I now have comprehensive information from the textbooks. Let me compile the full answer.
Lipid Profile
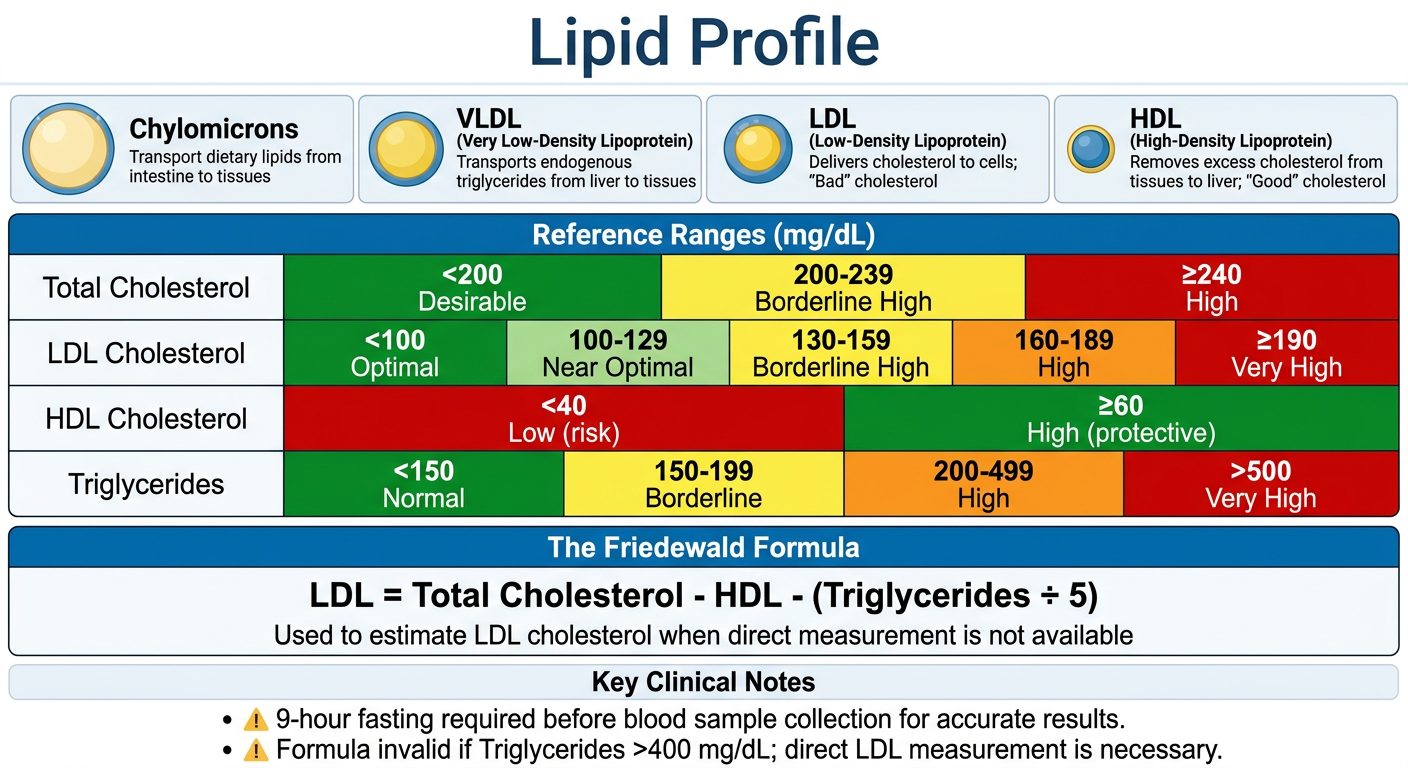
A lipid profile (also called a lipid panel or fasting lipid panel) is a blood test used to evaluate cardiovascular disease (CVD) risk. It measures four main components: total cholesterol, LDL cholesterol, HDL cholesterol, and triglycerides.
Components and Reference Ranges
Based on the NCEP ATP III classification (Berek & Novak's Gynecology, Table 22-6; Textbook of Family Medicine 9e):
Total Cholesterol
| Value | Classification |
|---|
| < 200 mg/dL | Desirable |
| 200-239 mg/dL | Borderline high |
| ≥ 240 mg/dL | High |
LDL Cholesterol (Low-Density Lipoprotein)
| Value | Classification |
|---|
| < 100 mg/dL | Optimal |
| 100-129 mg/dL | Near/above optimal |
| 130-159 mg/dL | Borderline high |
| 160-189 mg/dL | High |
| ≥ 190 mg/dL | Very high |
HDL Cholesterol (High-Density Lipoprotein)
| Value | Classification |
|---|
| < 40 mg/dL | Low (increased CVD risk) |
| ≥ 60 mg/dL | High (protective) |
Triglycerides
| Value | Classification |
|---|
| < 150 mg/dL | Normal |
| 150-199 mg/dL | Borderline high |
| 200-499 mg/dL | High |
| > 500 mg/dL | Very high |
The Four Major Lipoprotein Classes
- Chylomicrons - Transport dietary (exogenous) triglycerides from intestine to peripheral tissues
- VLDL (Very-Low-Density Lipoprotein) - Transport endogenous triglycerides from liver to peripheral tissues
- LDL (Low-Density Lipoprotein) - Carries 60-70% of plasma cholesterol; directly associated with increased CHD risk
- HDL (High-Density Lipoprotein) - Carries 20-30% of total cholesterol; performs reverse cholesterol transport back to liver (protective). Carries apolipoprotein A-1. For every 1 mg/dL decrease in HDL, CAD risk increases 2-3%.
- Textbook of Family Medicine 9e, p. 234
How LDL is Calculated
The standard panel measures total cholesterol, HDL, and triglycerides directly, then uses the Friedewald formula to calculate LDL:
LDL = Total Cholesterol - HDL - (Triglycerides / 5)
The formula is NOT valid when:
- Chylomicrons are present (non-fasting sample)
- Triglycerides > 400 mg/dL (leads to underestimation of LDL)
- Dysbetalipoproteinemia (type III hyperlipidemia) is present
In these cases, a direct LDL measurement should be ordered.
- Textbook of Family Medicine 9e, p. 234
Pre-Test Conditions and Sources of Variation
-
A 9-hour fast is required for the standard panel (fasting elevates triglycerides; affects LDL calculation)
-
Total cholesterol and HDL are reliable even in non-fasting state
-
Stable diet for 3 weeks before testing is recommended (dietary changes appear in ~1-2 weeks)
-
Morning specimens are preferred (triglycerides show diurnal variation - lowest in morning)
-
Recent illness/surgery/MI/stroke can lower lipids for several weeks; wait 2-3 months after major illness
-
Cholesterol drops 24 hours after MI and stays low up to 12 weeks
-
Textbook of Family Medicine 9e, p. 234
Drugs That Affect Lipid Values
| Drug | Total Cholesterol | LDL | HDL | Triglycerides |
|---|
| Thiazide diuretics | ↑ | ↑ | -- | ↑ |
| Beta-blockers | -- | -- | ↓ | ↑ |
| Alpha-blockers | ↓ | ↓ | ↑ | ↓ |
| ACE inhibitors | -- | -- | -- | -- |
| Calcium-channel blockers | -- | -- | -- | -- |
| Unopposed estrogens | ↓ | ↓ | ↑ | ↑ |
| Unopposed progestogens | -- | ↑ | ↓ | ↓ |
| Isotretinoin | ↑ | ↑ | --/↓ | ↑ |
| Protease inhibitors | ↑ | -- | -- | ↑ |
| Tamoxifen | ↓ | ↓ | -- | ↑ |
- Textbook of Family Medicine 9e, Table 14-13, p. 235
Other Factors Affecting Cholesterol
-
Age/Sex: Before age 50, women have lower lipid values than men; after 50, women's levels tend to exceed men's (modified by exogenous estrogen)
-
Seasonal variation: Lipid levels in December/January are ~2.5% higher than June/July
-
Obesity/Diet: Weight reduction in an obese patient can decrease triglycerides by up to 40%; total cholesterol and LDL decrease < 10% with diet alone
-
Secondary causes of dyslipidemia: hypothyroidism, diabetes mellitus, chronic kidney disease, nephrotic syndrome, liver disease
-
Berek & Novak's Gynecology, p. 1067-1068
Non-HDL Cholesterol
Non-HDL cholesterol = Total Cholesterol - HDL. This includes LDL + VLDL + IDL + lipoprotein(a). The
AHA considers non-HDL cholesterol a reliable risk marker that doesn't require fasting and may be as predictive as LDL particle number.
When to Screen
The NCEP ATP III recommends lipid screening to promote CVD risk reduction. Screening is part of routine metabolic workups along with CBC, CMP, HbA1c, and other baseline labs in multiple clinical contexts (diabetes management, pre-medication screening for statins, immunosuppressants, isotretinoin, etc.).