Nerve conduction study principle usage indications methodology disadvantages explain in detail with appropriate images and diagrams
Reading File
Finding Sources
Finding Sources
Searching the Web
nerve conduction study principle methodology indications NCS EMG
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks plus excellent diagrams. Let me compile the full detailed answer.
Nerve Conduction Study (NCS): Comprehensive Review
1. Principle
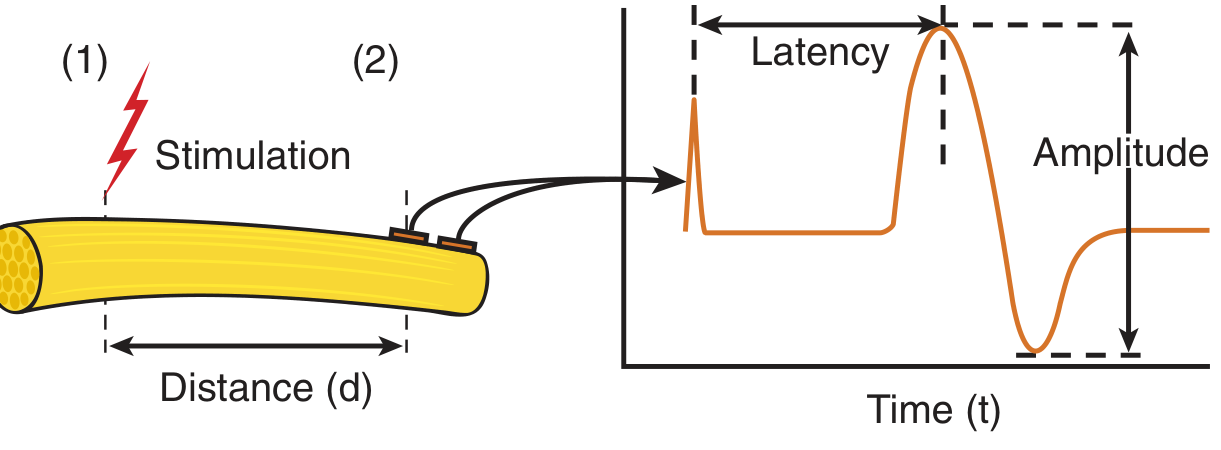
A nerve conduction study measures the electrical properties of peripheral nerves by applying a controlled electrical stimulus at one point on a nerve and recording the evoked electrical response at another point. The fundamental basis rests on the electrochemical properties of nerve membranes:
- Depolarization: When an electrical stimulus is applied to the nerve surface via the cathode (negative electrode), negative charges accumulate beneath it, depolarizing the axon membrane and generating an action potential.
- Propagation: This action potential propagates bidirectionally along the nerve fiber.
- Recording: Surface (or needle) electrodes placed at a defined distance downstream detect the traveling electrical wave.
The key measurable parameters derive from two physical quantities:
| Parameter | Definition | Unit |
|---|---|---|
| Latency | Time from stimulus to onset of response | Milliseconds (ms) |
| Conduction Velocity (CV) | Distance between two stimulation sites ÷ difference in latencies | Meters/second (m/s) |
| Amplitude | Height of the evoked potential | mV (motor) or µV (sensory) |
| Duration | Width of the negative phase of the potential | Milliseconds (ms) |
| Area | Area under the negative phase curve | mV·ms |
The formula for conduction velocity:
CV = Distance (mm) / [Proximal latency (ms) - Distal latency (ms)]
Normal ranges:
- Motor CV: 50-70 m/s in upper limbs; 40-60 m/s in lower limbs
- Sensory CV: slightly faster than motor in the same nerve
2. Types of NCS
A. Motor Nerve Conduction Study (MNCS)
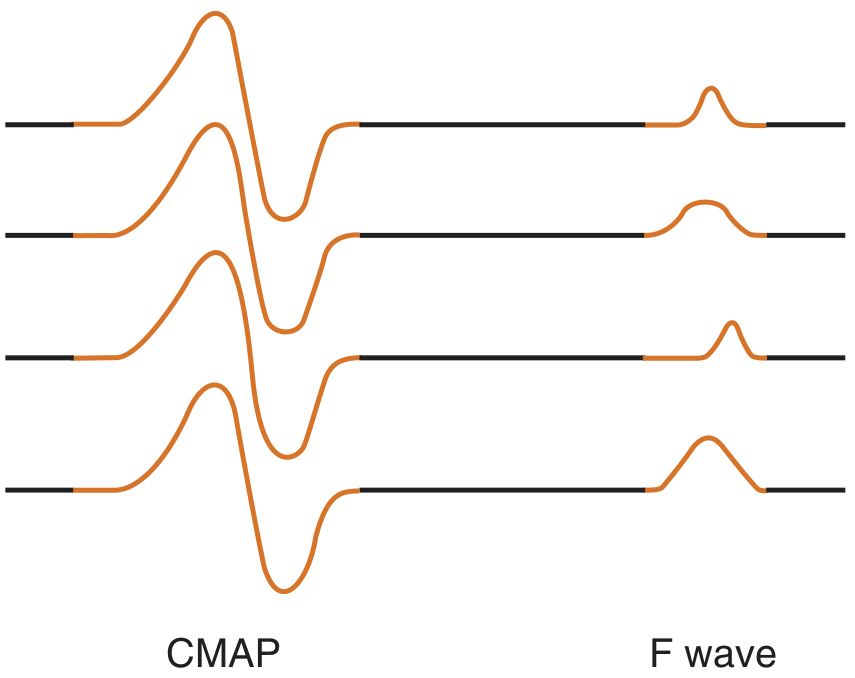
The motor nerve (or mixed nerve) is stimulated at two or more points along its course. The Compound Muscle Action Potential (CMAP) - also called the M wave - is recorded from a muscle innervated by that nerve using surface electrodes in a belly-tendon configuration (active electrode G1 over muscle belly, reference G2 over tendon). The CMAP represents the summated electrical activity of all activated muscle fibers under the recording electrode.
CMAP measures:
- Amplitude (baseline to negative peak, in mV): reflects the number of functional motor axons and muscle fiber integrity
- Duration (negative phase, in ms): reflects synchrony of conduction across all axons
- Area: more accurate than amplitude alone for assessing axonal loss
- Distal latency: time from distal stimulation to CMAP onset; reflects conduction in the fastest fibers of the distal segment plus neuromuscular transmission time
B. Sensory Nerve Conduction Study (SNCS)
A purely sensory or mixed nerve is stimulated and the Sensory Nerve Action Potential (SNAP) is recorded directly from the nerve (not muscle). Two techniques exist:
- Orthodromic: stimulate distally (e.g., digit), record proximally (e.g., wrist)
- Antidromic: stimulate proximally, record distally (larger amplitude; most commonly used clinically)
SNAP amplitude is measured in microvolts (much smaller than CMAP) and represents the number of sensory axons conducting between the stimulating and recording points. Because there is no neuromuscular junction amplification, SNAP amplitude is a very sensitive index of sensory axon loss.
Key CMAP vs SNAP differences:
| Feature | CMAP (Motor) | SNAP (Sensory) |
|---|---|---|
| Signal size | mV | µV |
| Amplification | Via muscle fibers | None |
| Affected by radiculopathy | Yes | No (DRG distal to root) |
| Sensitivity to axonal loss | Lower (reinnervation masks) | Higher |
| Stimulation sites needed for CV | ≥2 | 1 sufficient |
C. Mixed Nerve Conduction Study (MNAP)
Both motor and sensory fibers are assessed simultaneously by stimulating and recording from a mixed nerve trunk (e.g., median nerve at palm and wrist). Less commonly used in routine clinical practice.
3. Equipment and Electrode Setup
Stimulators
Two types are used:
- Constant voltage stimulator: regulates voltage; current varies inversely with skin-tissue impedance
- Constant current stimulator: adjusts voltage so the current reaching the nerve remains constant despite changes in skin resistance
In both types, a bipolar stimulator is used with:
- Cathode (negative, black): placed closer to the recording electrode - causes depolarization
- Anode (positive, red): placed 2-3 cm proximal to cathode - causes hyperpolarization (can cause anodal block if accidentally placed distally)
Supramaximal stimulation is required: the intensity is increased until the response stops growing, then increased by an additional 20-30% to ensure all available axons are depolarized.
Recording Electrodes
- Surface (skin) electrodes: used for routine CMAP and SNAP recording
- Needle electrodes: used when surface recording is inadequate (e.g., deep muscles, severe edema, obesity)
- G1 (active): placed over the motor point (muscle belly) or nerve recording site
- G2 (reference): placed over electrically inactive site (tendon or nearby bony area)
4. Special Studies: F Wave and H Reflex
F Wave
The F wave is a late motor response elicited when supramaximal stimulation of a motor nerve antidromically excites a small proportion of anterior horn cells, which then re-discharge orthodromically down the motor axon to the muscle. It evaluates the entire proximal-to-distal nerve pathway including nerve roots.
Key F wave parameters:
- Minimum F latency: the earliest latency among multiple F waves recorded (most sensitive to proximal slowing)
- Chronodispersion: difference between earliest and latest F wave latencies
- Persistence: percentage of stimuli that produce a recordable F wave
- F wave CV: useful when proximal slowing is suspected (e.g., early Guillain-Barré)
H Reflex
The H reflex (Hoffmann reflex) is the electrical analogue of the ankle jerk. It is recorded in the gastrocnemius-soleus after submaximal stimulation of the tibial nerve. It tests the S1 root reflex arc and is the most sensitive NCS parameter for early S1 radiculopathy.
5. Indications
NCS is indicated for evaluation of the peripheral nervous system, including:
Peripheral Neuropathies
- Symmetric polyneuropathies: diabetic, alcoholic, uremic, nutritional, toxic, hereditary (CMT), inflammatory (CIDP, GBS)
- Focal/multifocal neuropathies: vasculitic, multifocal motor neuropathy
Entrapment Neuropathies (most common indication)
- Carpal tunnel syndrome (median nerve at wrist) - most common
- Cubital tunnel syndrome (ulnar nerve at elbow)
- Tarsal tunnel syndrome
- Peroneal nerve compression at fibular head
- Meralgia paresthetica (lateral femoral cutaneous nerve)
Radiculopathies
- Cervical and lumbar radiculopathies (NCS is often normal in pure root lesions since the DRG is distal to the root; EMG adds diagnostic value)
- F waves and H reflexes are abnormal in severe root lesions
Plexopathies
- Brachial plexopathy (trauma, neuralgic amyotrophy, thoracic outlet syndrome, radiation-induced)
- Lumbosacral plexopathy
Mononeuropathies
- Traumatic nerve injuries (classification as neurapraxia vs. axonotmesis vs. neurotmesis)
- Monitoring recovery after peripheral nerve injury or surgery
Neuromuscular Junction Disorders
- Combined with repetitive nerve stimulation (RNS) for myasthenia gravis, Lambert-Eaton syndrome
Motor Neuron Disease
- To exclude peripheral nerve disease in ALS workup
Systemic Diseases with Nerve Involvement
- Amyloidosis, hypothyroidism, critical illness neuropathy, sarcoidosis, paraneoplastic neuropathy
6. Methodology - Step by Step
Step 1: Patient Preparation
- Patient is positioned comfortably; the limb to be tested is relaxed and supported
- Skin is cleaned with alcohol to reduce impedance
- Limb temperature is measured: nerve conduction is temperature-dependent (CV decreases ~2 m/s per °C drop); if limb temperature is below 32°C, warm the extremity before testing or apply a correction factor
- Skin-to-electrode impedance is checked (ideally <5 kΩ)
Step 2: Electrode Placement
- Recording electrodes (G1 and G2) placed per standard anatomical landmarks for each nerve
- Ground electrode placed between stimulating and recording electrodes to reduce stimulus artifact
- Stimulating electrode placed over the nerve, with cathode facing the recording site
Step 3: Stimulation
- Start with submaximal stimulation, gradually increase intensity
- Identify the threshold response, then increase to supramaximal (20-30% above plateau)
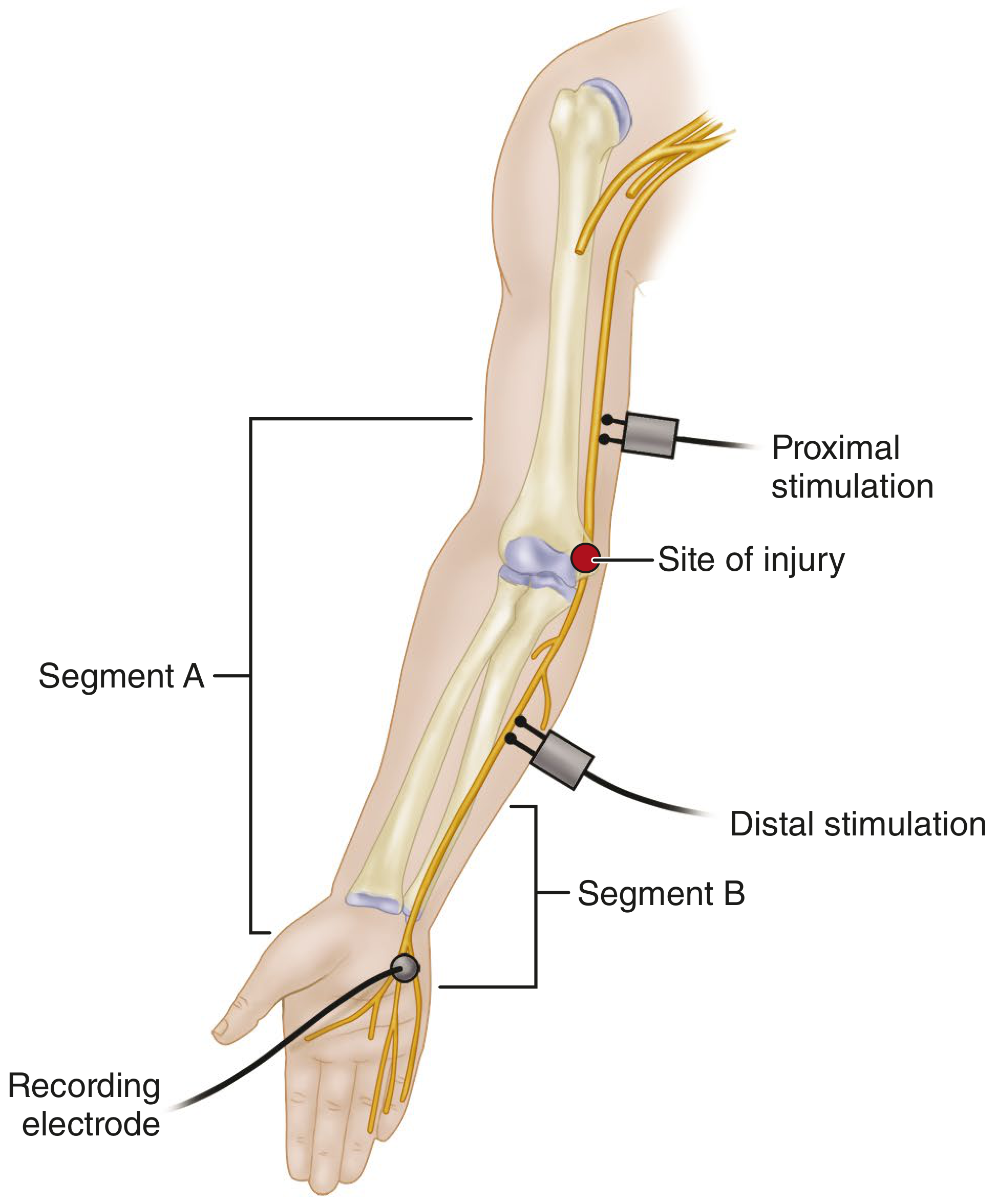
- Stimulate at distal site first, then proximal site(s)
Step 4: Recording and Measurement
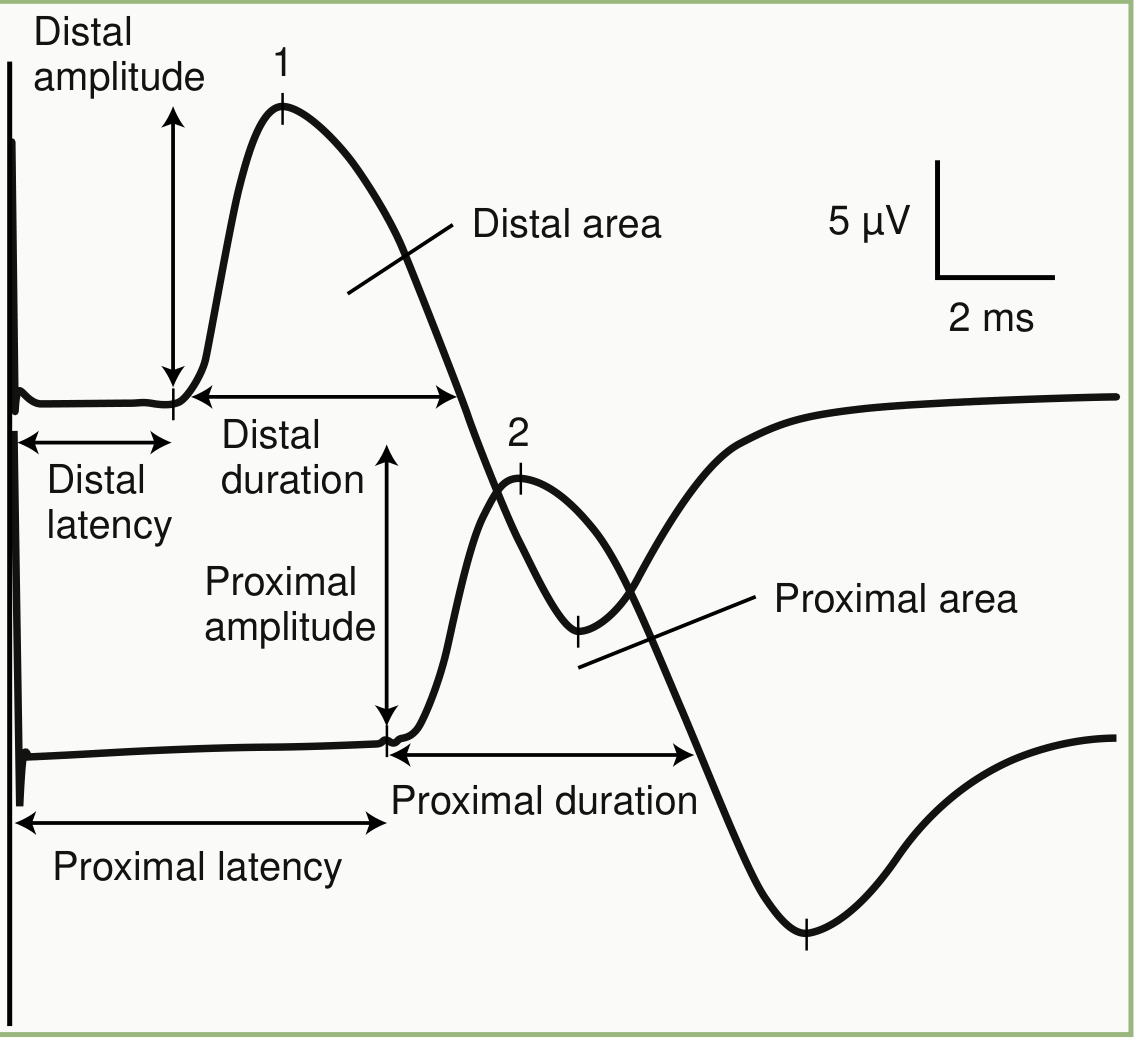
- For CMAP: measure distal latency, amplitude (baseline to negative peak), duration, and area from distal stimulation; then measure proximal latency to calculate CV
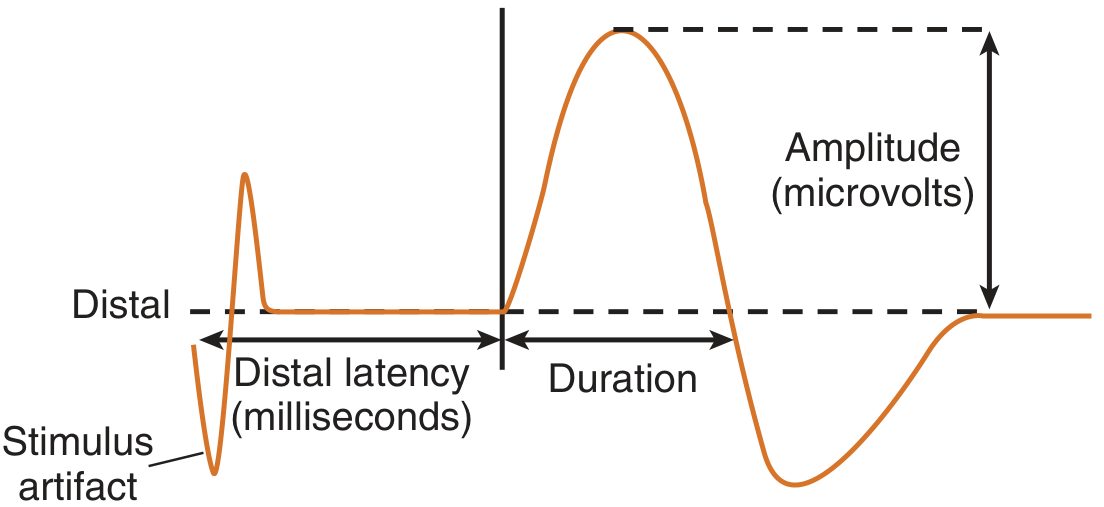
- For SNAP: measure onset latency (or peak latency), amplitude (baseline to negative peak or peak-to-peak), and duration
- Digital averaging used for low-amplitude SNAPs (signal-to-noise ratio improves with √n trials)
Step 5: F Wave Recording
- Nerve stimulated supramaximally at a distal site; multiple stimulations (minimum 10-20) given
- Late responses recorded and minimum latency identified
Step 6: Data Interpretation
Results are compared against age-, sex-, height-, and temperature-adjusted normative values. The pattern of abnormalities determines the diagnosis:
Demyelinating pattern (e.g., CIDP, GBS, entrapment):
- Prolonged distal latency
- Slowed conduction velocity (<75% lower limit of normal)
- Prolonged F wave latency
- Increased CMAP duration (temporal dispersion)
- Conduction block (>50% drop in CMAP amplitude proximal vs. distal)
- Relatively preserved amplitude early on
Axonal loss pattern (e.g., axonal neuropathy, severe entrapment):
- Reduced CMAP and/or SNAP amplitude
- Normal or minimally slowed CV (fast fibers preserved)
- Normal or mildly prolonged distal latency
- Wallerian degeneration distal to lesion after 5-10 days
7. Interpretation of Injury Patterns
After traumatic nerve injury, the NCS pattern evolves over time and helps classify the injury type:
| Injury Type | Proximal Stimulation | Immediately Post-injury (Distal) | 10 Days Post-injury (Distal) |
|---|---|---|---|
| Neurapraxia (demyelination only) | No response across lesion | Normal CMAP | Normal CMAP (distal axons intact) |
| Axonotmesis/Neurotmesis | No response | Normal initially | No response (Wallerian degeneration complete) |
- CMAP amplitude falls to its nadir 5-6 days after axonal injury
- SNAP amplitude falls to its nadir 10-11 days after axonal injury (NMJ failure accounts for the earlier CMAP drop)
8. Limitations and Disadvantages
Technical Limitations
- Temperature dependence: Cold limbs slow conduction and increase amplitude artifactually, mimicking or masking pathology. Strict temperature control is necessary.
- Operator dependence: Accurate electrode placement, distance measurement, and supramaximal stimulation require training and experience. Errors in distance measurement directly cause errors in CV calculation.
- Stimulus artifact: Large electrical artifacts from the stimulator can obscure early responses, especially short-distance SNAPs.
- Volume conduction: Potentials from distant muscles (via anomalous innervation or stimulus spread) can generate an initial positive deflection, indicating incorrect G1 placement.
- Anatomical variations: Anomalous innervation (e.g., Martin-Gruber anastomosis of median-ulnar in the forearm, occurring in ~15-30% of people) can produce misleading results if unrecognized.
Diagnostic Limitations
- Cannot assess small fibers: NCS evaluates only large myelinated A-alpha (motor) and A-beta (sensory) fibers. Small unmyelinated C fibers (pain, temperature) and thinly myelinated A-delta fibers cannot be assessed - normal NCS does not exclude small fiber neuropathy.
- Normal in pure radiculopathy: Because the dorsal root ganglion (DRG) lies distal to the nerve root, sensory axons remain intact in root lesions, making SNAPs normal. NCS cannot directly assess nerve roots.
- Cannot assess proximal nerve segments directly: Plexus and root segments are not directly accessible to percutaneous stimulation; F waves and H reflexes provide only indirect information.
- Limited in early disease: In the first 5-10 days after axonal injury, distal Wallerian degeneration is incomplete and the distal nerve remains excitable, masking the true extent of axonal loss.
- Does not assess neuromuscular junction directly: RNS and SFEMG are needed for NMJ disorders; routine NCS is insufficient.
- Low sensitivity for mild polyneuropathy: Subclinical or length-dependent polyneuropathies may show NCS changes only when nerve fiber loss is substantial.
Patient-Related Limitations
- Pain and discomfort: Electrical stimulation causes discomfort, particularly with supramaximal stimulation. It is poorly tolerated in children and anxious patients.
- Obesity and edema: Increased subcutaneous tissue distances reduce amplitude and may prevent adequate stimulation, making results unreliable.
- Lymphedema: Alters electrode-skin contact and tissue impedance.
- Pacemakers/implanted devices: Electrical stimulation near pacemakers requires caution (relative contraindication), though NCS is generally safe at standard intensities with proper precautions.
Interpretive Limitations
- Only evaluates fastest conducting fibers: CV reflects only the fastest-conducting (largest-diameter, most myelinated) fibers in the nerve. Selective loss of slow fibers may be missed.
- Temporal dispersion: With proximal stimulation, phase cancellation between faster and slower fibers causes a physiological reduction in SNAP/CMAP amplitude and prolongation of duration, which can be misinterpreted as pathological.
- Age, height, and sex affect normal values: Normal ranges must be adjusted; elderly patients and tall individuals normally have slower conduction in the legs.
9. Summary Comparison: Demyelination vs. Axonal Loss
| NCS Parameter | Demyelination | Axonal Loss |
|---|---|---|
| Conduction velocity | Markedly slowed | Normal or mildly slowed |
| Distal latency | Prolonged | Normal or mildly prolonged |
| Amplitude | Normal early; may drop with conduction block | Reduced (proportional to axon loss) |
| Duration | Increased (temporal dispersion) | Normal |
| Conduction block | Present | Absent (uniform loss) |
| F wave | Prolonged/absent | May be prolonged or absent |
Sources:
- Bradley and Daroff's Neurology in Clinical Practice, 8th Ed., Ch. 36 - Clinical Electromyography
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed., Ch. 224 - Nerve Conduction Studies
- Campbell's Operative Orthopaedics, 15th Ed. 2026, Ch. 67 - Nerve Conduction Velocity
- Adams and Victor's Principles of Neurology, 12th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.