
My mom's age is 45yrs She had an episode of audible sounds in ears for few seconds Mind numb for few minutes After that mild weakness in left arm and left side of face she had this problem since 9months she's on lerrace and gabica but I'm confused there's no any true fit like fit include urinary incontinence tongue problem or fit like condition but I'm confused above mentioned condition is what panic attack or fit according to this MRI report?
Fahr disease seizure clinical manifestations
Fahr disease seizures focal epilepsy
Fahr disease seizures focal epilepsy symptoms clinical features 2024
https://pmc.ncbi.nlm.nih.gov/articles/PMC11621208
What the MRI Report Says - Plain Language Explanation
MRI Key Findings (What They Mean)
1. Bilateral Symmetrical Calcifications - Basal Ganglia + Cerebellum
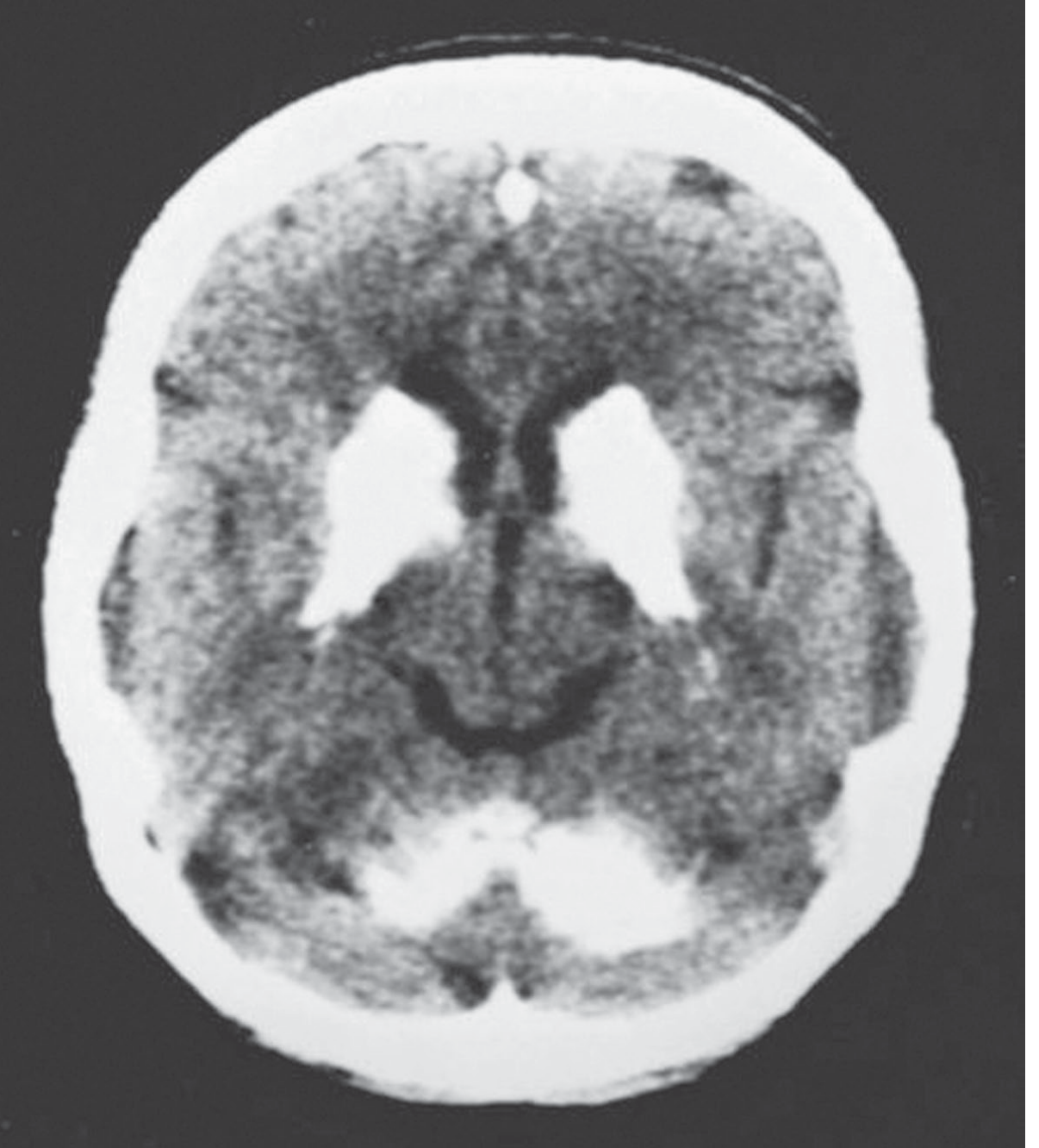
2. Chronic Microvascular Ischaemic Changes (Periventricular White Matter)
3. Widened Sulci / CSF Spaces
4. No Acute Infarction / No Hemorrhage
Is This a Fit (Seizure) or a Panic Attack?
Why it is NOT a Panic Attack
- Auditory auras (ringing/sounds in ears)
- Transient numbness of the mind
- Unilateral limb weakness (left arm)
- Unilateral facial weakness (left side of face)
Why it IS Most Likely a Focal Seizure (Specifically a Focal Aware Seizure + Todd's Paralysis)
| Phase | What Happened | Medical Term |
|---|---|---|
| Aura | Audible sounds in ears for seconds | Focal auditory/sensory aura |
| Ictal phase | Mind "numb" for a few minutes | Focal impaired awareness seizure |
| Postictal phase | Mild weakness in left arm and left face | Todd's (postictal) paralysis |
Why She Doesn't Have the "Classic" Fit Appearance
- Tongue biting
- Urinary incontinence
- Generalized shaking
The Role of Fahr's Disease
What About the Medications She's On?
- Lerrace = Levetiracetam (brand name) - this is an antiepileptic drug, confirming her treating neurologist already suspects or diagnosed seizures
- Gabica = Gabapentin - used for seizures and neuropathic pain
What Still Needs to Be Done (Pending Workup)
- Serum calcium, phosphorus, parathyroid hormone (PTH) - to rule out hypoparathyroidism (the most common secondary cause of basal ganglia calcification; if PTH is low or absent, that is the cause)
- Serum alkaline phosphatase, magnesium
- Genetic testing for SLC20A2 or PDGFRB mutations (responsible for familial Fahr's)
- EEG (electroencephalogram) - to characterize the seizure type and confirm epilepsy
- Brain CT scan if not done - CT is actually superior to MRI for quantifying calcifications
Summary in Simple Terms
Your mother is most likely having focal aware seizures (a type of epilepsy) caused or triggered by Fahr's disease (a condition where calcium deposits form in the basal ganglia and cerebellum of the brain). These seizures do not look like the "classic" convulsion with shaking and tongue-biting - instead they cause an auditory sensation, brief confusion, and then temporary weakness of the left side (called Todd's paralysis). There is no acute stroke on this MRI. She needs blood tests to investigate the underlying cause of the calcification (especially parathyroid hormone) and an EEG to map her seizure activity. Her current medications (levetiracetam and gabapentin) are the right class of drugs for this.
Disclaimer: This is educational information only and is not a substitute for in-person medical evaluation. Please consult her treating neurologist for clinical decisions.
Serum calcium, phosphorus, PTH, ALP , Magnesium , CT done Tomorrow I'll go for EEG of my mom
Before the EEG - What to Do Tonight & Tomorrow
What Happens During the EEG
- Small electrodes are placed on the scalp with a gel - completely painless, no needles
- She will be asked to open and close her eyes, breathe deeply and fast (hyperventilation) for a few minutes, and look at a flashing light - these are activation techniques to provoke any abnormal activity
- The test takes about 30-45 minutes
- If she has an episode during it, that is actually very useful diagnostic information
When You Get the Results - Share Them Here
- The EEG report
- The blood results (calcium, phosphorus, PTH, ALP, magnesium)
- The CT report (if you have it)
- Whether the calcification is primary (Fahr's disease) or secondary (e.g., hypoparathyroidism - which is treatable)
- What type of seizure pattern is on the EEG
- Whether the current medications need adjustment
Calcium, phosphorus, PTH, ALP, magnesium are all normal CT scan shows same result as it is on MRI But EEG is not done yet
What Normal Labs + CT Calcification Means
| Test | Normal = Rules Out |
|---|---|
| PTH normal | Hypoparathyroidism, pseudohypoparathyroidism |
| Calcium normal | Hypercalcemia-related calcification |
| Phosphorus normal | Metabolic phosphate disorders |
| ALP normal | Metabolic bone disease |
| Magnesium normal | Hypomagnesemia-related disorders |
What This Means Practically
1. The Seizures Are Explained
2. Her Current Medications Are Appropriate
- Lerrace (Levetiracetam) - a first-line antiepileptic, well suited for focal seizures
- Gabica (Gabapentin) - helps with neural excitability and possible associated pain/discomfort
3. There Is No Specific Cure for Fahr's Disease
- Antiepileptics for seizures (which she is already on)
- Monitoring for emerging movement disorders (parkinsonism, dystonia, ataxia) over time
- Neuropsychiatric monitoring (memory, mood, personality changes can develop gradually)
- Regular follow-up with a neurologist every 3-6 months
4. Family History Matters
- First-degree relatives (her children, siblings) may carry the same mutation
- Genetic counseling is advisable if she has children
- Screening with brain CT/MRI can be considered for symptomatic family members
The EEG Tomorrow Is Still Very Important
- It will classify the seizure type precisely - focal vs. generalized, which hemisphere, which lobe
- It guides medication dosing - if the EEG shows frequent interictal discharges, her current dose may need to go up
- It gives a baseline - future EEGs can be compared to it to track progression
- It may catch subclinical seizures she is not aware of
One Additional Test Worth Discussing With Her Neurologist
Share the EEG report when done for medication assessment
- What type and location of epileptic activity is present
- Whether her current doses of Lerrace and Gabica are likely adequate for what the EEG shows
- Whether any additional medications may be needed
- What questions to ask her neurologist at the next visit
- Arrive on time - the technician needs to set up electrodes carefully, so rushing affects quality
- If she has an episode during or after the test - tell the technician immediately and do not leave until it is documented, as capturing an actual event on EEG is extremely valuable
- Ask for a printed copy of the report before you leave the hospital, or at least a digital copy - many centers only call with a verbal summary which is not enough detail
- Ask specifically whether the reporting neurologist reviewed it or only the EEG technician - the neurologist's interpretation is what matters
How above mentioned genetic testing for genes is done , is it done through blood test??
How Genetic Testing for Fahr's Disease Is Done
Sample Collection
- A regular venous blood draw (usually 3-5 ml in an EDTA tube - the purple/lavender cap tube)
- Same type of draw as a routine CBC
- No fasting required, no special preparation
- Takes 2 minutes at any lab
What the Lab Does With the Blood
| Gene | What It Does |
|---|---|
| SLC20A2 | Phosphate transporter - accounts for ~40-50% of familial cases |
| PDGFRB | Platelet-derived growth factor receptor - blood-brain barrier integrity |
| PDGFB | Ligand for PDGFRB |
| XPR1 | Phosphate exporter |
Practical Steps to Get It Done
Step 1 - Get a Referral
Step 2 - Find a Genetics Lab
- Shaukat Khanum Memorial Hospital, Lahore - has a molecular genetics department
- Aga Khan University Hospital, Karachi - offers molecular/genetic testing and may send abroad if not available locally
- INMOL / Liaquat National Hospital genetics departments
- Some samples are sent to labs in UAE, UK, or India for processing if not available locally - this is normal and acceptable
Step 3 - Turnaround Time
- Usually 3-6 weeks for NGS panel results
- Some international labs take up to 8 weeks
Step 4 - Interpreting the Result
- Pathogenic mutation found - confirms familial Fahr's, identifies specific gene, family members can be tested for the same mutation
- Variant of uncertain significance (VUS) - a change is found but its meaning is not yet clear, needs follow-up
- No mutation found - does not rule out Fahr's disease; about 50% of cases have no currently identified mutation (the disease may still be genetic but the causative gene not yet discovered)
Is It Necessary Right Now?
- Your family's planning - if you or your siblings want to know if they carry the same risk
- Future pregnancies in the family
- Academic completeness of the diagnosis
How much it cost like If I'm willing to done this from agha khan karachi
- Whether the test is done in-house or sent to an external/international lab
- Which specific gene panel is ordered (single gene vs. full PFBC panel)
- Whether a genetics specialist consultation is bundled in
How to Get the Exact Cost - Do This Tomorrow
Option 1 - Call AKUH Directly
- Main number: (021) 111-911-911
- Ask for the Pathology / Molecular Genetics department
- Say: "I need pricing for a genetic test for Primary Familial Brain Calcification / Fahr's disease - SLC20A2 and PFBC gene panel"