Senile cataract in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"senile cataract" OR "age-related cataract"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching Images
senile cataract types nuclear cortical subcapsular slit lamp
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive information to write a detailed answer. Let me compile everything:
Senile (Age-Related) Cataract
A senile cataract is an opacification of the crystalline lens occurring as a consequence of aging. It is the most common cause of reversible blindness worldwide and the leading indication for elective eye surgery.
Anatomy of the Lens
The crystalline lens is a biconvex, avascular, transparent structure suspended by the zonule of Zinn between the iris and vitreous. It consists of:
- Lens capsule — outermost, elastic basement membrane
- Lens epithelium — single layer of cells beneath the anterior capsule; the only mitotically active layer
- Lens cortex — newer, peripheral lens fibres (soft)
- Lens nucleus — older, central compacted lens fibres (harder with age)
New lens fibre cells are continuously laid down at the equator, compressing older fibres centrally. These central fibres cannot be shed, so the nucleus grows denser and less transparent over decades. By age 45, the lens loses pliability, impairing accommodation (presbyopia); later it loses transparency (cataract).
Pathogenesis
Several mechanisms converge to cause age-related lens opacification:
| Mechanism | Effect |
|---|---|
| Oxidative stress | UV-B and reactive oxygen species denature crystallin proteins, disrupting their ordered packing |
| Protein aggregation | Insoluble high-molecular-weight aggregates scatter light |
| Urochrome pigment deposition | Progressive yellowing → browning of the nucleus |
| Ion pump failure | Na⁺/K⁺-ATPase dysfunction → cortical hydration, vacuole and cleft formation |
| Epithelial cell migration | Abnormal posterior migration of equatorial epithelium → posterior subcapsular opacification |
| Sorbitol accumulation (in diabetes) | Aldose reductase converts glucose to sorbitol → osmotic swelling of lens fibres |
- Adams and Victor's Principles of Neurology, 12th Ed.: "lens proteins denature and degrade over time" as the fundamental mechanism.
- Robbins, Cotran & Kumar Pathologic Basis of Disease: accumulation of urochrome pigment renders the nucleus brown, distorting colour perception — the yellowish hues of Rembrandt's later paintings may reflect his nuclear sclerotic cataracts.
Risk Factors
Non-modifiable:
- Advancing age (most important)
- Female sex
- Genetic predisposition
Modifiable / Environmental:
- Ultraviolet-B radiation exposure
- Smoking
- Alcohol
- Dehydration and diarrhoeal episodes
- Poor nutrition (low antioxidant intake)
Systemic diseases:
- Diabetes mellitus (accelerates all types)
- Myotonic dystrophy
- Atopic dermatitis
- Neurofibromatosis type 2
- Wilson disease, galactosaemia
Drugs / Iatrogenic:
- Corticosteroids (systemic or topical) → posterior subcapsular cataract
- Phenothiazines
- Amiodarone
- Radiation (ionising and UV)
- Trauma
Classification by Morphology (Types of Senile Cataract)
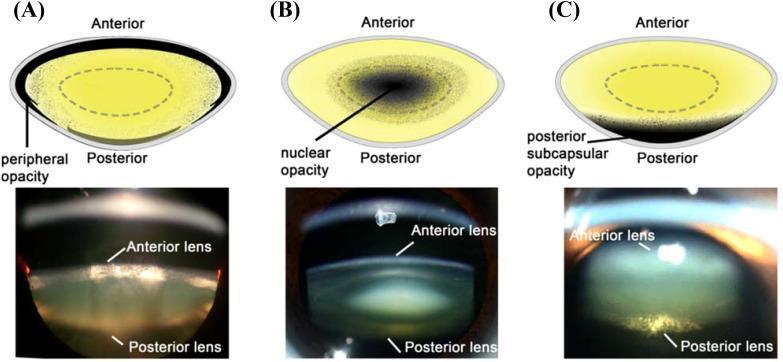
1. Posterior Subcapsular (PSC) Cataract
- Located just anterior to the posterior capsule
- Slit lamp: granular or plaque-like on oblique beam; black with vacuoles on retroillumination (Wedl/bladder cells = swollen migratory epithelial cells)
- Sits at the nodal point → disproportionate visual impact even when small
- Symptoms: glare (from oncoming headlights), worse with miosis (near vision, bright sunlight)
- Common with corticosteroids, diabetes, radiation, NF2
2. Nuclear Sclerotic Cataract
- Exaggeration of the normal ageing process — most common senile type
- Gradual yellowing (urochrome) → amber → brown (brunescent) → rarely black
- Best assessed with an oblique slit-lamp beam
- Retroillumination shows good red reflex with subtle nucleus–cortex distinction
- Associated with myopic shift ("second sight of the aged"): increased refractive index of the nucleus allows previously presbyopic patients to read again without spectacles
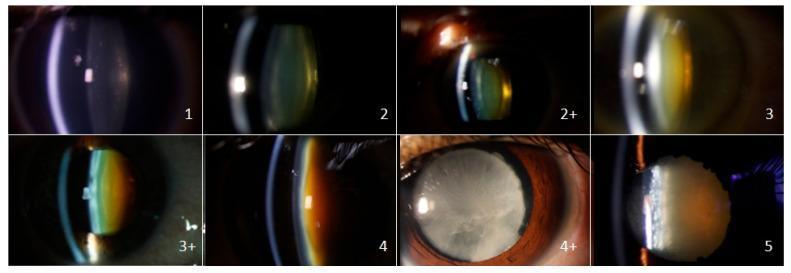
- Nuclear grading scale (SPONCS): Grade 1–5
3. Cortical Cataract
- Involves anterior, posterior, or equatorial cortex
- Begins as clefts and vacuoles due to cortical hydration → typical cuneiform (wedge-shaped) or radial spoke-like opacities, often starting infranasally
- Glare is prominent
- On slit-lamp: spoke-like opacities radiating from periphery toward centre
4. Anterior Subcapsular Cataract
- Lies directly under the anterior capsule
- Associated with fibrous metaplasia of the lens epithelium
- Seen with chronic anterior uveitis (posterior synechiae deprive epithelium of aqueous contact), atopic dermatitis (shield-like plaque)
5. Christmas Tree Cataract
- Uncommon; polychromatic needle-like formations in deep cortex and nucleus
- Associated with myotonic dystrophy
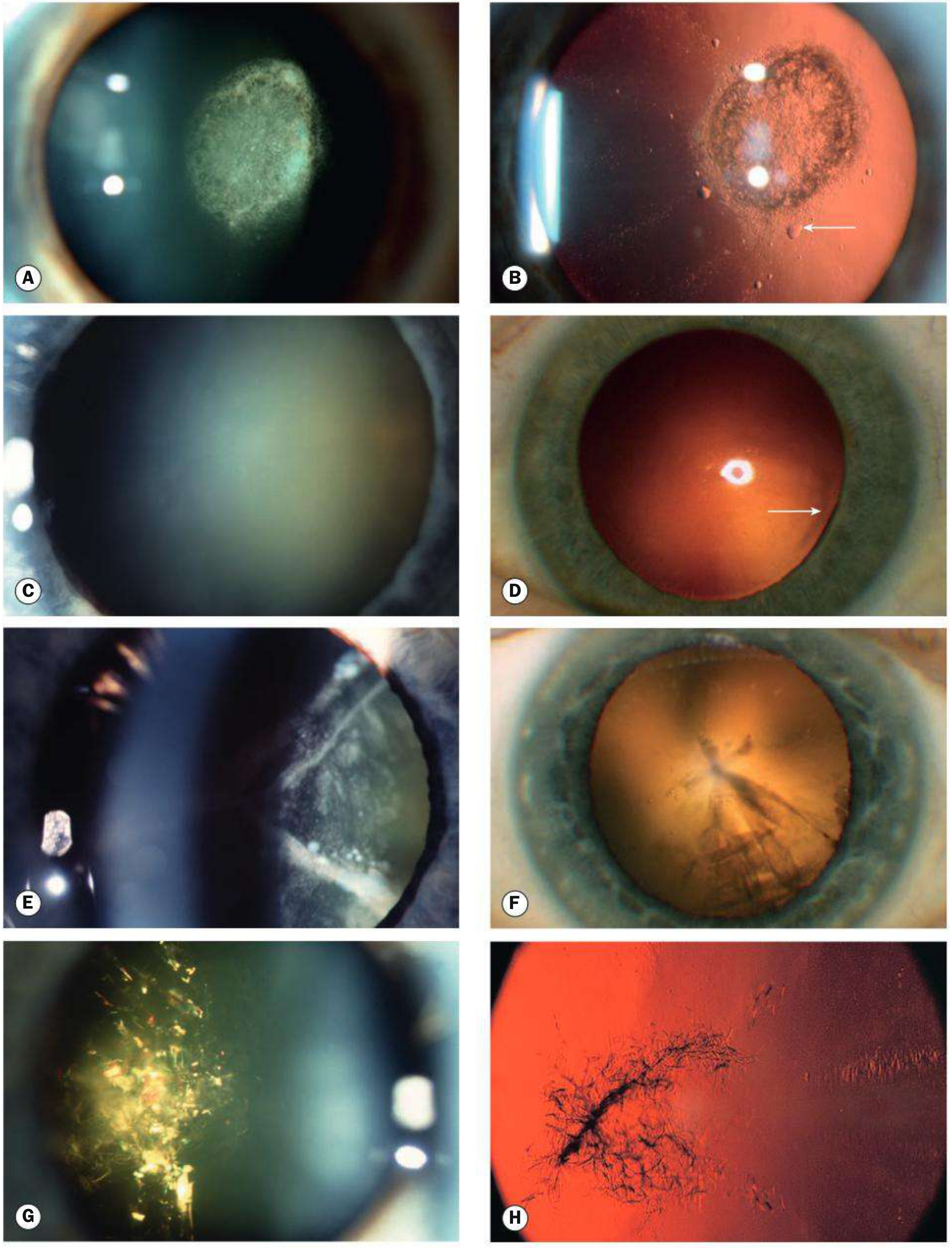
Fig. 10.2 — Kanski's Clinical Ophthalmology 10th ed.
Stages of Maturity
| Stage | Lens Appearance | Clinical Features |
|---|---|---|
| Immature | Partially opaque | Variable vision loss; red reflex present |
| Mature | Completely opaque; lens becomes milky white | No red reflex; significant vision loss |
| Hypermature | Shrunken, wrinkled anterior capsule | Water has leaked out; risk of phacolytic glaucoma |
| Morgagnian | Cortex liquefied; nucleus sinks inferiorly | Most advanced; dense white cortex with sunken brown nucleus |
Clinical Features
Symptoms:
- Gradual, painless, progressive visual blur
- Glare and halos (especially PSC and cortical)
- Monocular diplopia or polyopia (irregular refractive indices)
- Colour desaturation (nuclear cataract — blue-end of spectrum filtered)
- "Second sight" (myopic shift with nuclear cataract — temporary improvement in near vision)
- Difficulty with night driving
Signs on examination:
- Reduced visual acuity (Snellen chart)
- No afferent pupillary defect — its presence implies posterior pole pathology, not cataract alone
- Absent or diminished red reflex on direct ophthalmoscopy (mature/dense cataract)
- Slit-lamp biomicroscopy: definitive characterisation of type, density, location
Complications of Untreated Cataract
- Phacolytic glaucoma — mature/hypermature cataract leaks lens proteins through intact capsule → macrophages engulf them → block trabecular meshwork → open-angle glaucoma
- Phacomorphic glaucoma — intumescent (swollen) lens pushes iris forward → acute angle closure
- Phacoanaphylactic uveitis — lens protein leakage → autoimmune granulomatous uveitis
- Amblyopia — in unilateral dense cataract, especially in children
Management
Indications for Surgery
- Visual: Opacity sufficient to interfere with daily activities (most common)
- Medical: Phacolytic/phacomorphic glaucoma, media opacity preventing fundus monitoring/treatment
- Elective refractive: Clear lens exchange for refractive error correction
Preoperative Assessment
- Biometry (keratometry + axial length) → IOL power calculation
- Optical coherence biometry (partial coherence interferometry) is the preferred method
- A-scan ultrasonography as alternative
- Multiple formulae used (SRK-T, Hoffer Q, Haigis, Barrett Universal II)
- Check for alpha-blocker use (tamsulosin) → risk of intraoperative floppy iris syndrome (IFIS)
- Pupillary dilation adequacy; corneal endothelial cell count; macular OCT if suspect macular disease
- Manage anticoagulants per local protocol
Surgical Technique
Phacoemulsification (Standard)
- Small self-sealing corneal incision (~2.4–2.8 mm)
- Viscoelastic injection into anterior chamber
- Continuous curvilinear capsulorhexis (CCC) — circular tear of anterior capsule
- Hydrodissection — fluid wave separates nucleus from cortex
- Phacoemulsification — ultrasonic probe emulsifies and aspirates the nucleus
- Irrigation/aspiration of residual cortex
- Intraocular lens (IOL) insertion into the capsular bag
- Wound closure (usually self-sealing, no sutures)
Goldman-Cecil Medicine: "Standard phacoemulsification provides results as good as femtosecond laser treatment."
Extracapsular Cataract Extraction (ECCE)
- Larger incision; nucleus expressed intact; less used now
- Still preferred in very hard (brunescent) nuclei or when phaco is unavailable
Intracapsular Cataract Extraction (ICCE)
- Entire lens including capsule removed; rarely performed today
Intraocular Lenses (IOL)
- Monofocal (most common) — corrects for one distance; glasses needed for others
- Multifocal — corrects near and distance; risk of glare/halos
- Extended depth of focus (EDOF) — intermediate and distance
- Toric — corrects pre-existing astigmatism
- Target refraction: usually emmetropia or slight myopia
Complications of Cataract Surgery
| Category | Complication | Notes |
|---|---|---|
| Common / mild | Posterior capsular opacification (PCO) | Most common late complication; treated with Nd:YAG laser capsulotomy |
| IOP spike, iridocyclitis, ecchymosis | Usually transient | |
| Moderate | Posterior capsular rupture + vitreous loss | ~1% experienced surgeons |
| Cystoid macular oedema (CMO) | ~1–2%; treated with NSAIDs/steroids | |
| Retinal detachment | <1% | |
| Unexpected refractive outcome | May need IOL exchange or corneal surgery | |
| Zonular dehiscence, dropped nucleus (~0.2%) | Requires vitreoretinal surgery | |
| Rare / serious | Endophthalmitis (~0.1%) | Sight-threatening infection; treated with intravitreal antibiotics |
| Suprachoroidal haemorrhage (~0.04%) | Potentially devastating | |
| Overall risk | Loss of sight | ~1 in 1,000 operations |
Posterior Capsular Opacification (PCO)
- Most common late complication — occurs in up to 20–40% within 5 years
- Residual lens epithelial cells migrate onto the posterior capsule → "Elschnig pearls" or fibrous opacity
- Treatment: Nd:YAG laser posterior capsulotomy (outpatient, definitive)
Special Situations
Cataract in Diabetes
- Glucose → sorbitol (aldose reductase) → osmotic hydration → cortical vacuoles → opacities
- Classic diabetic (snowflake) cataract: white cortical flakes in young patients; may resolve with glucose control
- Age-related cataract occurs sooner in diabetics; nuclear sclerosis progresses rapidly
- Pre-existing diabetic macular oedema worsens post-surgery — monitor carefully
Morgagnian Cataract
A hypermature cataract in which the cortex has completely liquefied; the hard brown nucleus sinks to the bottom of the capsular bag under gravity. Surgical challenge: no red reflex, difficult capsulorhexis due to high intracapsular pressure.
Differential Diagnosis of Lens Opacity
| Condition | Key Distinguishing Feature |
|---|---|
| Congenital cataract | Present at birth or early childhood; requires urgent surgery to prevent amblyopia |
| Traumatic cataract | History of injury; "rosette" pattern |
| Corticosteroid-induced | PSC pattern; corticosteroid history |
| Diabetic (snowflake) | Young patient; white cortical flakes |
| Radiation cataract | PSC; radiation history |
| Wilson disease | "Sunflower" cataract (green/brown central opacity) |
Prognosis
The prognosis for restoration of vision is excellent when the retina is healthy. Cataracts typically develop asymmetrically; the worse eye is operated on first. Visual recovery is immediate — most patients achieve 6/6 to 6/12 vision within days. The second eye is operated on as the cataract becomes visually significant.
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed.; Goldman-Cecil Medicine, International Ed.; Robbins, Cotran & Kumar Pathologic Basis of Disease; Adams and Victor's Principles of Neurology, 12th ed.
This is a shared conversation. Sign in to Orris to start your own chat.