Tennis elbow
Reading File
Finding Sources
Finding Sources
Searching PubMed
"lateral epicondylitis" treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Here is a comprehensive overview of tennis elbow (lateral epicondylitis):
Tennis Elbow (Lateral Epicondylitis)
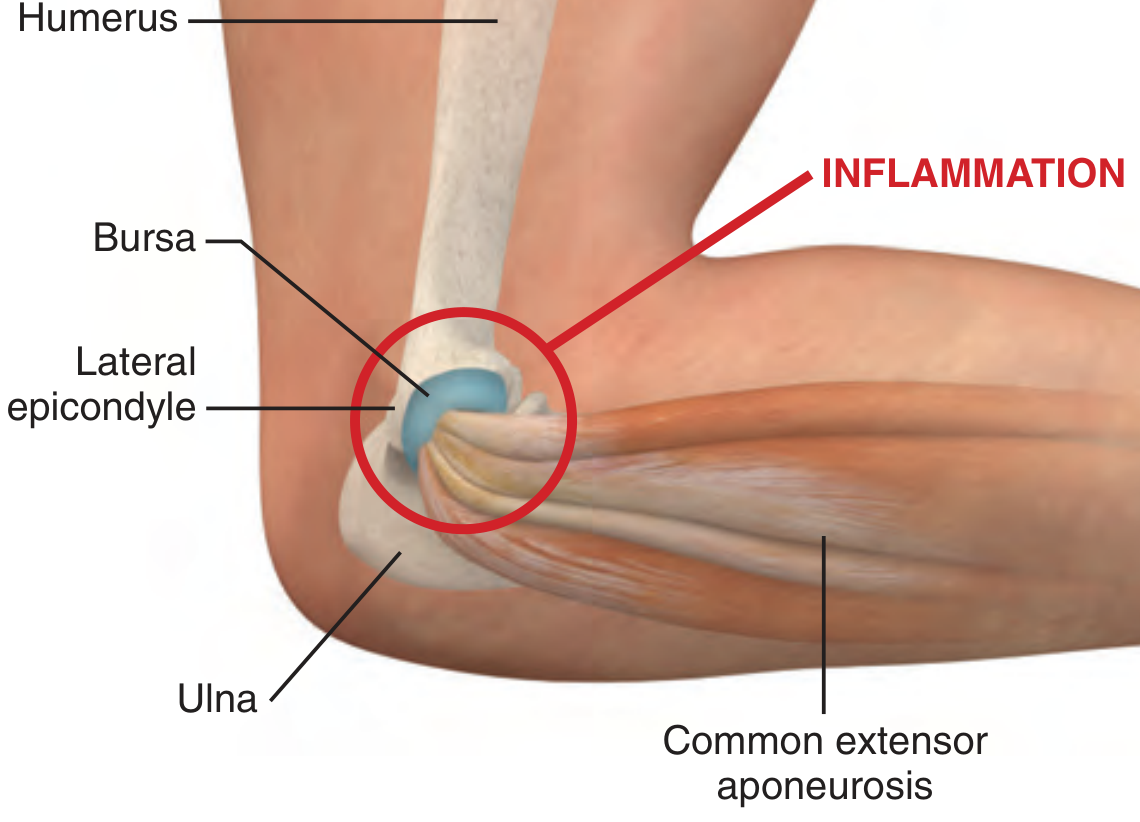
Definition & Anatomy
Tennis elbow is a painful degenerative condition at the origin of the extensor carpi radialis brevis (ECRB) on the lateral epicondyle of the humerus. Despite the name, fewer than 5% of patients actually play tennis — it is far more common in manual workers (prevalence approaching 14.5% in the workforce), and arises from repetitive activities such as turning screws, using a wrench, gardening, or assembly line work.
- Rosen's Emergency Medicine, 10th ed.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Pathophysiology
Although "epicondylitis" implies inflammation, histological examination consistently shows angiofibroblastic hyperplasia (also called angiofibroblastic tendinosis) — a degenerative process with a paucity of acute inflammatory cells. It is now better classified as a tendinopathy rather than true tendinitis.
- Miller's Review of Orthopaedics, 9th ed.
Clinical Features
Symptoms:
- Dull ache along the lateral aspect of the elbow, over the lateral epicondyle or radiohumeral joint
- Pain exacerbated by grasping, twisting, wrist extension or supination
Examination findings:
-
Tenderness just distal (5–10 mm) to the lateral epicondyle, at the ECRB origin
-
Cozen's test (resisted wrist extension with forearm stabilized) — reproduces lateral epicondyle pain; sensitivity ~74%, poor specificity
-
Maudsley's test (resisted extension of the middle finger with elbow in extension) — reproduces pain at the lateral epicondyle; sensitivity ~54%, also poor specificity
-
Rosen's Emergency Medicine; Bailey and Love's Short Practice of Surgery, 28th ed.
Investigations
- Plain radiographs: Usually normal; ~20% show tendon calcification or reactive exostosis at the epicondyle tip. Useful to exclude fractures in atypical or prolonged cases.
- MRI: Characteristic findings described but not indicated emergently.
- Differential diagnosis: Posterior interosseous nerve entrapment, radiohumeral bursitis, plica lesions, synovitis, chondromalacia, osteochondral defects.
Management
Conservative (first-line)
| Measure | Notes |
|---|---|
| Activity modification | Avoid inciting activities |
| RICE + immobilization | Sling initially; analgesics |
| NSAIDs | Useful for analgesia, not anti-inflammatory effect per se |
| Physical therapy | Stretching, strengthening; superior to corticosteroid at 6 weeks and beyond |
| Counterforce brace | May reduce tendon load |
Corticosteroid Injection
- Provides short-term pain relief (superior to NSAIDs and physiotherapy for the first 6 weeks)
- After 6 weeks, physical therapy becomes more effective
- Do not inject directly into the tendon — corticosteroids weaken collagen
- Avoid subcutaneous injection (risk of skin depigmentation/atrophy)
- No clear long-term benefit — Miller's Review of Orthopaedics notes "no clear benefit from corticosteroid injection" overall
Emerging / Other Treatments
- Platelet-rich plasma (PRP): Growing evidence; recent meta-analyses (2025) suggest PRP may outperform corticosteroid for longer-term outcomes in tendinopathy (PMID 40200209)
- Extracorporeal shockwave therapy (ESWT): Systematic review (2024) suggests ESWT is at least comparable to corticosteroid injection for chronic lateral epicondylitis (PMID 39198038)
- Dry needling: Updated meta-analysis (2024) supports therapeutic benefit (PMID 38484834)
Surgery
Reserved for recalcitrant cases failing prolonged conservative management (typically >6 months). Open and arthroscopic approaches show equivalent results. The procedure involves debridement/release of the ECRB origin.
- Miller's Review of Orthopaedics, 9th ed.
Summary
| Feature | Detail |
|---|---|
| Site | Lateral epicondyle (ECRB origin) |
| Pathology | Angiofibroblastic tendinosis (degenerative) |
| Key test | Cozen's / Maudsley's |
| First-line Rx | Activity modification, PT, NSAIDs |
| Injection | Short-term benefit only |
| Surgery | Last resort for recalcitrant cases |
This is a shared conversation. Sign in to Orris to start your own chat.