever + CVA tenderness | Pyelonephritis | Admit + IV antibiotics |
| Rigors (shaking chills) | Bacteraemia / sepsis | Blood cultures + IV antibiotics within 1 hour |
| Hypotension or tachycardia | Septic shock | ICU / HDU level care |
| Dysmorphic RBCs + casts + proteinuria | Glomerulonephritis | Nephrology urgently |
| Positive pregnancy test | Pregnancy complication | Obstetrics involved |
| Adnexal mass / free fluid on USS | Ectopic pregnancy / TOA | Surgical emergency |
| Haematuria + weight loss + smoking history | Malignancy | Urology outpatient; CT urogram; cystoscopy |
| Oliguria / anuria + rising creatinine | Acute Kidney Injury | Nephrology urgent |
Summary: ER Management Algorithm
Young woman + Fever (past few days) + Hematuria + Dysuria
│
▼
IMMEDIATE
├── Vitals + sepsis screen
├── IV access if febrile/tachycardic
├── Urine dipstick + MSU (BEFORE antibiotics)
├── βhCG (mandatory)
└── Pelvic exam ± STI swabs if indicated
│
▼
BLOOD TESTS
FBC, CRP, creatinine, electrolytes, blood cultures (if febrile)
│
▼
URINE MICROSCOPY (KEY DECISION POINT)
│
├── Round RBCs + WBCs + bacteria
│ → UTI/Pyelonephritis
│ → Urine culture + antibiotics
│ ├── CVA tenderness + high fever → ADMIT + IV ceftriaxone
│ └── Suprapubic only + mild → Oral nitrofurantoin, discharge
│
├── Dysmorphic RBCs + RBC casts + proteinuria
│ → Glomerulonephritis (IgA, SLE, post-infectious)
│ → Nephrology referral + serology + renal USS
│ └── Consider renal biopsy
│
└── Round RBCs only (no infection)
→ Structural (stone, tumour)
→ Renal USS / CT KUB
→ Urology referral
Quick Reference - Common Diagnoses at a Glance
| Feature | Cystitis | Pyelonephritis | IgA Nephropathy |
|---|---|---|---|
| Fever | Low/absent | High (38.5°C+) | Low-grade |
| Flank pain | No | Yes (CVA tender) | No/mild |
| Dysuria | Prominent | Present | Mild |
| Hematuria | Common | Common | Cola-coloured |
| RBC morphology | Round | Round | Dysmorphic |
| RBC casts | No | No | Yes |
| Proteinuria | Mild | Mild | Significant |
| Trigger | None / sex | Preceding UTI | Recent URTI |
| Management | Oral antibiotics | IV antibiotics + admit | Nephrology referral |
Sources: Campbell Walsh Wein Urology (9780323546423); Rosen's Emergency Medicine (9780323757898); Creasy & Resnik's Maternal-Fetal Medicine (9780323828499)
This is a shared conversation. Sign in to Orris to start your own chat.