Describe the role of sialendoscopy in various salivary gland disease in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
sialendoscopy salivary gland
Searching the Web
sialendoscopy salivary gland disease RGUHS ENT 50 marks role indications technique
Reading File
Finding Sources
Finding Sources
Searching PubMed
sialendoscopy juvenile recurrent parotitis Sjogren radioiodine
Reading File
Reading File
Searching PubMed
sialendoscopy technique outcome complications
Reading File
Reading File
Reading Article
Reading Article
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading Article
Generating Image
Generating Image
I now have all the material needed for a comprehensive answer. Let me compose the full detailed response.
ROLE OF SIALENDOSCOPY IN SALIVARY GLAND DISEASES
(RGUHS ENT - 50 Marks Long Answer)
Sources: Cummings Otolaryngology (7th ed.), Scott-Brown's Otorhinolaryngology HNS, KJ Lee's Essential Otolaryngology, and recent systematic reviews
I. INTRODUCTION
Sialendoscopy represents one of the most significant advances in the management of salivary gland diseases over the past three decades. Introduced in the early 1990s by Marchal and colleagues, it is a minimally invasive, gland-preserving endoscopic technique that allows both diagnostic visualization and therapeutic intervention within the major salivary duct systems - primarily the parotid (Stensen) duct and the submandibular (Wharton) duct - through their natural transoral orifices.
Prior to sialendoscopy, the standard surgical options for most salivary gland obstructive diseases were submandibular gland excision (with risks of marginal mandibular nerve injury, lingual nerve injury) or parotidectomy (with facial nerve risk). Sialendoscopy has transformed the paradigm: today, using endoscopic and combined/hybrid techniques, a safe, effective, gland-preserving alternative is achievable with success rates of 80-100% (Cummings, 7th ed., Ch. 83).
II. ANATOMY RELEVANT TO SIALENDOSCOPY
Wharton's Duct (Submandibular):
- Length: 5-6 cm; diameter: 1.5-3 mm
- Opens at the sublingual papilla lateral to the frenulum
- Right-angle bend over posterior edge of mylohyoid is the most common site of stone impaction
- More amenable to sialendoscopy due to larger caliber and dependent drainage
Stensen's Duct (Parotid):
- Length: ~6 cm; diameter: 1-3 mm
- Opens opposite upper 2nd molar
- Tortuosity makes instrumentation more technically demanding
- Prone to stricture formation after manipulation - stenting often required
III. THE SIALENDOSCOPE - INSTRUMENTATION
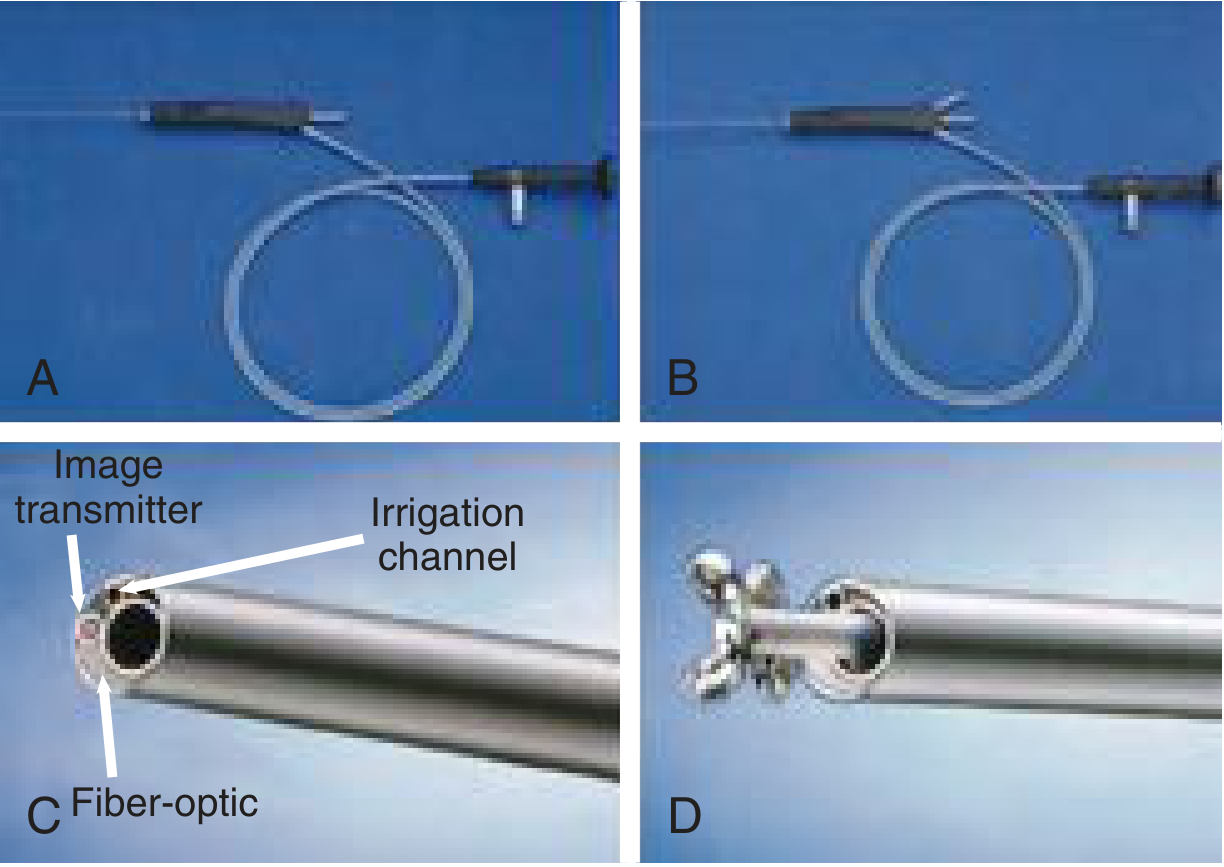
Sialendoscopes come in three categories based on rigidity:
| Feature | Flexible | Semirigid | Rigid |
|---|---|---|---|
| Diameter | 0.8-1.1 mm | 0.8-1.6 mm | 1.1-1.6 mm |
| Navigation | Easy in curves | Moderate | Difficult in bends |
| Working channel | Limited | Yes (>1.1mm) | Yes |
| Stone retrieval | Limited | Yes | Yes |
The Erlangen (Karl Storz) zero-degree telescope is the most widely used system, available in three sizes:
- 0.8 mm - diagnostic only (light + image + irrigation, no working channel)
- 1.1 mm - working channel allows microdrill, laser fiber, balloon dilator
- 1.6 mm - full instrumentation; occasionally too large for small pediatric patients
Working channel instruments available:
- Wire basket - for stone extraction (Dormia-type, 3-4 wire)
- Balloon dilator - for ductal strictures (high-pressure)
- Holmium:YAG laser fiber - for stone fragmentation (lithotripsy)
- Pneumatic/hydraulic lithotripter - intraductal fragmentation
- Microdrill - for large impacted stones
- Salivary stent - for post-dilation stenosis prevention
IV. FLOWCHART: SIALENDOSCOPY DECISION ALGORITHM
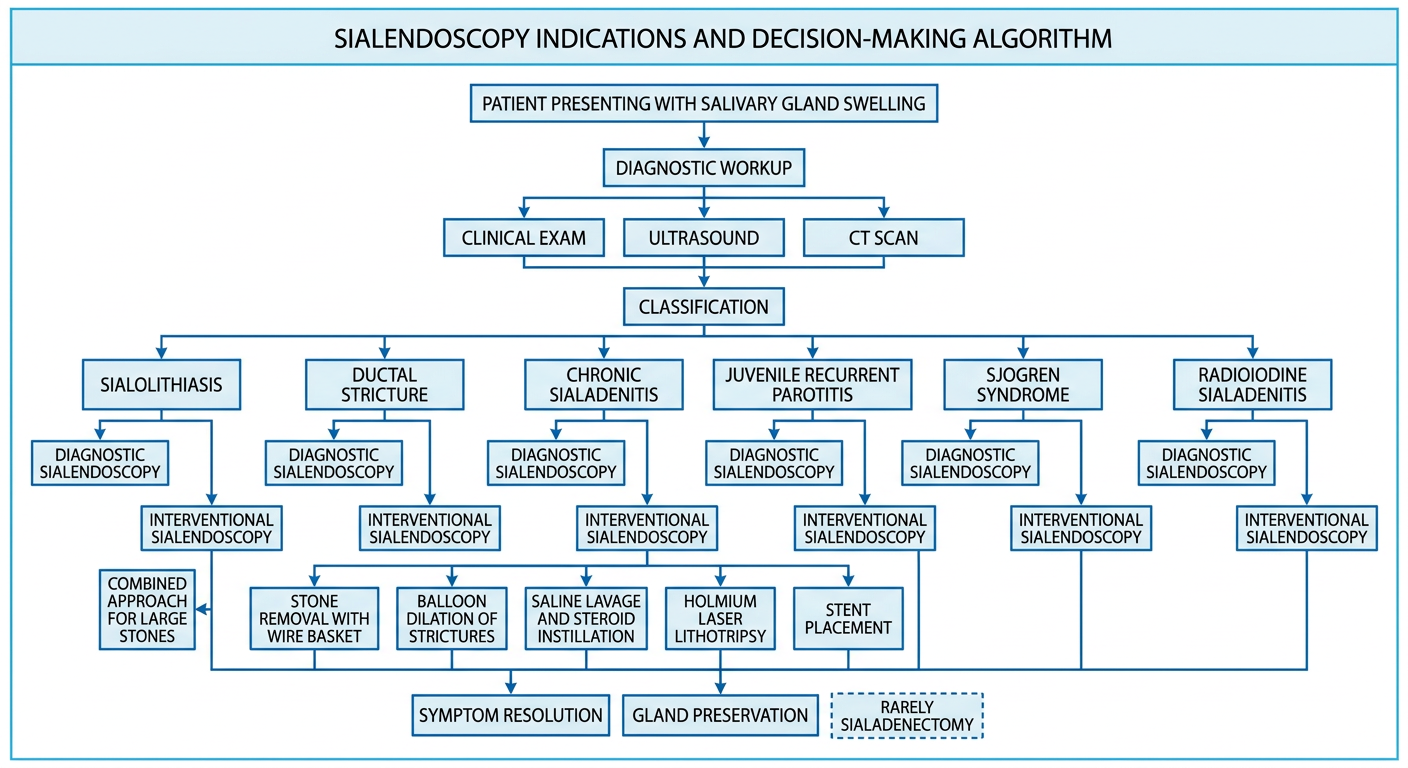
Fig. 2: Decision algorithm for sialendoscopy in salivary gland disease
V. ANATOMY DIAGRAM - SIALENDOSCOPY TECHNIQUE
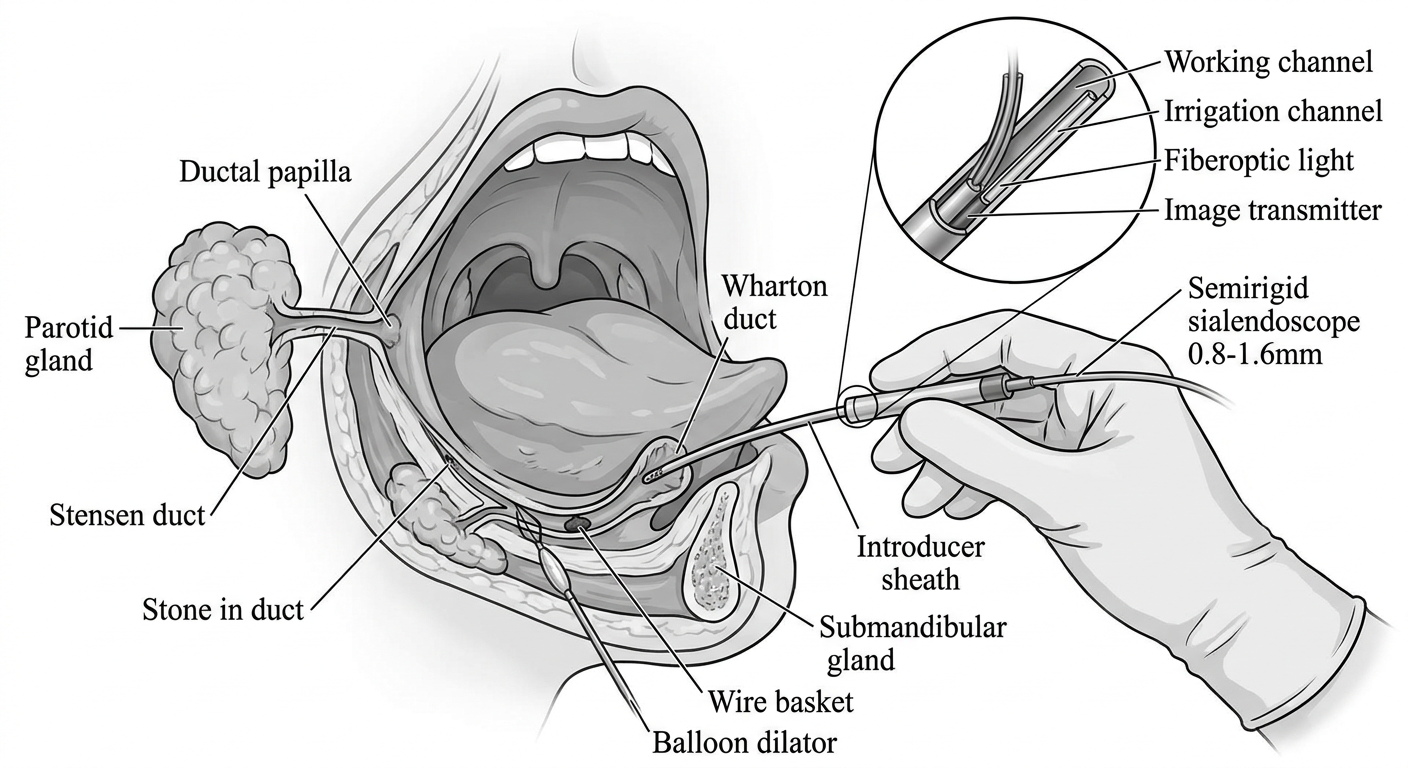
Fig. 3: Sialendoscope inserted through introducer sheath in cannulated papilla of submandibular duct
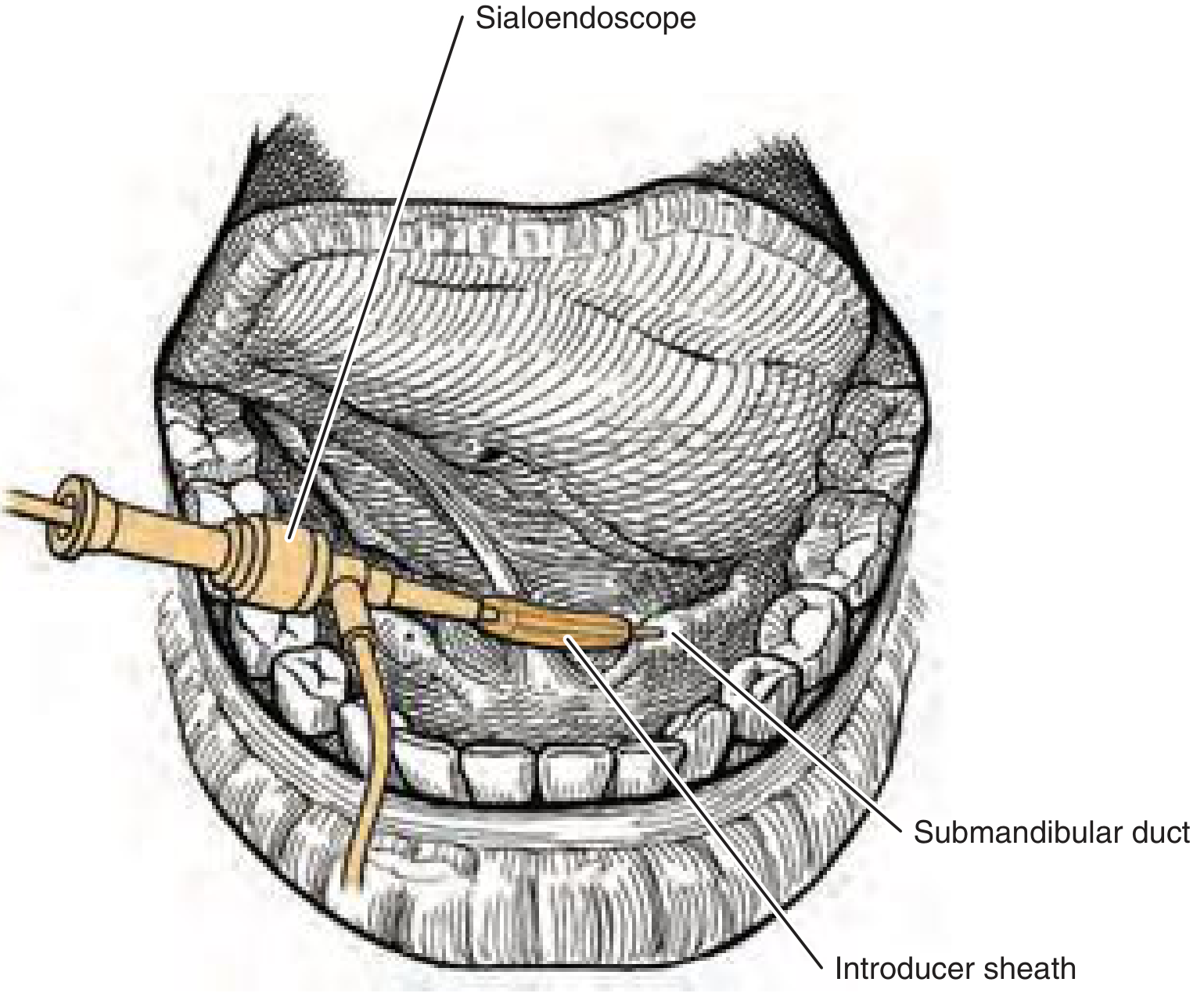
Fig. 4: Sialendoscope inserted through introducer sheath in cannulated papilla of submandibular duct (Cummings, Fig. 83.3)
VI. TECHNIQUE OF SIALENDOSCOPY
Patient Preparation
- Anesthesia: General anesthesia is standard; local anesthesia may be used in cooperative adults and children >8 years
- Position: Supine with head slightly extended
- Equipment: Bite block on contralateral side; salivary duct probe set; dilators; sialendoscope; camera system; irrigation saline; light source
Step-by-Step Operative Technique
STEP 1: Identification of ductal papilla
↓
STEP 2: Serial dilation using salivary duct probes (Bowman probes 000 → 4)
↓
STEP 3: Insertion of introducer sheath
↓
STEP 4: Introduction of sialendoscope into dilated orifice
↓
STEP 5: Exploration under continuous saline irrigation (maintains lumen,
flushes debris, allows visualization)
↓
STEP 6: Advance to first branching point; explore each branch
↓
STEP 7: Identify pathology (stone, stricture, mucus plug, abnormal mucosa)
↓
STEP 8: Therapeutic intervention (basket, balloon, laser, lavage)
↓
STEP 9: Stent placement if indicated (2-4 weeks) → prevents re-stricture
↓
STEP 10: Post-op: sialagogues, hydration, antibiotics if needed
Normal Sialendoscopic Appearance:
- Pink-white ductal wall
- Normal vascular markings (fine branching vessels visible)
- Clear lumen
Abnormal Findings:
- Sialolith: Yellowish-white, hard, fixed or mobile mass
- Stricture: Narrowing, blanched walls, loss of vascular markings
- Chronic sialadenitis: Mucus plugs, whitish debris, dilated ducts
- JRP: Whitish particles (mucoid), punctate sialectasis appearance
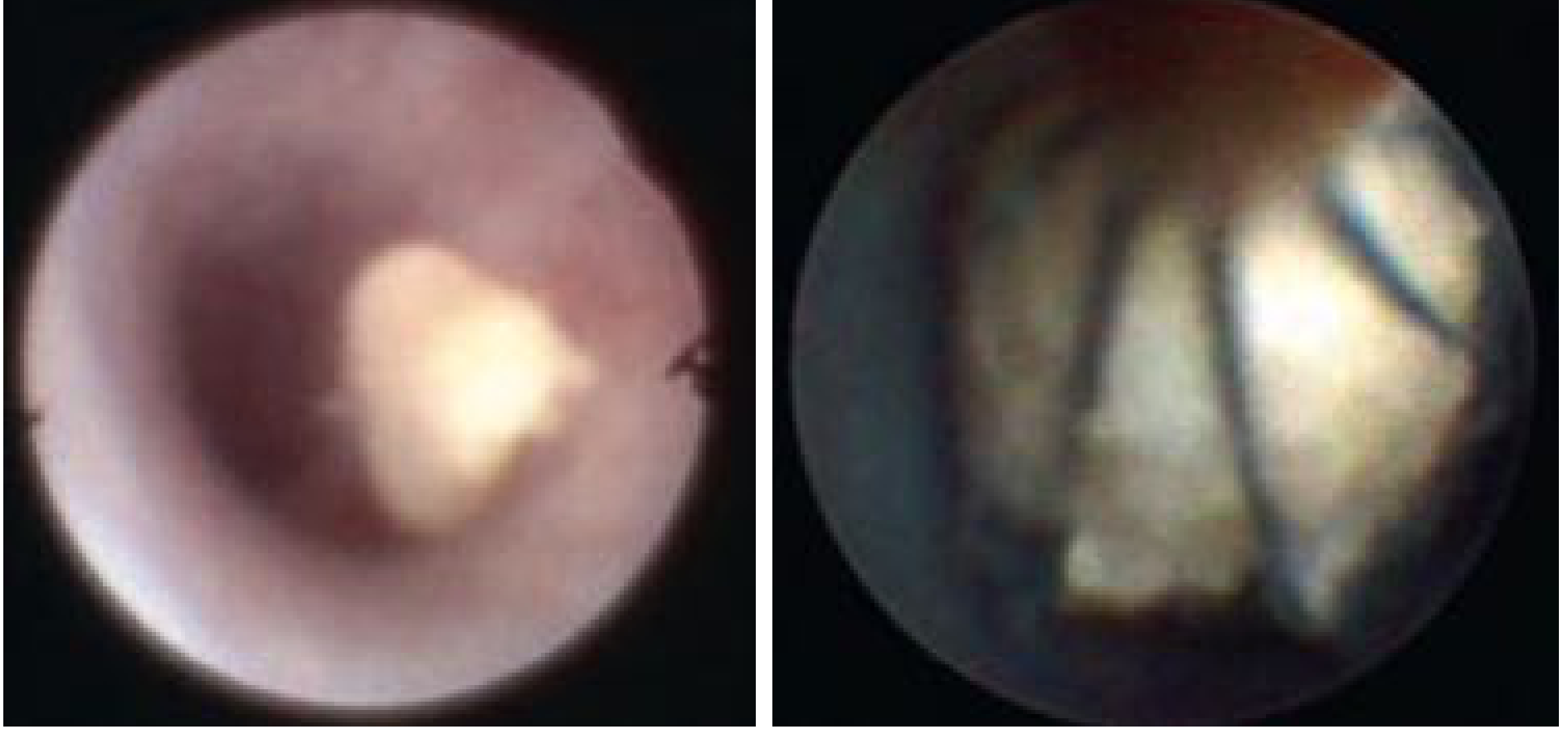
Fig. 5: Sialendoscopic view - stone in duct (left) before grasping; wire basket removal of stone (right). (Cummings, Fig. 83.4)
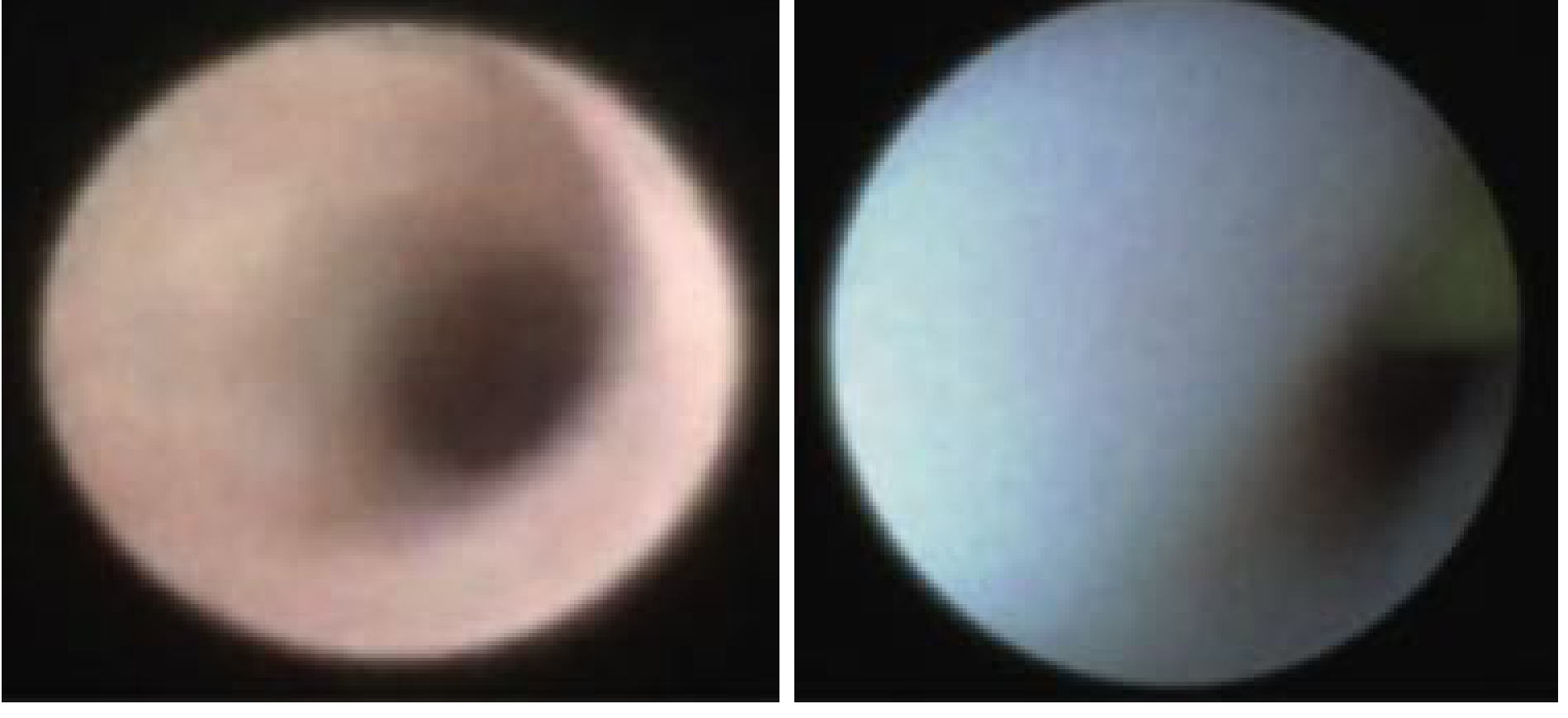
Fig. 6: Endoscopic view - normal salivary duct (left) vs blanched, narrowed duct with loss of normal vascular markings in chronic sialadenitis (right). (Cummings, Fig. 83.9)

Fig. 7: Stone-extractor wire basket containing a submandibular stone removed by sialendoscopy. (Cummings, Fig. 205.12)
VII. INDICATIONS FOR SIALENDOSCOPY
Per Cummings (7th ed.) and Scott-Brown's:
A. DIAGNOSTIC Indications
- Unexplained recurrent salivary gland swelling
- Sialolithiasis (confirmation + localization when imaging inconclusive)
- Ductal anatomy assessment before surgery
- Suspected ductal polyp or foreign body
- Investigation of unexplained xerostomia in autoimmune disease
B. THERAPEUTIC Indications
| Condition | Sialendoscopy Role |
|---|---|
| Sialolithiasis | Stone retrieval, fragmentation |
| Ductal strictures | Balloon dilation, stent placement |
| Chronic sialadenitis | Lavage, steroid instillation |
| Juvenile Recurrent Parotitis (JRP) | Ductal washout, steroid irrigation |
| Sjögren syndrome | Dilation, lavage, steroid instillation |
| Radioiodine-induced sialadenitis | Washout, debris removal, dilation |
| Mucus plugs | Retrieval, lavage |
| Ductal kinks | Balloon dilation |
| Sialodochitis fibrinosa | Fibrin plug retrieval |
Contraindications:
- Acute suppurative sialadenitis (absolute - risk of perforation, sepsis spread)
- Trismus (relative - cannot access papilla)
- Untreated coagulopathy
- Recent ductal surgery with scarring at papilla (relative)
VIII. ROLE IN SPECIFIC DISEASES
A. SIALOLITHIASIS (SALIVARY CALCULI)
Sialolithiasis accounts for 50-66% of all presentations of salivary gland obstruction (Scott-Brown's, Vol. 2, Ch. 45). The submandibular gland is affected in ~80% of cases due to alkaline mucous secretion, longer tortuous duct, and dependent drainage against gravity.
Sialendoscopic Management Algorithm:
Stone confirmed on imaging (US/CT)
|
↓
Determine stone characteristics:
Size: <4mm / 4-8mm / >8mm
Location: Distal / Mid / Proximal / Intraglandular
Mobility: Mobile / Impacted
|
↓
┌──┴──┐
<4mm 4-8mm >8mm
Mobile ±impacted or impacted
| | |
↓ ↓ ↓
Wire basket Holmium Combined approach:
retrieval laser Endoscopy-guided
alone fragmentation transoral incision
| or parotidectomy
↓ approach + stone
Basket removal removal
of fragments
|
↓
Stent placement 2-4 weeks (Parotid especially)
|
↓
Success rate: 89.6% for sialolithiasis
(Beumer et al., Oral Dis 2024; 91 studies, 8218 patients)
Endoscopic approach limitations:
- Stones >4-5 mm in the parotid duct are often too large for basket extraction alone and require laser fragmentation first
- Submandibular success rate: 88.3% vs. parotid: 81.2% (Beumer et al., 2024)
- Endoscopic-assisted transoral removal: 86.3%
- Combined approach parotid: 78.2%
Per Cummings: "Salivary endoscopy has caused a paradigm shift in the management of salivary stones. Today, using a combination of endoscopic techniques combined with transoral or external approaches, it is possible to provide a safe, effective, gland-preserving alternative with success rates between 80% and 100%."
B. DUCTAL STRICTURES (STENOSIS)
Strictures account for a significant proportion of chronic obstructive salivary disease. They may be primary (idiopathic) or secondary to stone passage, infection, external trauma, radiation, or post-procedural scarring.
Classification by severity:
- Grade I: Mild narrowing, easily negotiated
- Grade II: Moderate - requires balloon dilation
- Grade III: Severe - requires balloon + stent
- Grade IV: Complete obliteration - endoscopic approach may fail
Sialendoscopic treatment:
- Balloon dilation using high-pressure balloon dilators passed through the working channel
- Stent placement (polyethylene or silicone stent, 2-6 weeks duration)
- Prevents re-stricture after dilation
- Success rate for stenoses: 56.3% (Beumer et al., 2024 meta-analysis; lower than sialolithiasis due to recurrence)
- Repeated sessions may be required
Salivary stent left in place for 2-4 weeks after dilation prevents stricture recurrence (Cummings, Ch. 83).
C. CHRONIC SIALADENITIS (RECURRENT PAROTITIS IN ADULTS / CHRONIC OBSTRUCTIVE SIALADENITIS)
Chronic sialadenitis - most commonly in the parotid gland - results from obstructive ductal pathology, mucus plugging, and secondary infection leading to cycles of inflammation and fibrosis.
Sialendoscopic findings: Blanched ductal walls, loss of normal vascular markings, mucus plugs, strictures, whitish secretions (Fig. 83.9, Cummings).
Therapeutic mechanism:
Per Cummings: "Diagnostic endoscopy can improve symptoms by washing out the salivary ducts with a continuous normal saline lavage, intraglandular steroid instillation, and hydrostatic dilation of the ductal system."
Protocol:
- Ductal dilation
- Saline lavage (continuous irrigation, removes debris)
- Steroid instillation - Triamcinolone acetonide 40 mg diluted in 3-5 mL normal saline - instilled at end of procedure (anti-inflammatory effect on ductal mucosa)
- Stent if stricture present
- Antibiotic irrigation (gentamicin/ampicillin) if infection suspected
Sialography (historical) using iodinated oil also has therapeutic effect - antiseptic effect, mechanical dilation - but now largely replaced by sialendoscopy.
D. JUVENILE RECURRENT PAROTITIS (JRP)
JRP is characterized by recurrent episodes of unilateral or bilateral painful parotid swelling in children (peak age 3-6 years and second peak at puberty). It is the most common non-infectious inflammatory salivary gland disease in children.
Pathogenesis: Idiopathic; postulated mechanisms include ductal hypoplasia, mucus plugging, immune dysregulation. Sialendoscopy reveals characteristic "snowflake" appearance - white particles and inspissated secretions - and punctate sialectasis.
Sialendoscopy as primary treatment:
Per Cummings pediatric section: "In a recent systematic review of pediatric sialendoscopy, JRP was the most frequent indication (68.9%), followed by sialolithiasis (14.7%)."
The Soriano-Martin systematic review (2023, PMID 37598195):
- 524 patients, 646 sialendoscopies
- Sialendoscopy was 74.9% effective as primary treatment in prevention of recurrent symptoms
- Mean recurrence rate: 25.1% (95% CI 23.6-26.6%)
- Type of ductal irrigation (saline alone vs. corticosteroids vs. corticosteroids + antibiotics) did not significantly influence recurrence
- Significant relationship between frequency of pre-op attacks and post-op recurrences (p<0.05)
Irrigation protocol for JRP:
- Saline washout + corticosteroid (triamcinolone/hydrocortisone) instillation
- Most procedures done under general anesthesia in children
- Can be done under local anesthesia in children >8 years who cooperate
- May require repeat procedures (2-3 sessions)
- Virtually all cases resolve spontaneously at puberty - surgical intervention rarely needed
Flowchart: JRP Management:
Recurrent parotid swelling in child (age 3-6 years)
|
↓
Clinical assessment + Ultrasound
(punctate sialectasis = pathognomonic)
|
↓
Acute episode? ──Yes──→ Conservative: antibiotics,
| sialagogues, hydration, warm compress
No
↓
Recurrent (≥2 episodes/year)?
|
Yes
↓
Sialendoscopy
(diagnostic + therapeutic)
- Ductal washout
- Saline ± steroid irrigation
- Stent if stricture
|
↓
74.9% symptom-free
25.1% may recur
|
↓
Recurrence? ──Yes──→ Repeat sialendoscopy
|
No
↓
Follow-up to puberty
(spontaneous resolution expected)
E. SJÖGREN SYNDROME
Sjögren syndrome (SS) is an autoimmune exocrinopathy causing chronic salivary and lacrimal gland inflammation. Ductal involvement leads to strictures, mucus plugging, and glandular atrophy.
Per Cummings: "Patients with recurrent sialadenitis may benefit from sialendoscopy to dilate and wash out the affected ducts. A multidisciplinary approach that involves the salivary endoscopist, who can offer interval procedures, and the rheumatologist can help optimize treatment."
Sialendoscopic findings in SS:
- Whitish ductal walls
- Multiple strictures
- Reduced duct caliber
- Mucus plugs
- Loss of vascular markings
Treatment protocol:
- Serial balloon dilation of strictures
- Saline + steroid lavage (triamcinolone)
- May require repeated sessions (every 6-12 months)
- Combined rheumatological management: hydroxychloroquine, pilocarpine
Note: Success rate in SS is lower than sialolithiasis; symptomatic improvement rather than cure is the aim. Sialendoscopy cannot reliably differentiate SS from JRP (Soriano-Martin 2023).
F. RADIOIODINE-INDUCED SIALADENITIS (RAIS)
Radioactive iodine (RAI/I-131) used for thyroid cancer treatment causes sialadenitis in 18-26% of patients, with subjective symptoms in up to 60% and abnormal scintigraphy in 69%. The parotid is more severely affected due to its predominantly serous nature and higher concentration capacity for iodide. Bilateral parotid involvement is most common.
Mechanism: I-131 concentrates in salivary acinar cells (via NIS - sodium-iodide symporter), causing direct cytotoxicity, ductal inflammation, strictures, mucus plugging, and fibrosis.
Per Cummings: "Sialendoscopy is a relatively novel approach in the treatment of radioiodine-induced sialadenitis... involves gland washouts, removal of debris and mucus plugs, and dilation of the papilla, ducts, or strictures with or without stent placement; this treatment seems to provide symptomatic benefit and reduced frequency and intensity."
Success rate for RAIS: 45.8% (lowest among all indications - Beumer et al., 2024 meta-analysis). Lower success reflects irreversible glandular damage from radiation.
Sialendoscopy protocol for RAIS:
- Papilla dilation
- Washout of mucus plugs and debris
- Balloon dilation of strictures
- Steroid instillation (triamcinolone)
- Stent placement
Prevention: Some authors recommend prophylactic sialendoscopy or sialagogue use during/after RAI therapy to reduce RAIS incidence.
G. SIALODOCHITIS / MUCUS PLUGS / FIBRIN PLUGS
Sialodochitis (ductal inflammation) may produce fibrin plugs, mucus casts, or debris that obstruct the duct without a calculus. These are ideally managed with:
- Endoscopic retrieval using basket or forceps
- Saline lavage under irrigation pressure
- Steroid instillation
IX. COMBINED (HYBRID) APPROACH
When sialendoscopy alone is insufficient - typically for large, impacted, or intraglandular stones - a combined approach is used:
Sialendoscopy alone fails or stone >8mm
|
↓
Combined / Hybrid Approach
|
┌──────────┴──────────┐
↓ ↓
Submandibular Parotid gland
(Transoral approach) (External approach)
| |
↓ ↓
Sialendoscope Sialendoscope
localizes stone localizes stone
| |
↓ ↓
Transoral incision Partial or complete
over Wharton duct parotidectomy incision
+ stone removal with SMAS flap elevation
| |
↓ ↓
Stent placement Stent placement
2-4 weeks 2-4 weeks
Per Cummings: "The combined approach involves visualization and localization of the stone by endoscopy or ultrasound and removal of the stone by making an incision into the duct."
For parotid stones, a partial parotidectomy incision and elevation of the superficial musculoaponeurotic system (SMAS) flap may be required. Post-procedure stenting is especially important in the parotid given its high stricture tendency.
X. PEDIATRIC SIALENDOSCOPY
Special considerations in children:
- General anesthesia in almost all cases below age 8
- Smaller scope sizes required (0.8-1.1 mm preferred)
- JRP is the dominant indication (68.9% - Cummings)
- Sialolithiasis is rarer in children but success rate is high: 95.5% effectiveness, 97.2% safety (Skalias et al., Eur Arch Otorhinolaryngol 2023, PMID 36781439; meta-analysis of 13 studies, 133 pediatric sialolithiasis cases)
- The 1.6 mm scope may be too large for very young patients - 0.8 mm diagnostic scope used first
- JRP resolves spontaneously at puberty in virtually all cases
XI. OUTCOMES AND SUCCESS RATES
The most comprehensive evidence comes from Beumer et al. (2024) - PMID 37486613:
- Systematic review + meta-analysis
- 91 studies, 8218 patients, 9043 procedures
- Weighted pooled success rate: 80.9%
- No major complications reported
- Sialadenectomy rate: 0-14%
| Indication/Gland | Success Rate |
|---|---|
| Sialolithiasis (overall) | 89.6% |
| Submandibular gland | 88.3% |
| Parotid gland | 81.2% |
| Endoscopic-assisted transoral (stone) | 86.3% |
| Combined parotid approach | 78.2% |
| Ductal stenoses | 56.3% |
| Juvenile Recurrent Parotitis | 67.0% |
| Radioiodine-Induced Sialadenitis | 45.8% |
XII. COMPLICATIONS
Sialendoscopy has an excellent safety profile. No major complications were reported in the Beumer 2024 meta-analysis.
| Complication | Frequency | Management |
|---|---|---|
| Ductal perforation | Most common | Usually self-limiting; rarely needs repair |
| Temporary swelling | Common | Resolves in 24-48h |
| Post-op infection | Rare | Antibiotics |
| Papilla trauma/scarring | Rare | Careful dilation technique; stenting |
| Ductal avulsion | Very rare | Surgical repair |
| Stone migration proximally | Occasional | Repeat sialendoscopy |
| Failure to cannulate | 5-10% | Abandon; try alternative approach |
Per Cummings pediatric section: "The most common complication was ductal perforation."
XIII. FLOWCHART: OVERALL SIALENDOSCOPY PATHWAY
PATIENT WITH SALIVARY GLAND SYMPTOMS
(Recurrent swelling, pain, xerostomia)
|
↓
CLINICAL ASSESSMENT
History + Physical Examination
|
↓
IMAGING
┌──────────┼──────────┐
↓ ↓ ↓
USG HRCT MR Sialography
(1st line) (stone (complex cases,
sizing) strictures)
|
↓
DIAGNOSIS CONFIRMED?
| |
Yes No
| ↓
| Diagnostic Sialendoscopy
| |
| ↓
└──────→ PATHOLOGY IDENTIFIED
|
┌──────────┼──────────┬──────────┐
↓ ↓ ↓ ↓
Sialolithiasis Stricture Chronic JRP / SS /
(stenosis) inflam. RAIS
| | | |
↓ ↓ ↓ ↓
Wire basket Balloon Lavage + Lavage +
± Laser dilation + Steroid Steroid ±
lithotripsy Stent instill. Stent
| | | |
↓ ↓ ↓ ↓
Stone >8mm? Severe? Refractory? Recurrence?
| | | |
Yes Yes Yes Yes
↓ ↓ ↓ ↓
Combined Repeat Gland Repeat
approach sessions excision sialendo.
|
↓
GLAND PRESERVED + SYMPTOM RESOLUTION
(Overall success ~80.9%)
XIV. ROLE OF STEROID USE IN SIALENDOSCOPY
Recent systematic review (Teng et al., Clin Otolaryngol, 2026; PMID 41501981) specifically evaluated steroid use during sialendoscopy. Intraductal steroid instillation (triamcinolone, hydrocortisone, dexamethasone) is widely practiced to:
- Reduce post-procedural ductal edema
- Prevent re-stricture
- Reduce recurrence in inflammatory conditions (JRP, SS, RAIS)
- Provide anti-inflammatory effect on ductal mucosa
The Donaldson systematic review (Ann Otol Rhinol Laryngol, 2022; PMID 34493105) highlighted the need for properly designed studies on post-sialendoscopy oral corticosteroids.
XV. RECENT ADVANCES (2021-2026)
-
Robot-assisted sialolithotomy: Seif-Elnasr et al. (Laryngoscope 2024; PMID 38041581) compared intraoral microscopic vs. robot-assisted approach - robotic technique showed improved precision for submandibular stones.
-
Image-guided sialendoscopy: Gaffuri et al. (J Laryngol Otol 2024; PMID 37807900) described image-guided and sialendoscopy-assisted transoral approach for parotid duct stenosis and megaduct - improved accuracy for complex anatomy.
-
Pneumatic intraductal lithotripsy: Emerging as an alternative to holmium laser for stone fragmentation - lower cost, effective for medium stones, used through working channel.
-
Salivary Gland Society (MSGS) Questionnaire: International consensus tool (Buchholzer et al., Laryngoscope 2022; PMID 34236085) for standardizing patient-reported outcomes in sialendoscopy - enables multicenter outcome comparison.
-
Eosinophilic sialodochitis: Recently characterized entity (Sanchez Barrueco et al., Clin Rev Allergy Immunol, 2026; PMID 42032355) - sialendoscopy shows characteristic findings (fibrinous plugs, eosinophilic infiltration) and plays a therapeutic role.
-
Ultrasound-guided combined approach: Pre-operative ultrasound marking of stone location for combined approach planning - improves precision of external incision.
-
Virtual sialendoscopy: CT/MRI 3D reconstruction allowing pre-procedural ductal mapping in complex cases before actual sialendoscopy (Cummings, Ch. 83).
-
Biodegradable stents: Under investigation for prevention of re-stenosis after balloon dilation - avoid second procedure for stent removal.
XVI. CONTRAINDICATIONS AND LIMITATIONS
Absolute contraindications:
- Acute suppurative sialadenitis (perforation risk; bacteremia risk)
- Trismus (cannot access papilla)
Limitations:
- Expensive, specialized equipment
- Long learning curve
- Cannot access intraglandular parenchymal disease
- Limited utility in complete ductal obliteration
- Low success in severe RAIS (irreversible glandular damage)
- Not curative for Sjögren syndrome (only symptomatic relief)
- Requires general anesthesia in children
- Sporadic adoption due to cost in low/middle-income countries
XVII. COMPARISON WITH TRADITIONAL APPROACHES
| Aspect | Sialendoscopy | Gland Excision |
|---|---|---|
| Invasiveness | Minimally invasive | Major surgery |
| Gland preservation | Yes | No |
| Nerve risk | Nil | Facial / lingual / hypoglossal |
| Scar | None | External |
| Anesthesia | GA or LA | GA |
| Recovery | Day-care | 2-5 days hospital |
| Success | 80-90% | 100% (stone removed with gland) |
| Dry mouth | No | Yes (permanent loss of gland) |
| Cost | High (equipment) | Moderate-high |
XVIII. SUMMARY TABLE - ROLE BY DISEASE
| Disease | Sialendoscopy Modality | Key Action | Success |
|---|---|---|---|
| Sialolithiasis | Interventional | Wire basket ± laser | 89.6% |
| Ductal stricture | Interventional | Balloon dilation + stent | 56.3% |
| Chronic sialadenitis | Interventional | Lavage + steroid | Good |
| JRP | Interventional | Washout + steroid | 74.9% |
| Sjögren syndrome | Interventional | Dilation + lavage | Palliative |
| RAIS | Interventional | Washout + dilation | 45.8% |
| Mucus plugs | Interventional | Basket + lavage | High |
| Unexplained swelling | Diagnostic | Visualization | Diagnostic |
XIX. REFERENCES
- Cummings CW, Flint PW, et al. Cummings Otolaryngology Head and Neck Surgery, 7th ed. Elsevier, 2021. Chapters 83, 205.
- Scott-Brown WG. Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th ed. CRC Press, 2019. Vol. 2, Ch. 45.
- Lee KJ. KJ Lee's Essential Otolaryngology, 11th ed. McGraw-Hill, 2022. Ch. Sialadenitis/Sialolithiasis.
- Beumer LJ, Vissink A, Gareb B, et al. "Success rate of sialendoscopy. A systematic review and meta-analysis." Oral Dis. 2024 May. [PMID: 37486613] - 91 studies, 8218 patients; pooled success 80.9%.
- Soriano-Martin D, Garcia-Consuegra L, Junquera L, et al. "Sialendoscopy approach in treating juvenile recurrent parotitis: a systematic review." J Otolaryngol Head Neck Surg. 2023 Aug. [PMID: 37598195] - 74.9% success in JRP.
- Skalias A, Garefis K, Markou K, et al. "Effectiveness and safety of sialendoscopy for sialolithiasis in children." Eur Arch Otorhinolaryngol. 2023 Jul. [PMID: 36781439] - 95.5% effectiveness in pediatric sialolithiasis.
- Teng TZJ, Low JYD, Razali AH. "Steroid Use in Sialendoscopy - A Systematic Review." Clin Otolaryngol. 2026 May. [PMID: 41501981].
- Donaldson G, de Paiva Leite S, Hardcastle T. "The Need for Studies on Oral Corticosteroids After Sialendoscopy." Ann Otol Rhinol Laryngol. 2022 Jul. [PMID: 34493105].
- Seif-Elnasr M, Magdy EA, Fung E. "Intraoral Microscopic vs Robot-Assisted Sialolithotomy." Laryngoscope. 2024 May. [PMID: 38041581].
- Gaffuri M, Battilocchi L, Pignataro L. "Image-guided and sialendoscopy-assisted transoral approach for parotid duct stenosis." J Laryngol Otol. 2024 May. [PMID: 37807900].
- Dhingra PL, Dhingra S. Diseases of Ear Nose and Throat, 8th ed. Elsevier; Salivary Gland Diseases chapter.
- Hazarika P. Textbook of ENT and Head & Neck Surgery. Jaypee Brothers; Salivary Glands.
Key Exam Points for RGUHS:
- Sialendoscopy introduced in 1990s; uses semirigid scopes of 0.8-1.6 mm diameter
- Principle: Gland-preserving, minimally invasive, transoral approach
- Most common indication overall: Sialolithiasis; in children: JRP (68.9%)
- Contraindicated in acute suppurative sialadenitis
- Overall success rate: 80.9% (Beumer meta-analysis 2024)
- Best results: sialolithiasis (89.6%); worst: RAIS (45.8%)
- Steroid instillation (triamcinolone 40 mg in 3-5 mL NS) at end of procedure is standard
- Stent for 2-4 weeks post-dilation to prevent re-stricture
- Combined/hybrid approach for stones >8 mm or impacted stones
- JRP: resolves spontaneously at puberty; sialendoscopy provides 74.9% recurrence prevention
This is a shared conversation. Sign in to Orris to start your own chat.