Pseudomonas eradication therapy in bronchiectasis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Pseudomonas aeruginosa" AND "bronchiectasis" AND "eradication"
Reading File
Reading Article
PMID: 38296344
Reading Article
PMID: 41016738
Finding Sources
Loading Image
Finding Sources
Loading Image
Reading File
Finding Sources
I now have very rich content. Let me compile the comprehensive answer.
Pseudomonas aeruginosa Eradication Therapy in Bronchiectasis
Why Eradication Matters
P. aeruginosa is the most commonly isolated pathogen in bronchiectasis and is independently associated with worse outcomes: higher mortality, increased hospitalization risk, accelerated lung function decline, and poorer quality of life. When first/new isolation is identified, eradication is recommended - the goal being to clear the organism before it establishes chronic mucoid colonization, which is far harder to treat.
When to Attempt Eradication
Eradication is indicated on first or new isolation of P. aeruginosa from sputum. A repeat sputum culture should first confirm persistent isolation (rather than transient/contaminant detection) before committing to a full course. Once mucoid conversion occurs or chronic infection is established, true eradication becomes unlikely - though suppression strategies continue.
Three Eradication Pathways
The ERS guidelines (as depicted in Murray & Nadel's) describe three parallel pathway options, each with a total treatment duration of 3 months:
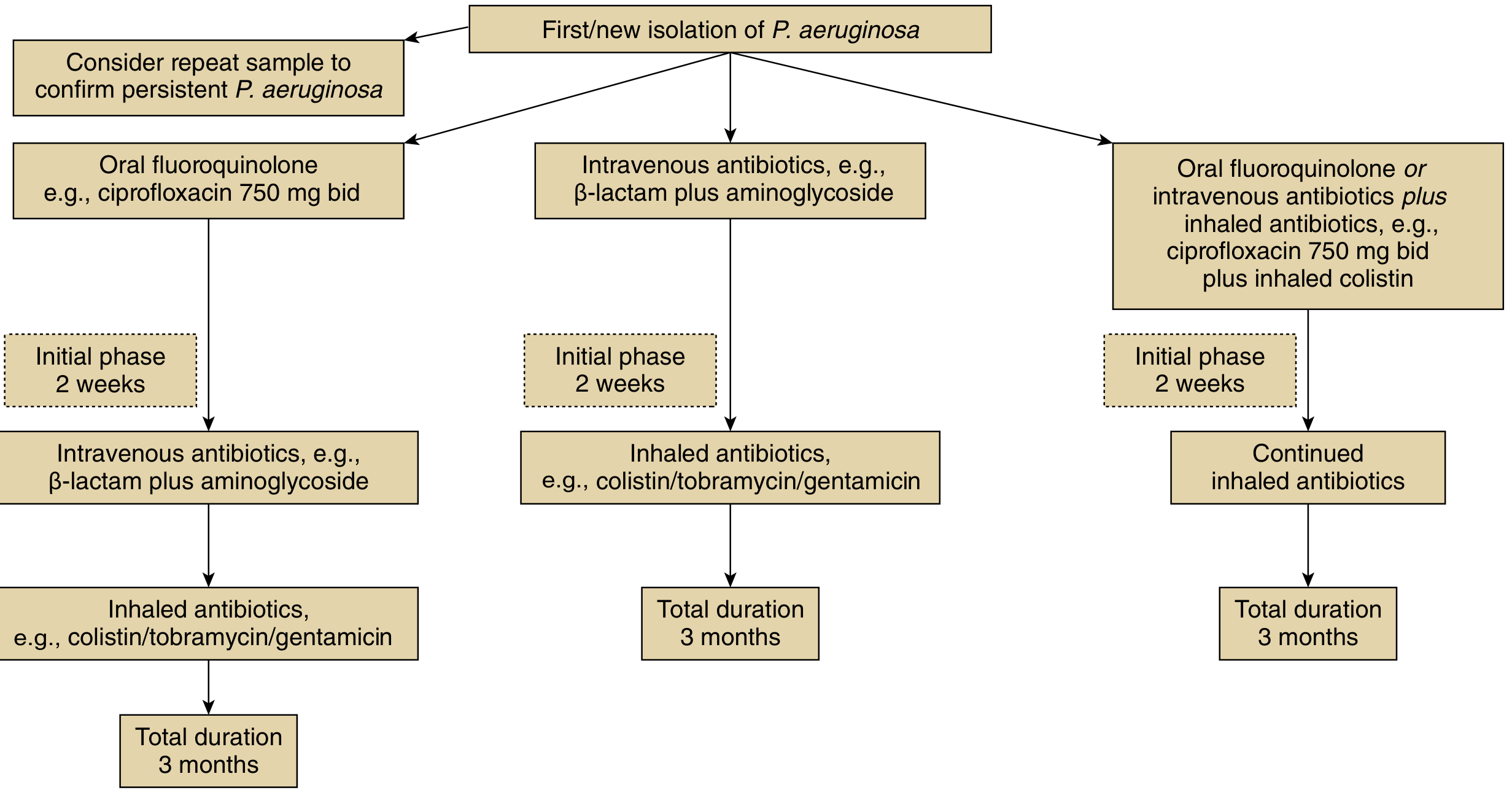
| Pathway | Initial phase (2 weeks) | Continuation |
|---|---|---|
| Pathway 1 | Oral fluoroquinolone (ciprofloxacin 750 mg BD) | IV antibiotics (beta-lactam + aminoglycoside), then inhaled antibiotics (colistin/tobramycin/gentamicin) |
| Pathway 2 | IV antibiotics (beta-lactam + aminoglycoside) | Inhaled antibiotics (colistin/tobramycin/gentamicin) - total 3 months |
| Pathway 3 | Oral fluoroquinolone OR IV antibiotics plus inhaled antibiotics (e.g., ciprofloxacin 750 mg BD + inhaled colistin) | Continued inhaled antibiotics - total 3 months |
After each step, sputum culture should be repeated. If P. aeruginosa persists, escalate to the next pathway.
Key Antibiotic Options
Oral (Systemic)
- Ciprofloxacin 750 mg BD - the preferred fluoroquinolone due to P. aeruginosa activity and oral bioavailability. Usually 2-4 weeks for the initial phase.
Intravenous
- Beta-lactam + aminoglycoside combination (e.g., ceftazidime, piperacillin-tazobactam, meropenem + gentamicin or tobramycin). Used for more severe presentations or when oral therapy has failed.
Inhaled
Used as continuation/maintenance after systemic therapy:
- Colistin (nebulized)
- Tobramycin (nebulized or dry powder - TOBI Podhaler)
- Gentamicin (nebulized) - RCT showed 31% P. aeruginosa eradication, reduced exacerbation frequency, improved QoL scores (LCQ, SGRQ), with no emergence of gentamicin resistance
- Ciprofloxacin - liposomal and dry powder inhaler formulations studied in phase 3 trials (ORBIT, RESPIRE programs)
- Aztreonam - inhaled solution studied but phase 3 trials did not demonstrate clinical benefit
Evidence Base and Success Rates
The 2024 systematic review and meta-analysis by Conceição et al. (Eur Respir Rev, PMID: 38296344) - the most rigorous analysis to date - found:
- Overall 12-month eradication rate: ~40% (95% CI 34-45%) across 6 observational studies, 289 patients
- Combined systemic + inhaled antibiotics: 48% eradication (95% CI 41-55%)
- Systemic antibiotics alone: 27% (95% CI 13-45%)
- No significant heterogeneity (I² = 0%)
This confirms that adding inhaled antibiotics to systemic therapy meaningfully improves outcomes, though even with optimal treatment, eradication fails in ~50-60% of patients.
After Failed Eradication: Long-Term Suppression
When eradication fails and chronic P. aeruginosa infection is established (or in patients with ≥3 exacerbations/year), the strategy shifts to long-term suppression:
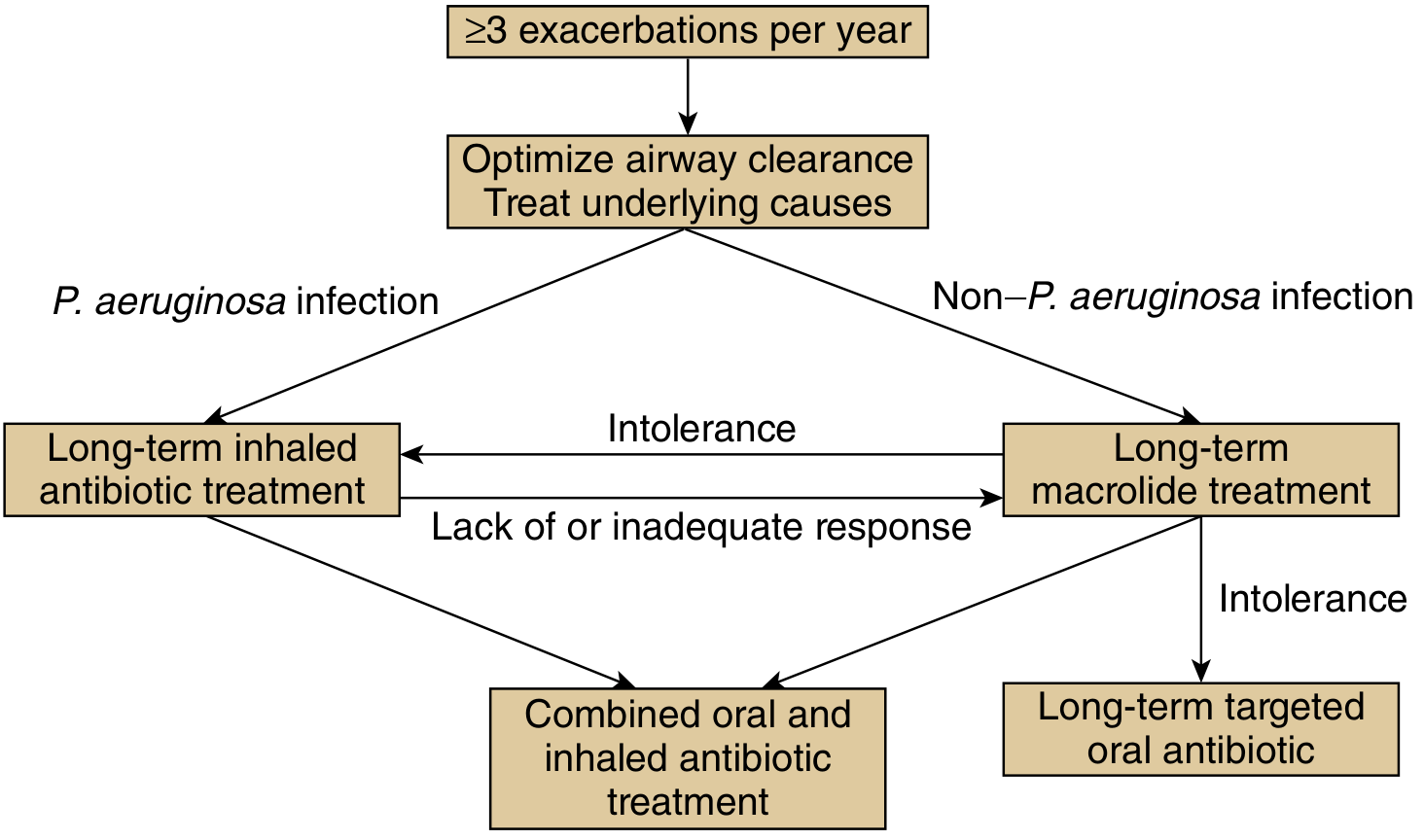
- P. aeruginosa infection → Long-term inhaled antibiotics (first line). If inadequate response: add oral antibiotics.
- Non-P. aeruginosa → Long-term macrolide (azithromycin), with a strong ERS 2025 recommendation for macrolides in high-exacerbation patients.
- Macrolide intolerance in P. aeruginosa patients → Long-term targeted oral antibiotic.
2025 ERS Guideline Updates
The updated ERS clinical practice guideline (Chalmers et al., Eur Respir J 2025, PMID: 41016738) made:
- Conditional recommendation in favor of eradication treatment in specific circumstances (acknowledging the limited RCT evidence base)
- Strong recommendation for long-term inhaled antibiotics in patients with chronic P. aeruginosa infection at high exacerbation risk
- Strong recommendation for macrolides in patients at high exacerbation risk
Practical Considerations
| Issue | Comment |
|---|---|
| Resistance monitoring | Repeat sensitivities at each exacerbation; P. aeruginosa multi-drug resistance is common |
| Bronchospasm with inhaled antibiotics | Pre-treat with bronchodilator; tobramycin and colistin can cause bronchospasm - monitor FEV1 after first dose |
| Combination antibiotic for exacerbations | Consensus supports combination (2 anti-pseudomonal agents) for severe exacerbations with P. aeruginosa; not needed for mild exacerbations |
| Duration | Minimum 14 days for exacerbations; 3 months total for eradication attempts |
| Mucoid conversion | New mucoid phenotype also warrants aggressive eradication attempt even in previously colonized patients |
| Renal monitoring | Required with aminoglycosides (IV); inhaled agents have much lower systemic absorption |
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders; Conceição et al., Eur Respir Rev 2024 (PMID 38296344); Chalmers et al. ERS Guideline, Eur Respir J 2025 (PMID 41016738)
This is a shared conversation. Sign in to Orris to start your own chat.