Rhinomanometry
rhinomanometry nasal airway resistance
Rhinomanometry
Definition
- R = resistance (Pa/cm³/s, or cmH₂O/L/s)
- ΔP = trans-nasal pressure (Pa or cmH₂O)
- V̇ = nasal airflow (cm³/s or L/s)
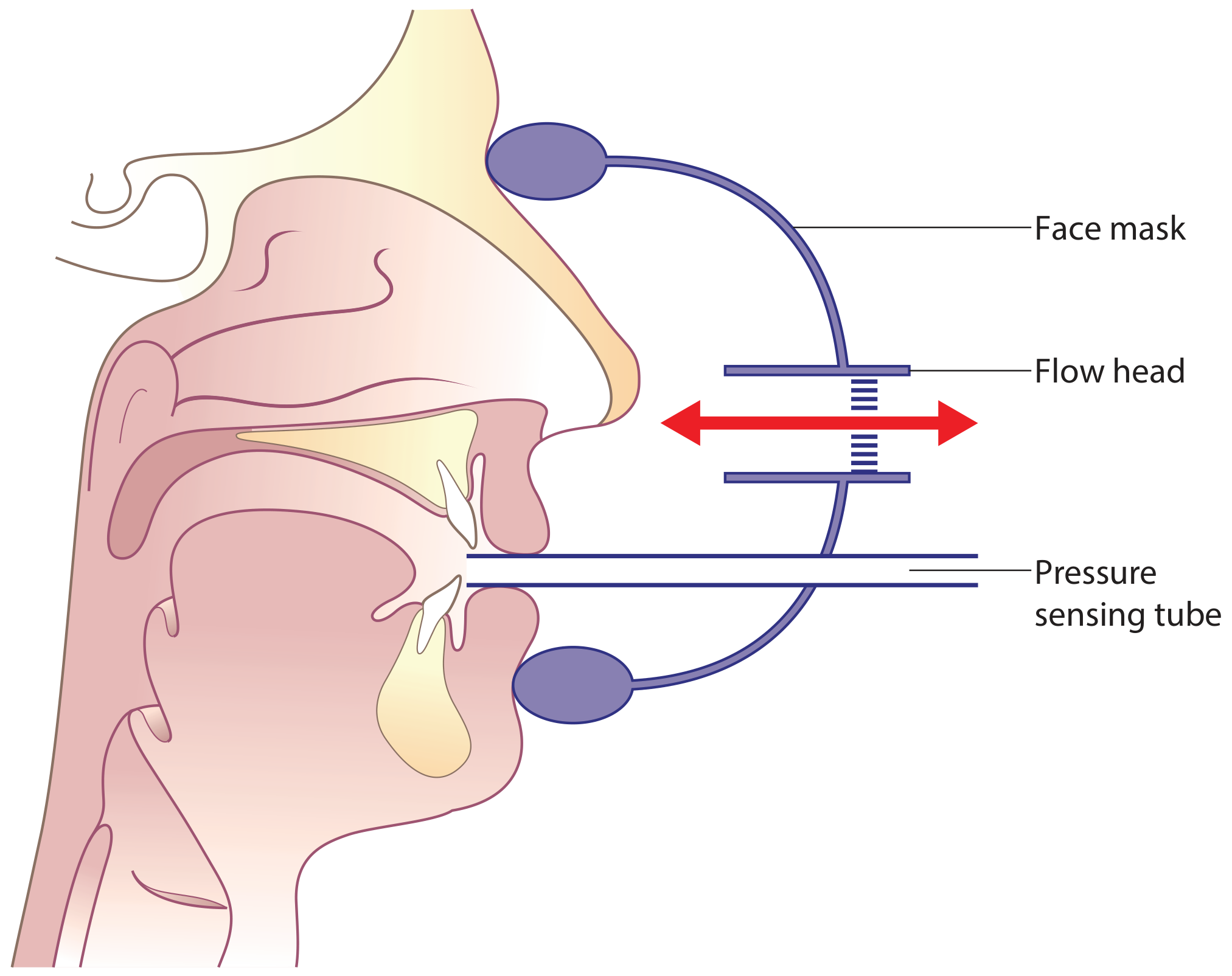
How It Works
- Nasal airflow - via a flow head (mesh resistance inside a tube); pressure difference across the mesh is proportional to airflow.
- Trans-nasal pressure - the pressure at the posterior nares relative to atmospheric pressure (or nasal mask pressure) at the nostril entrance.
Classification of Methods
| Feature | Type | Description |
|---|---|---|
| Airflow source | Active | Patient breathes normally |
| Passive | External fan/pump drives air through the nose | |
| Pressure sensor location | Anterior | Tube taped to one nostril; measures one side at a time |
| Posterior | Tube in the mouth; measures both nostrils simultaneously |
Active Anterior Rhinomanometry (AAR) - Most Common
- A face mask is applied over the nose.
- The pressure-sensing tube is taped into one nostril (occluding it), so the sealed passage acts as an extension of the tube to detect posterior nares pressure.
- Airflow is measured from the contralateral (open) nostril.
- The tube is then switched to measure the other side.
- Resistance is measured for each side separately, then combined to give total resistance.
- Cannot be used in nasal septal perforation (pressure equalization prevents measurement).
Active Posterior Rhinomanometry
- The pressure-sensing tube is placed in the mouth, detecting posterior nares pressure when the soft palate allows oral communication.
- Both nasal passages can be measured simultaneously.
- Advantage: total nasal airflow is measured directly.
- Disadvantage: not all subjects can maintain soft palate opening; successful in ~90% with training.
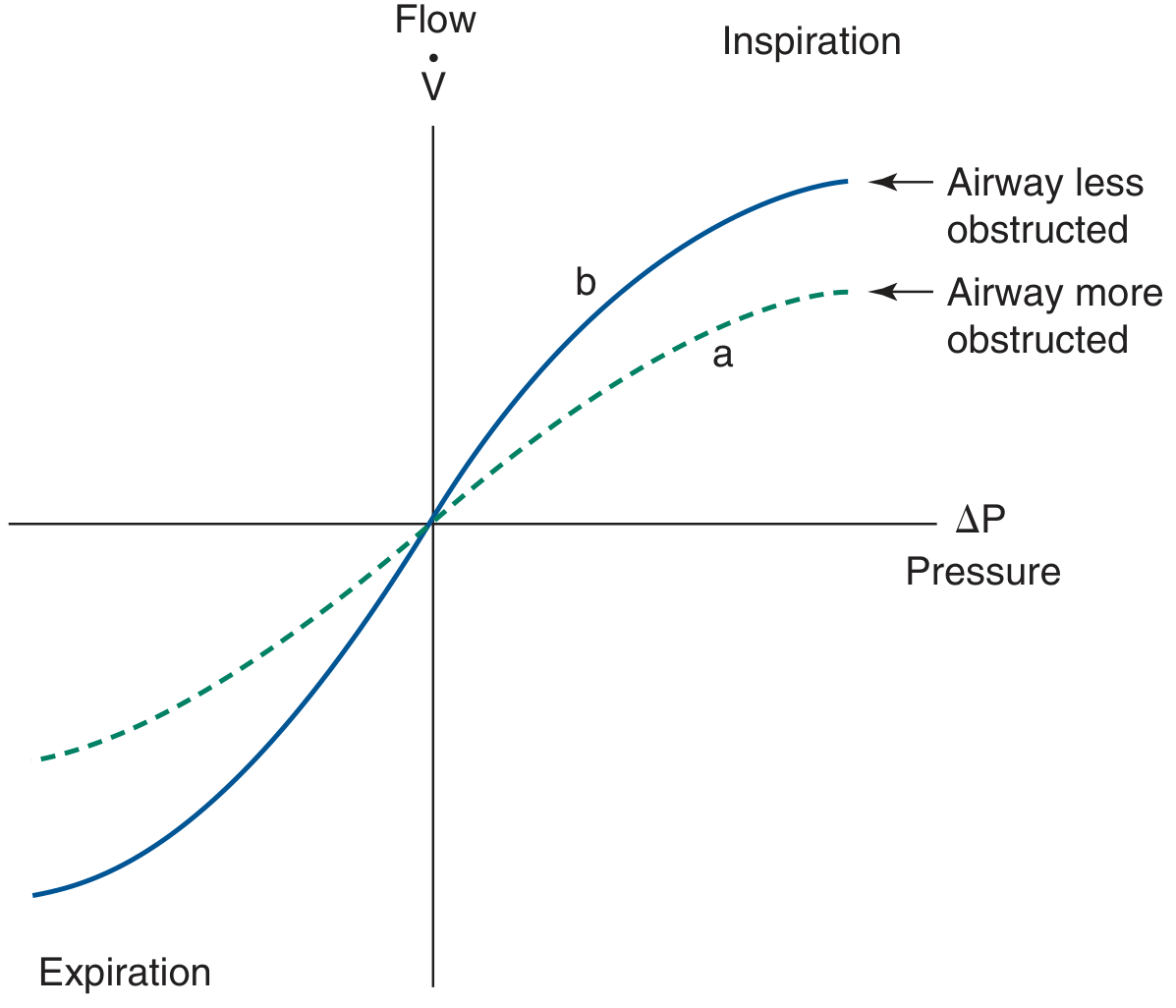
The Pressure-Flow Curve
- The curve has a sigmoid shape.
- A more obstructed airway produces a curve shifted closer to the pressure axis (lower flow for the same pressure).
- Flattening of the curve distally at a single flow rate may represent nasal valve collapse.
- During inspiration, the accelerating and decelerating limbs trace slightly different paths (hysteresis), which is the basis of 4-phase rhinomanometry.
Standardized Reporting Points
- Unilateral NAR: measured at 150 Pa (classic RM, anterior method)
- Bilateral NAR: measured at 75 Pa (posterior method)
- Units: Pa/cm³/s (0.1 Pa/cm³/s = 1 cmH₂O/L/s)
- Results from inspiration are most commonly reported in classic RM.
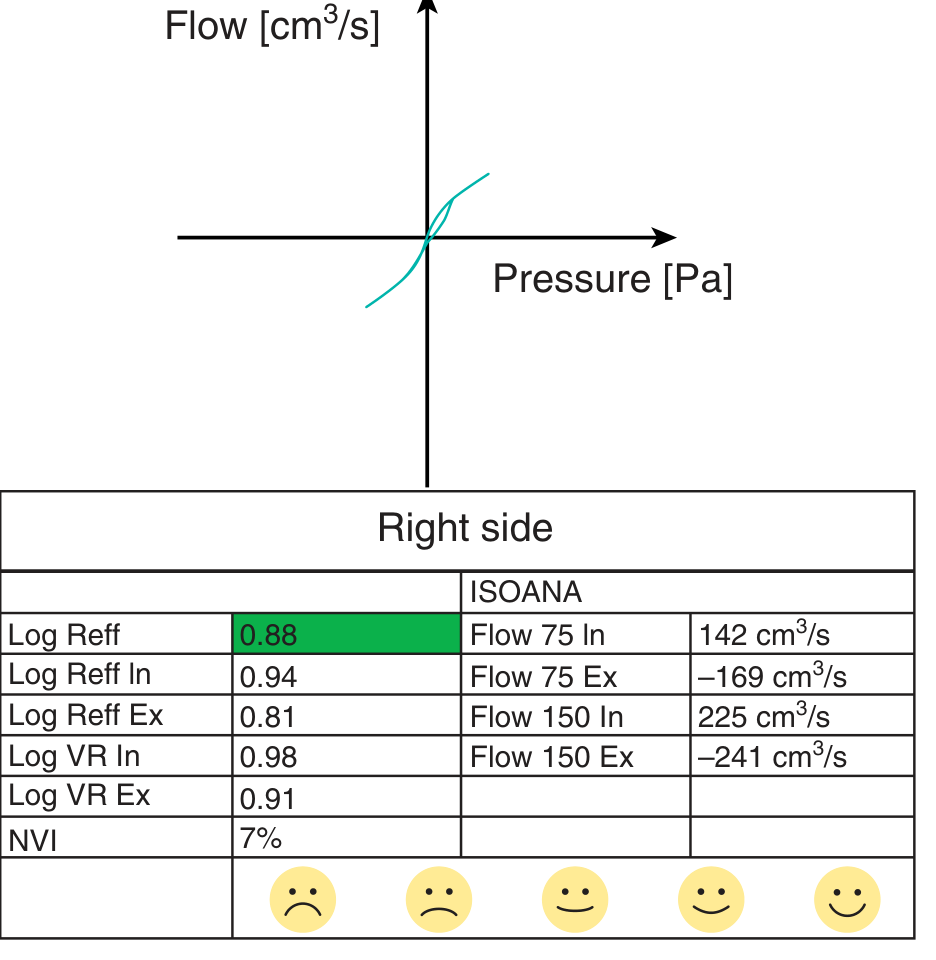
4-Phase Rhinomanometry (4PR)
- Vertex Resistance (VR) - resistance at the highest point of the flow curve during quiet breathing; best correlates with the subjective symptom of nasal obstruction.
- Effective Resistance (Reff) - resistance across the entire breathing cycle (area under the curve of hundreds of resistances).
- ReffIn / ReffEx - effective resistance during inspiration/expiration separately.
- Logarithmic values (LVR, LReff) are used for normal distribution.
Normal Values
| Population | Total NAR (congested) |
|---|---|
| Adults (mean) | ~0.23 Pa/cm³/s |
| Adults (normal range) | 0.15-0.39 Pa/cm³/s |
| Upper limit of normal (clinical screen) | 0.30 Pa/cm³/s |
| Obstructed (Cole's criterion) | >0.25 Pa/cm³/s |
| Infants | ~1.2 Pa/cm³/s |
| Children 5-12 yr (males) | ~0.6 Pa/cm³/s |
| Adolescents 13-19 yr | ~0.29 Pa/cm³/s |
| Adults >20 yr | ~0.22 Pa/cm³/s |
- NAR is higher in infants, declines to adult values at age 16-18 years.
- Females have lower resistance than males on average.
- Unilateral NAR is highly variable due to the nasal cycle (can vary 4-fold over 6-8 hours); total NAR is more stable due to reciprocal congestion/decongestion.
Technical Considerations
- Multiple measurements with mask repositioning between each are required - a single measurement is unreliable.
- The computerized simultaneous display of the pressure-flow curve allows detection of mask leaks during testing.
- Decongestion (exercise or topical decongestant) before measurement eliminates physiological variation from the nasal cycle and isolates anatomical factors - particularly useful when assessing nasal skeletal stenosis.
- RM can be performed in supine, right-side lying, and left-side lying positions to evaluate positional nasal obstruction.
- Can be performed in children as young as 2 years old using a smaller facemask.
- Reference values should ideally be established in each department, as population differences exist.
Clinical Applications
| Indication | Notes |
|---|---|
| Nasal obstruction assessment | Objective measurement before/after septoplasty, turbinate surgery |
| Allergic rhinitis | RM is useful for diagnosis; shown to be sensitive to mucosal changes |
| Nasal challenge testing | Documents response to allergen or pharmacological challenge |
| Decongestant response | Demonstrates physiological vs anatomical component of obstruction |
| Positional nasal obstruction | RM in different body positions |
| Preoperative/postoperative rhinological assessment | Objective outcome measure |
| Pediatric nasal airway assessment | From age 2 years |
Comparison with Peak Nasal Inspiratory Flow (PNIF)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1, Chapter 90 (p. 1039-1040)
- Cummings Otolaryngology Head and Neck Surgery, Chapter 37 (p. 767-768)
Benign tumors of parotid gland
parotid gland benign tumors
Benign Tumors of the Parotid Gland
Epidemiology - General Principles
- ~75% of all salivary gland neoplasms arise in the parotid gland.
- About 80% of parotid tumors are benign.
- A useful rule: the larger the salivary gland, the more likely a tumor is benign - malignancy rates are ~25% (parotid), ~50% (submandibular), and ~75% (sublingual/minor salivary glands).
- Deep lobe parotid tumors can present as apparent unilateral tonsillar hypertrophy or soft palate bulge due to parapharyngeal space extension.
WHO Classification of Benign Epithelial Salivary Gland Tumors
| Tumor |
|---|
| Pleomorphic adenoma |
| Myoepithelioma |
| Basal cell adenoma |
| Warthin's tumor |
| Oncocytoma |
| Lymphadenoma |
| Cystadenoma |
| Sialadenoma papilliferum |
| Ductal papillomas |
| Sebaceous adenoma |
| Canalicular adenoma |
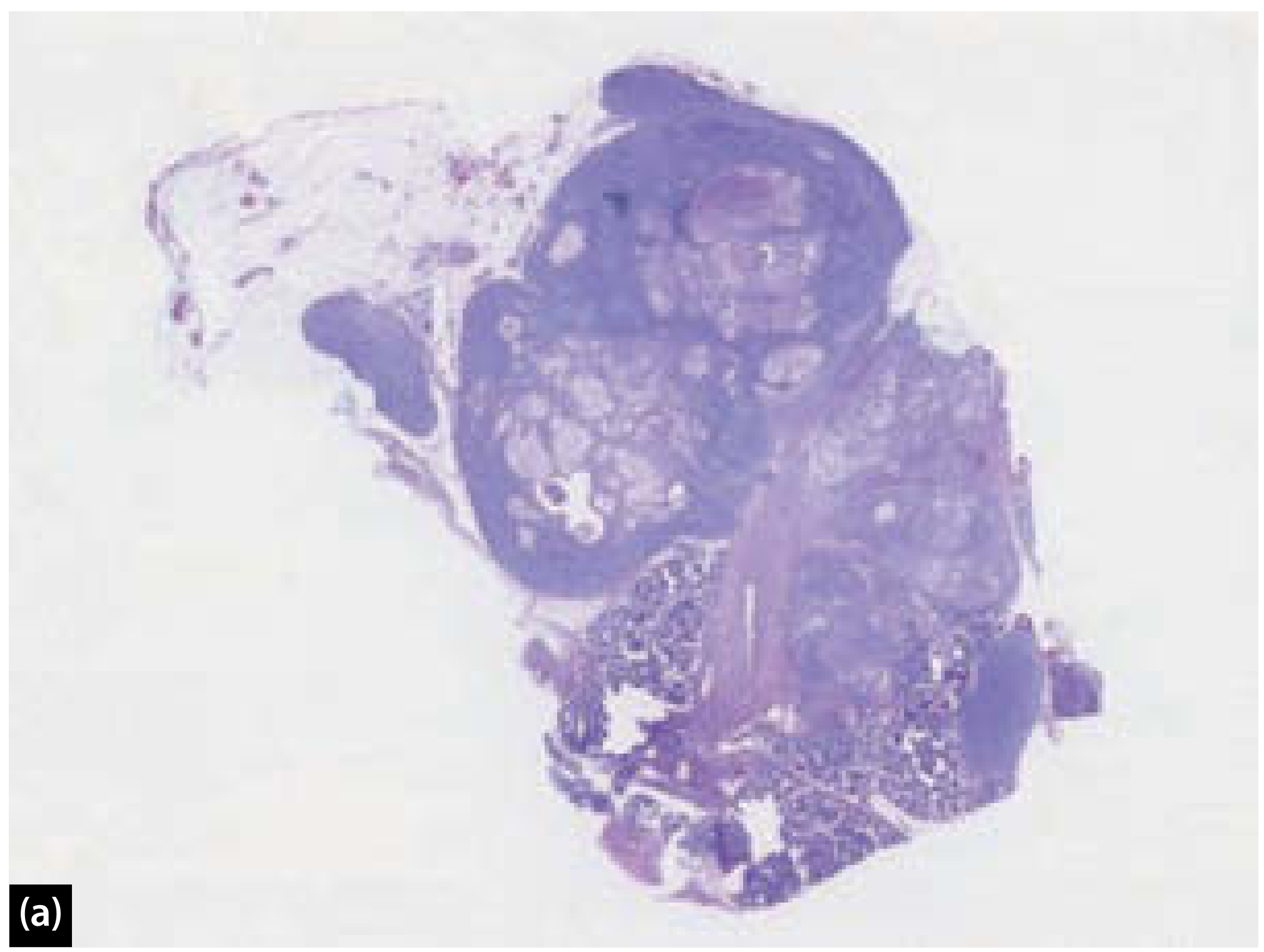
1. Pleomorphic Adenoma (Benign Mixed Tumor)
Overview
- Most common salivary gland tumor overall.
- Incidence: 2.4-3.05 per 100,000/year.
- Comprises ~50% of all salivary gland tumors, ~65% of parotid tumors, and ~40% of intra-oral minor salivary gland tumors.
Macroscopic Appearance
- Areas of cystic change and calcification
- Variably encapsulated - capsule may be thick/fibrotic or attenuated/incomplete
- Homogeneous or variegated cut surface depending on histological pattern
- Pericapsular nodules (sometimes attached by a slender pedicle) - enucleation risks detaching these, leaving a nidus for recurrence

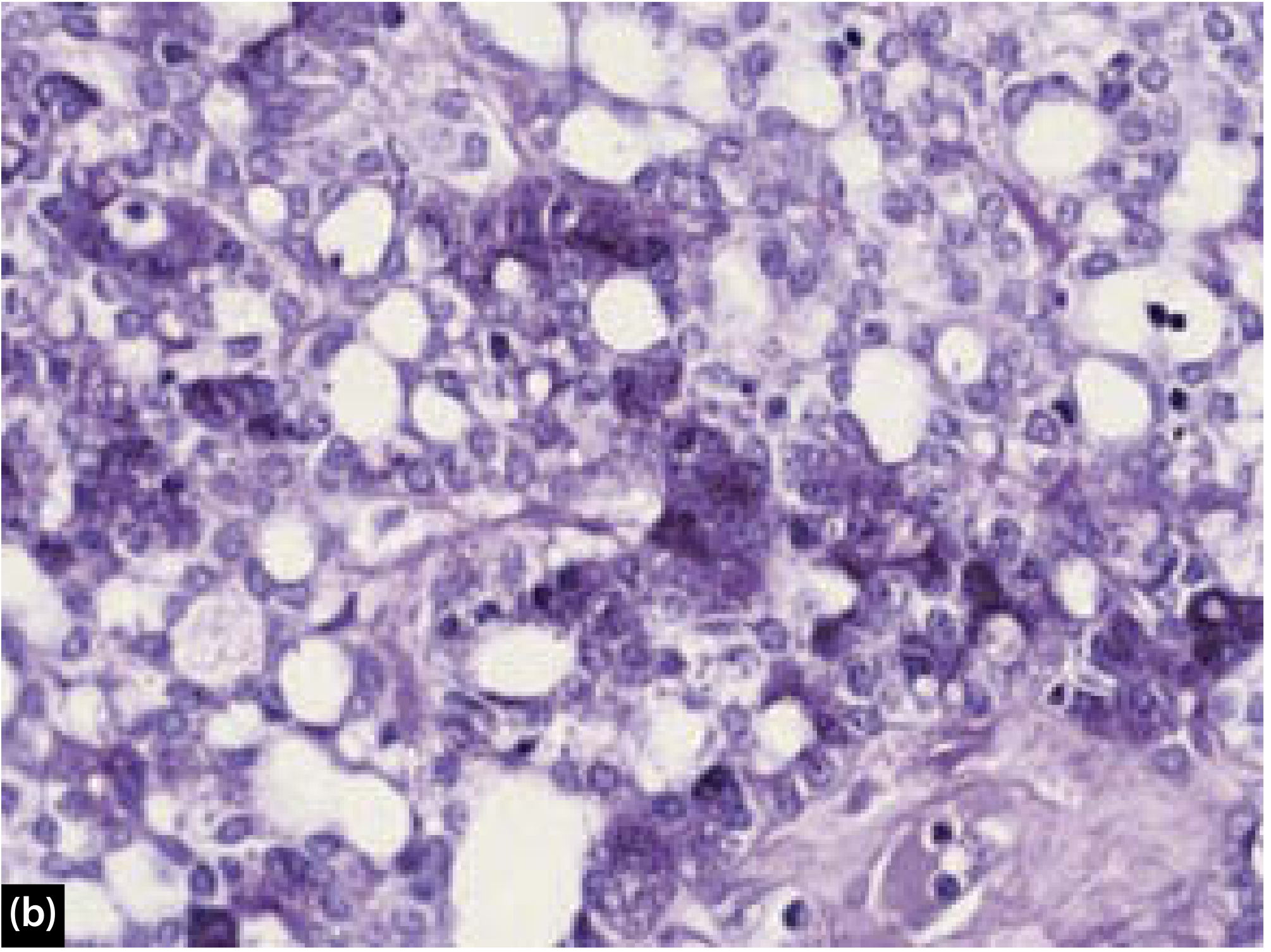
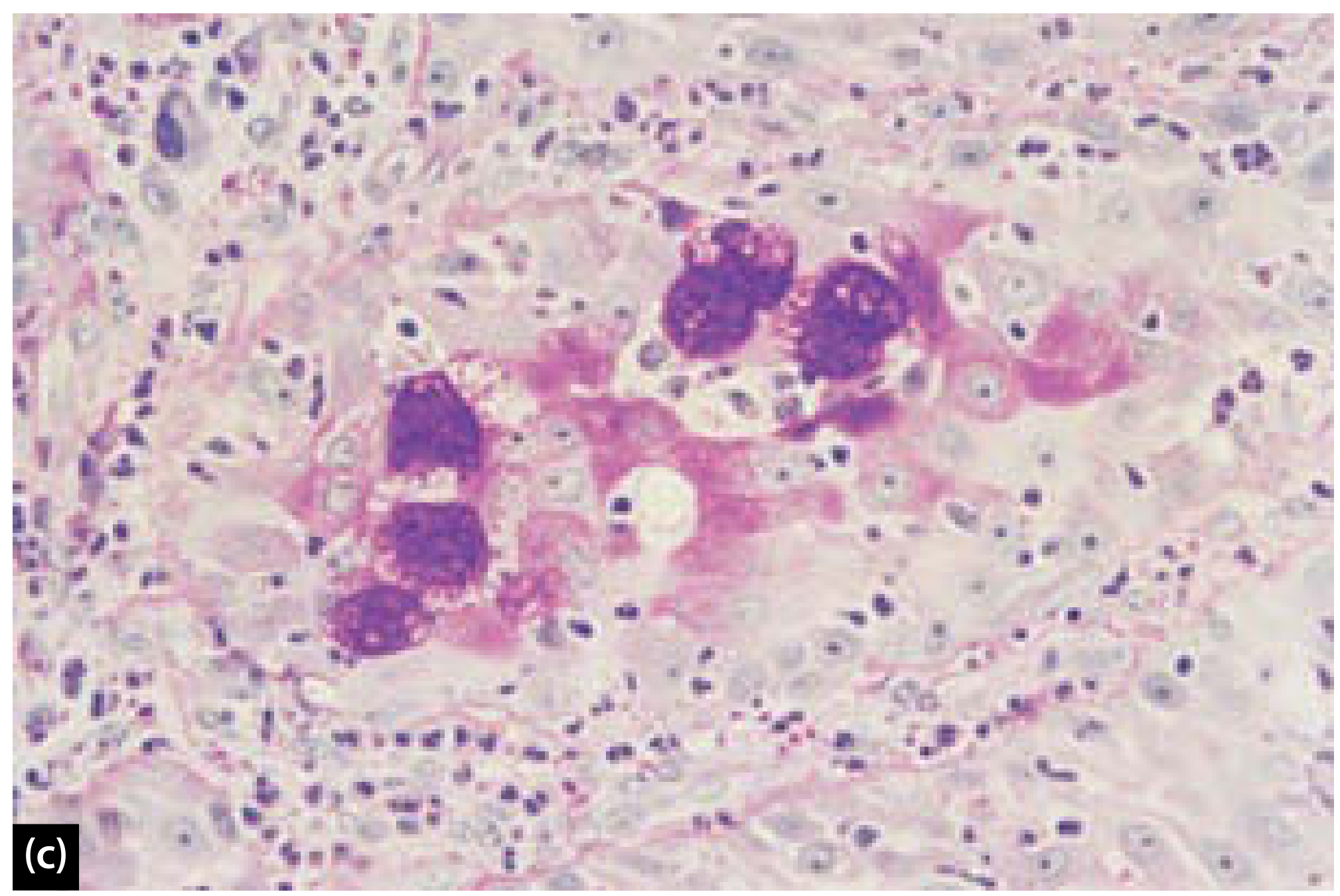
Microscopic Appearance
- Metaplastic: squamous, lipomatous, osseous, neuroid, angiomatoid
- Degenerative: cystic change, infarction, mineralization, hyalinization, elastosis
- Growth patterns: adenoid cystic-like, clear cell, epithelial-myoepithelial-like, basaloid, giant cell, spindle cell, plasmacytoid, oncocytoid
Risk of Malignant Transformation
- Older patient age
- Male sex
- Long duration of tumor
- Multiple recurrences
- Deep lobe parotid location
Treatment
- Parotidectomy with facial nerve preservation (superficial or total depending on tumor location).
- Enucleation alone is contraindicated - unacceptably high recurrence rate due to pericapsular nodules.
- Extracapsular dissection is an alternative technique (no facial nerve dissection) - only for select tumors in expert hands.
- Recurrence rate with facial nerve dissection procedures: 1%-4%; recurrences are typically multinodular.
- Definitive treatment for recurrence: resection of all gross tumor + postoperative radiation therapy.
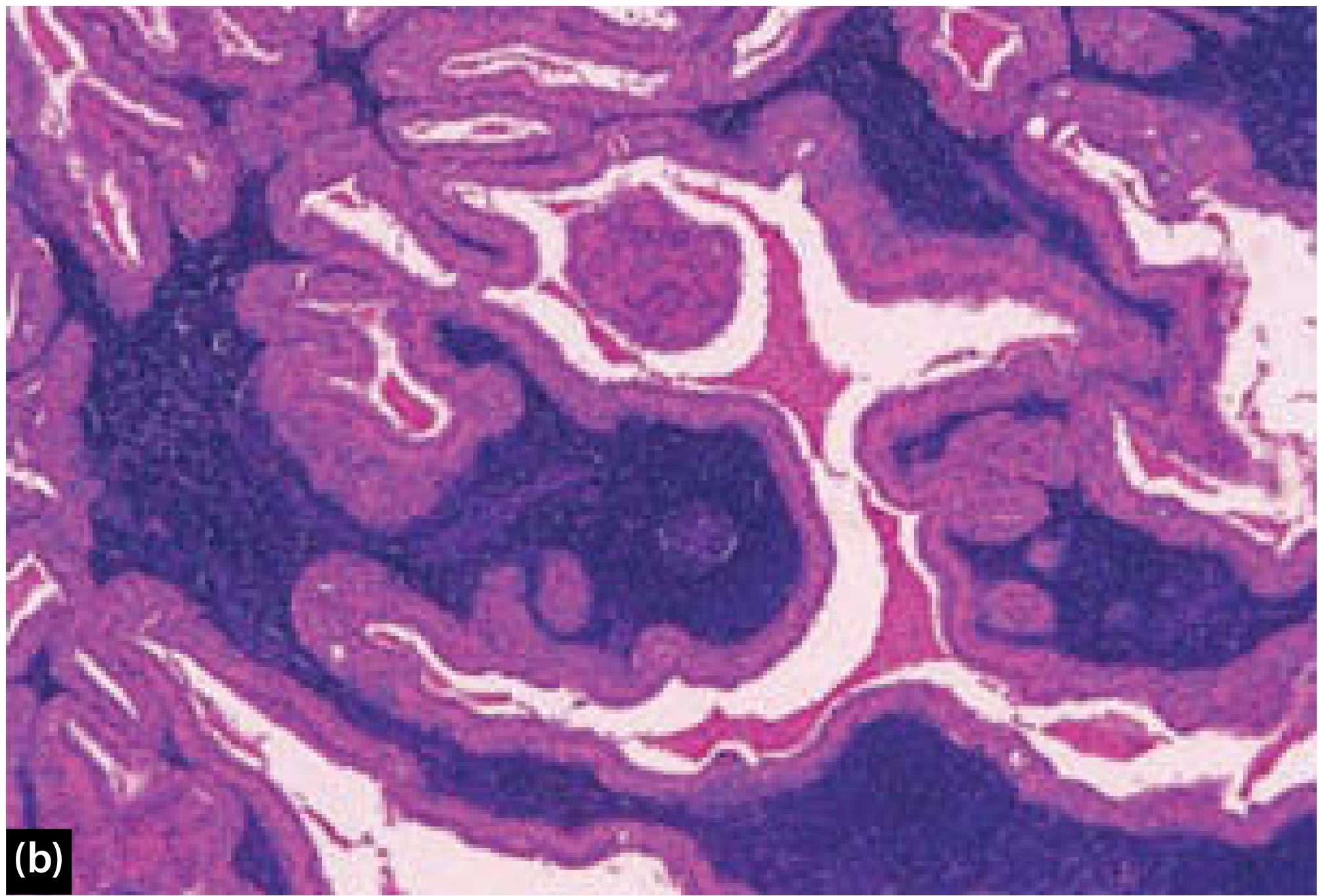
2. Warthin's Tumor (Adenolymphoma / Papillary Cystadenoma Lymphomatosum)
Overview
- Second most common benign parotid neoplasm; ~10% of all parotid tumors.
- Exclusive to the parotid gland and para-parotid lymph nodes.
- Multicentric and/or bilateral in 4-20% of cases.
- Comprises 3.5-30% of primary epithelial salivary gland tumors (geographic variation).
- More common in Caucasians and Asians; lower incidence in African-Americans and Black Africans.
- Occurs commonly in the sixth decade (women) and seventh decade (men).
- Strong association with cigarette smoking (most common in smokers >40 years).
- No clonal population by PCR - therefore not universally considered a true neoplasm.
Macroscopic Appearance

Microscopic Appearance
- Apical cells: tall columnar with dark small nuclei and granular pink (eosinophilic) cytoplasm
- Basal cells: cuboidal
- The granular eosinophilia of oncocytes = abundant mitochondria
- Cystic areas contain amorphous debris
Special Investigations
- Technetium-99m pertechnetate scintigraphy: hot spot (avid uptake due to oncocytic component) - useful for diagnosis.
- 18F-FDG PET: avid due to high mitochondrial content - can mimic metastasis on staging scans in cancer patients.
- The benign oncocytic epithelial inclusions commonly seen in intraparotid/para-parotid lymph nodes probably account for the tumor's multicentricity and bilaterality.
Malignant Transformation
- Rare - either carcinomatous or lymphomatous transformation.
- Considered to have very low malignant potential.
Treatment
- Surgical excision (parotidectomy with facial nerve preservation) for enlarging or symptomatic tumors.
- Observation is appropriate for:
- Non-enlarging or incidentally found tumors
- Patients with metastatic cancer (avoid false-positive PET interpretation)
- Patients with contraindications to surgery
- Bilateral tumors in heavy smokers
3. Oncocytoma (Oxyphilic Adenoma)
- <1% of all salivary gland tumors; most occur in the parotid gland.
- Oncocytes = large epithelial cells with granular eosinophilic cytoplasm due to mitochondrial hyperplasia (accumulation).
- Oncocytic metaplasia: transformation of acinar and ductal cells to oncocytes - associated with aging.
- Oncocytosis: proliferation of oncocytes throughout the salivary gland.
- Peak incidence: 5th-6th decade; gender distribution nearly equal.
- Associated with prior radiation exposure.
Histology
- Granular appearance due to abundant hyperplastic mitochondria.
- No lymphoid tissue (key distinction from Warthin's tumor).
- May show some atypia, squamous metaplasia, or necrosis - can mimic adenoid cystic carcinoma, mucoepidermoid carcinoma, adenocarcinoma; must be differentiated from metastatic thyroid or renal cell carcinoma.
Behavior
- Parotid oncocytomas: benign, slowly enlarging, painless, enhance on radionuclide scan.
- Minor salivary gland oncocytomas can be locally invasive, even involving cartilage or bone, despite histologically benign appearance.
- Rarely show true malignant features (increased mitoses, perineural or vascular invasion).
Treatment
4. Myoepithelioma
- ~1% of salivary gland neoplasms; most present in the parotid.
- Composed exclusively of myoepithelial cells (unlike PSA which has both ductal and myoepithelial elements).
- Can have spindle cell, plasmacytoid, epithelioid, or clear cell morphology.
- Generally behaves benignly; surgical excision is the treatment.
5. Basal Cell Adenoma
- 2%-5% of salivary gland tumors; about 5% occur in the parotid.
- Histologically shows nests and islands of basaloid cells with peripheral palisading.
- Can mimic the solid subtype of adenoid cystic carcinoma - careful histological distinction is needed.
- Membranous type (dermal analogue tumor) has the highest recurrence rate and a ~28% association with cylindromas of the skin.
6. Canalicular Adenoma
- Usually located in the upper lip (minor salivary glands), not commonly in the parotid.
- Slow-growing, asymptomatic.
- Characterized by bilayered columnar epithelial strands in a loose vascular stroma.
7. Benign Mesenchymal Tumors
Lipoma
- CT and MRI show characteristic fat-density/signal appearance.
- True parotid lipoma is uncommon.
Schwannoma (Neurilemmoma)
- Benign encapsulated tumor arising from Schwann cells of peripheral nerve sheath.
- In the parotid region, may arise from the facial nerve (cranial nerve VII) or its branches.
- The NF2 gene is inactivated in ~67% of schwannomas; ~2% are associated with neurofibromatosis type 2 (bilateral vestibular schwannomas + meningiomas - autosomal dominant).
- Treatment: surgical excision with nerve preservation when possible.
Differential Diagnosis of Parotid Mass
| Feature | Pleomorphic Adenoma | Warthin's Tumor | Mucoepidermoid Carcinoma |
|---|---|---|---|
| Frequency | 65% of parotid tumors | ~10% | Most common parotid malignancy |
| Age | Any | 6th-7th decade | Any |
| Bilaterality | Rare | Up to 20% | No |
| Smoking link | No | Yes (strong) | No |
| Surface | Bosselated | Smooth/cystic | Variable |
| Capsule | Variable | Thin, complete | Often absent |
| Tc-99m | Cold | Hot | Cold |
| Malignant potential | ~6% | Very low | Inherently malignant |
Investigations
| Test | Role |
|---|---|
| Ultrasound | First-line; assesses size, location, cystic vs solid |
| CT/MRI | Deep lobe tumors; parapharyngeal extension; bilateral parotid masses suggest Warthin's |
| FNA (FNAC) | Useful but ~80% sensitivity for benign vs malignant; cytologic accuracy varies |
| Tc-99m scintigraphy | Warm/hot = Warthin's or oncocytoma; cold = most other tumors |
| Intraoperative frozen section | Guides extent of surgery, avoids reoperation |
Treatment Summary
- All parotid tumors should generally be surgically removed regardless of benign diagnosis because:
- Confirms histopathology
- Prevents malignant transformation (especially PSA)
- Removal is technically easier before enlargement
- Reduces facial nerve morbidity
- Superficial parotidectomy with facial nerve identification and preservation: standard for superficial lobe tumors
- Total parotidectomy: required for deep lobe or multiquadrant tumors
- Facial nerve sacrifice is reserved for malignant disease with nerve invasion
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2, Chapter 26, p. 473-476
- Cummings Otolaryngology Head and Neck Surgery, Chapters 37 and 84, p. 767, 1512-1513
- KJ Lee's Essential Otolaryngology, Chapter on Benign Tumors and Cysts, p. 652
- Sabiston Textbook of Surgery, Chapter on Benign Neoplasms of the Salivary Glands, p. 1345
Superficial parotidectomy
superficial parotidectomy facial nerve
Superficial Parotidectomy
Definition and Principle
Indications
- Benign parotid tumors (pleomorphic adenoma, Warthin's tumor) in the superficial lobe
- Biopsy/excision for suspected malignancy (with intraoperative frozen section)
- Chronic parotitis not responding to conservative treatment
- As a component of total conservative parotidectomy for deep lobe tumors (superficial parotidectomy is performed first to expose the facial nerve)
- Access for parapharyngeal space tumors
Preoperative Preparation
- No neuromuscular paralysis (or short-acting agent only) - facial nerve monitoring requires the nerve to be electrically excitable throughout the procedure.
- Position: reverse Trendelenburg (head-up) to reduce venous congestion and bleeding.
- Facial nerve monitor electrodes placed in orbicularis oculi and orbicularis oris.
Incision

- 'Lazy S' incision (modified Blair incision): starts in the preauricular crease, curves around the lobule of the ear, down behind the ear into the hairline, then forward into the neck along a skin crease.
- Alternative: modified facelift incision - avoids a scar on the anterior (visible) neck, cosmetically superior.
- Infiltration with 1:100,000 adrenaline reduces hemorrhage and slightly aids facial nerve identification.
Raising Skin Flaps
- Skin flaps are raised containing subcutaneous tissue superficial to the parotid fascia, including the SMAS (superficial muscular aponeurotic system) layer.
- The parotid is mobilized from:
- Superiorly: cartilage of the tragus
- Posteriorly: mastoid tip and sternocleidomastoid muscle
- Inferiorly: posterior belly of the digastric muscle
- The greater auricular nerve (C2, C3) is encountered on the surface of the sternocleidomastoid and must be divided - preservation of its posterior branch should be attempted to reduce post-operative numbness of the earlobe.
- Wide exposure from superior to inferior, dissecting the gland off tragal cartilage and mastoid, is essential before seeking the facial nerve.
Identifying the Facial Nerve - Landmarks

Primary (Most Reliable) Landmarks
| Landmark | Relation to Facial Nerve |
|---|---|
| Tympanomastoid suture | Nerve lies immediately deep and inferior to this groove at its exit from skull - most reliable; can be felt with finger |
| Tragal pointer (inferior tip of cartilaginous EAC) | Nerve lies 1 cm deep and inferior to its tip. Note: slightly mobile when retracted so caution needed |
| Anterior border of posterior belly of digastric | Nerve exits skull immediately anterior to its mastoid attachment; careful dissection in this area exposes the nerve |
Caution
- The styloid process, though easy to palpate, lies deep to the nerve exit from the skull - dissecting onto it risks facial nerve damage.
Retrograde Nerve Identification (When Antegrade is Not Possible)
- Marginal mandibular branch: lies superficial to the facial vessels at the angle of the mandible.
- Cervical branch: pierces the deep fascia below the body of the mandible.
- Zygomatic and temporal branches (upper trunk): cross the zygomatic arch anterior to and within 1-2 cm of the superficial temporal artery.
Dissection and Gland Removal

- Once the main trunk is identified, its divisions and branches are followed anteriorly.
- The superficial lobe (or relevant part) is dissected off the facial nerve branches from deep to superficial using blunt dissection with fine instruments (mosquito clamp, nerve hook).
- The parotid duct (Stensen's duct) is ligated and divided.
- By this means, the superficial lobe is separated from the deeper parotid tissue and removed intact.
Tumor Rupture
- Can occur despite good technique, especially with myxoid pleomorphic adenomas.
- If rupture occurs: contain spillage, remove the adjacent deep lobe tissue to minimize seeding.
- Traditional teaching of copious irrigation with hypotonic water (not saline) is controversial - though the hypotonicity may lyse spilled cells, it may also disperse tumor cells over a wider area.
Wound Closure
- Hemostasis achieved.
- Drains usually placed (suction drains), but may not be necessary for lesser resections if haemostatic tissue glue is used.
- Caution with vacuum drains: if sections of unsupported facial nerve lie within the field, a vacuum drain can cause inadvertent neuropraxia by direct compression.
- Wound closed in layers, restoring the SMAS layer where possible (reduces risk of Frey's syndrome).
Facial Nerve Monitoring
- No evidence that routine use prevents permanent facial nerve injury.
- Most surgeons advocate its use in difficult or revision cases.
- Familiarity with monitoring is essential; this arguably makes a compelling case for routine use.
Extracapsular Dissection (ECD) - an Alternative
- Facial nerve is not formally identified.
- Same incision; tumor assessed for suitability after raising flaps.
- A plane is developed between tumor capsule and normal parotid tissue using traction/counter-traction.
- Facial nerve stimulator is essential throughout.
- Suitable for: mobile lesions in parotid tail, smaller tumors fairly superficial in superficial lobe.
- Unsuitable for: inflammatory lesions, large tumors, deep lobe extension, suspected malignancy.
- If doubt arises about nerve position: convert to partial parotidectomy with formal nerve identification.
- Recent systematic reviews (2025-2026) show ECD vs superficial parotidectomy comparisons continue to be studied, with ECD showing comparable recurrence rates in select cases (PMID: 40843726; 41430448).
Complications
Facial Nerve Injury
- Most important and feared complication.
- Temporary weakness (neuropraxia): up to 25-40% - usually resolves within weeks to months.
- Permanent weakness: ~2-3% for the marginal mandibular branch.
- All branches are at risk during dissection.
- Causes: traction, compression, ischemia, thermal injury, direct division.
Frey's Syndrome (Auriculotemporal Syndrome / Gustatory Sweating)
- Paint the ipsilateral face and neck with iodine solution; allow to dry.
- Dust starch powder over the painted area.
- Patient chews a sialagogue (lemon wedge) for several minutes.
- Dark blue spots (starch-iodine reaction where dissolved by sweat) confirm gustatory sweating.

- Antiperspirant applied to skin (first line for mild cases)
- Glycopyrrolate 1% roll-on lotion (anticholinergic)
- Botulinum toxin A subdermal injections - effective treatment; needs repeating every 6-12 months
- Tympanic neurectomy - surgical interruption of secretory fibers (Jacobson's nerve)
- More conservative surgery (partial/superficial rather than total parotidectomy)
- Restoration of the SMAS layer during closure (acts as barrier to reinnervation)
- Thick skin flaps
- Interpositional flaps (sternocleidomastoid muscle flap) - effective but not warranted routinely
Salivary Fistula / Sialocoele
- Occurs because there is always a cut surface of residual parotid gland (except in total parotidectomy).
- Presents within a few days: collection (sialocele - tense, painful, worse on eating) or leak through incision.
- Management: repeated aspiration, pressure dressings, wound care, antibiotics if infected.
- Hyoscine patches to reduce saliva production.
- If persistent: botulinum toxin injection into residual parotid gland under ultrasound control - temporarily stops saliva production; reverses over 2-3 months.
- Almost always settles within 1-2 weeks.
Greater Auricular Nerve Sensory Loss
- Numbness/dysesthesia of the earlobe and lower pinna - very common.
- Due to sacrifice of the greater auricular nerve; preservation of its posterior branch reduces the area of numbness.
Haematoma
- Early postoperative complication; requires surgical evacuation if large.
- Vacuum drains reduce incidence but must be placed carefully.
Scar / Cosmetic Deformity
- Parotid hollow/contour defect from gland removal.
- Properly placed lazy-S or facelift incision minimizes visible scarring.
Summary of Key Points
| Aspect | Key Points |
|---|---|
| Fundamental principle | Expose facial nerve first; remove gland around it |
| Incision | Lazy-S (modified Blair) or modified facelift |
| Most reliable landmark | Tympanomastoid suture |
| Tragal pointer | Nerve 1 cm deep and inferior to tip |
| Digastric belly | Nerve exits anterior to its mastoid attachment |
| Styloid caution | Lies deep to nerve - avoid dissecting onto it |
| Nerve monitoring | Not mandatory routinely; essential for revision/difficult cases |
| Rupture management | Remove adjacent deep lobe tissue; irrigation controversial |
| Drain placement | Caution - vacuum drain can cause neuropraxia |
| Permanent facial palsy | ~2-3% |
| Frey's syndrome | Subclinical: up to 96%; symptomatic: minority; treat with botulinum toxin |
| Salivary fistula | Almost always resolves; botulinum toxin if persistent |
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2, Chapter 9, p. 166-170
- Cummings Otolaryngology Head and Neck Surgery, Chapter 84, p. 1513-1521
- KJ Lee's Essential Otolaryngology, Auriculotemporal Syndrome section
Malignant salivary gland tumors
salivary gland malignant tumors treatment
Malignant Salivary Gland Tumors
Epidemiology
- Account for ~5% of all head and neck cancers; incidence of 2.5-3 per 100,000/year in the Western world.
- Estimated incidence: 0.9 per 100,000 in the USA; peaks at ages 65-74 years.
- Over 20 named malignant salivary gland neoplasms are recognized.
- Salivary gland malignancies are diverse and heterogeneous; their behavior and management are highly dependent on histologic type and grade.
Site-Malignancy Relationship
| Site | % of All Salivary Tumors | % Malignant |
|---|---|---|
| Parotid | 73% | ~15% |
| Submandibular | 11% | ~37% |
| Sublingual | 0.3% | ~86% |
| Minor salivary glands | 14% | ~46% |
Frequency of Malignant Types (Spiro's Series, n=1278)
| Histologic Type | % |
|---|---|
| Mucoepidermoid carcinoma | 34% |
| Adenoid cystic carcinoma | 22% |
| Adenocarcinoma NOS | 18% |
| Malignant mixed tumors | 13% |
| Acinic cell carcinoma | 7% |
| Squamous cell carcinoma | 4% |
WHO Classification of Malignant Epithelial Salivary Gland Tumors
- Mucoepidermoid carcinoma
- Acinic cell carcinoma
- Adenoid cystic carcinoma
- Adenocarcinoma NOS
- Carcinoma ex-pleomorphic adenoma
- Polymorphous adenocarcinoma
- Salivary duct carcinoma
- Myoepithelial carcinoma / Epithelial-myoepithelial carcinoma
- Secretory carcinoma
- Basal cell adenocarcinoma
- Intraductal carcinoma
- Clear cell carcinoma
- Carcinosarcoma
- Poorly differentiated / Undifferentiated carcinoma
- Small cell and large cell neuroendocrine carcinoma
- Lymphoepithelial carcinoma
- Squamous cell carcinoma
- Oncocytic carcinoma
- Sialoblastoma
Clinical Features Suggestive of Malignancy
| Feature | Significance |
|---|---|
| Rapid increase in size of a pre-existing mass | Especially in carcinoma ex pleomorphic adenoma |
| Facial nerve palsy (~10% of parotid malignancies) | Portends poor prognosis; may be mistaken for Bell palsy |
| Pain (constant, not episodic) | Episodic = obstruction/inflammation; constant = malignancy |
| Skin fixation or invasion | Late sign |
| Trismus | Infratemporal fossa involvement |
| Cervical lymphadenopathy | Regional metastasis |
| Numbness/paraesthesia | Perineural invasion (especially adenoid cystic carcinoma) |
| Fixation to deep structures | Locally advanced disease |
High-Grade Histologic Types
- High-grade mucoepidermoid carcinoma
- Squamous cell carcinoma
- Undifferentiated carcinoma
- High-grade adenocarcinoma NOS
- Solid-type (Grade III) adenoid cystic carcinoma
- Small cell carcinoma
- Salivary duct carcinoma
- Any tumor with "high-grade transformation"
Individual Tumor Types
1. Mucoepidermoid Carcinoma
- More frequent in females; can present at any age, peaks in the fifth decade.
- Most common malignancy in children and young adults (second decade peak in pediatric cases).
- Most common site: parotid gland (also occurs in minor salivary glands).
- Major risk factor: prior therapeutic radiation exposure (latent period 7-32 years).
| Parameter | Points |
|---|---|
| Intracystic component <20% | 2 |
| Neural invasion | 2 |
| Necrosis | 3 |
| Mitoses (>4/10 HPF) | 3 |
| Anaplasia | 4 |
| Grade | Total Score | 10-year Survival |
|---|---|---|
| Low | 0-4 | 90% |
| Intermediate | 5-6 | 70% |
| High | 7-14 | 25% |
- Low grade: macrocystic and microcystic, plentiful mucocytes, few epidermoid cells; can be mistaken for benign cyst.
- Intermediate grade: less circumscribed, more solid, predominant intermediate cell component.
- High grade: solid, infiltrative; nuclear atypia, mitoses, necrosis, perineural invasion, lymphovascular emboli; easily mistaken for SCC. At least focal intracellular mucin is essential for diagnosis.
- High-grade: locally aggressive with bone/skin involvement and nodal metastases; distant spread mainly to lungs.
2. Adenoid Cystic Carcinoma (AdCC / ACC)
- ~10-12% of all malignant salivary gland tumors.
- ~5% of parotid neoplasms; represents 30-50% of minor salivary gland malignancies.
- Ages 40s-60s; slight female preponderance (1.5:1); rare under 20 years.
- Can occur in oral cavity, paranasal sinuses, tracheobronchial tree.
- Slow-growing mass with numbness, paraesthesia, or pain (due to perineural invasion).
- Facial/other neural palsies depending on site.
- Asymptomatic lung metastases are frequent.
| Pattern | Features | Grade |
|---|---|---|
| Tubular | Most differentiated; true glandular/tubule-ductal spaces | Grade I |
| Cribriform | Most common; classic "Swiss cheese" appearance - pseudocysts containing basophilic mucoid basement membrane material | Grade II |
| Solid | Least common; sheets/nests, few glandular spaces, more pleomorphic cells, mitoses, necrosis | Grade III (worst prognosis) |
- Grade I: mostly tubular + some cribriform
- Grade II: entirely cribriform or with <30% solid component
- Grade III: >30% solid growth
- Radical surgical excision ± adjuvant radiotherapy.
- Single-modality radiotherapy: inferior control outcomes.
- Proton/carbon ion therapy: emerging role in unresectable or metastatic disease.
- Perineural spread along named nerves: radiation field must extend to the skull base.
3. Acinic Cell Carcinoma
- Low- to intermediate-grade tumor; ~7% of salivary gland malignancies.
- 90% occur in the parotid gland.
- Slight female predilection (1.5:1); typically presents in the fifth decade.
- Slow-growing, painless, mobile, solitary; rarely presents with facial palsy.
- Recapitulates serous acinar cells of normal salivary gland.
- Growth patterns: solid (most common), microcystic, papillary-cystic, follicular.
- Characteristic zymogen granules in serous acinar cells (demonstrated by histochemical stains); reactive lymphoid tissue is characteristic (can mimic lymph node metastasis).
- A small proportion may be high grade with metastasis to cervical nodes and lung.
4. Carcinoma Ex Pleomorphic Adenoma
- Most common malignant mixed tumor (>95% of all malignant mixed tumors).
- Accounts for ~3-5% of all salivary gland malignancies.
- Most common in parotid, then submandibular, minor salivary glands.
- Peak age: sixth and seventh decades (~one decade older than benign PSA).
- Poorly differentiated adenocarcinoma NOS
- Salivary duct carcinoma
- Undifferentiated carcinoma (Essentially any form of carcinoma can be found.)
| Classification | Definition | Prognosis |
|---|---|---|
| Noninvasive (intracapsular/in situ) | Within capsule | No risk of recurrence/metastasis after complete resection |
| Minimally invasive | ≤1.5 mm beyond capsule | Approaches behavior of benign PSA |
| Widely invasive | >1.5 mm beyond capsule | 5-year survival 26-65%; 20-year survival 0-38% |
5. Salivary Duct Carcinoma
- High-grade aggressive malignancy.
- Resembles high-grade ductal carcinoma of the breast histologically (comedonecrosis, cribriform architecture, Roman bridges).
- Predominantly affects the parotid gland in older males.
- Androgen receptor (AR) positive in many cases - relevant for hormonal therapy in recurrent/metastatic disease.
- Poor prognosis; frequent lymph node and distant metastases.
- Treatment: Surgery + radiotherapy; androgen deprivation therapy in AR-positive recurrent/metastatic cases.
6. Adenocarcinoma NOS
- Third most common malignant salivary gland neoplasm.
- Diagnosis of exclusion - malignant tumors with glandular/ductal differentiation that lack specific histological defining features.
- More common in women; peak in the fifth to eighth decade (mean age 58 years).
- ~60% occur in the parotid.
- Graded low, intermediate, high based on gland formation, nuclear pleomorphism, and mitotic count.
7. Squamous Cell Carcinoma
- Primary SCC of salivary glands is rare (~4%).
- Diagnosis of exclusion - must rule out metastasis from skin or mucosal SCC to intraparotid lymph nodes.
- High-grade behavior; poor prognosis.
- More common in elderly males.
8. Polymorphous Adenocarcinoma (PAC)
- Predominantly affects minor salivary glands (especially palate).
- Low-grade; characterized by uniform cytology but diverse architectural patterns (cribriform, tubular, papillary, solid).
- Good prognosis with surgery alone.
Summary Comparison Table
| Feature | Mucoepidermoid | Adenoid Cystic | Acinic Cell | Ca ex PSA |
|---|---|---|---|---|
| Frequency | Most common | 2nd overall; #1 in submandibular | 3rd | 3-5% of malignant |
| Primary site | Parotid | Submandibular/minor | Parotid (90%) | Parotid |
| Grade | Low-High | Grade I-III | Low-Intermediate | Variable |
| Perineural invasion | High-grade only | Hallmark | Rare | Present in high-grade |
| Facial palsy | High-grade | Yes (neural tracking) | Rare | Classic feature |
| Distant mets | Lung (high-grade) | Lung, bone, liver, brain | Rare | Common in invasive |
| Bilaterality | No | No | Rare (3%) | No |
| Prognosis | Grade-dependent | Good 5-yr; poor 10-yr | Generally favorable | Invasion-dependent |
| Key marker | PAS+ mucin | c-KIT+ (ductal) | PAS+ zymogen granules | Mixed PSA + carcinoma |
Investigations
| Investigation | Role |
|---|---|
| CT with contrast | Bone involvement, nodal metastases, deep lobe extension |
| MRI | Soft tissue extent, perineural spread, parapharyngeal involvement |
| FNA / Core biopsy | Tissue diagnosis (~80% sensitivity for benign vs. malignant) |
| Intraoperative frozen section | Guides surgical margins and extent |
| PET-CT | Staging, recurrence, distant metastasis; note: Warthin's also FDG-avid |
| Chest CT | Pulmonary metastases (especially adenoid cystic carcinoma) |
Treatment Principles
- Surgery: primary treatment for resectable disease. Extent depends on tumor size, location, grade, and facial nerve involvement.
- Facial nerve sacrifice: reserved for direct tumor invasion (not just proximity).
- Neck dissection: indicated for clinically/radiologically positive nodes; selective ND for high-grade histology even with N0 neck.
- Adjuvant radiotherapy indicated for:
- Advanced stage (T3/T4)
- Close or positive margins
- High-grade histologic types
- Perineural invasion
- Bone invasion / local tissue invasion
- AdCC (perineural spread along named nerves)
- Chemotherapy/systemic therapy: limited role in locoregional disease; used for recurrent/metastatic disease.
- A 2024 systematic review (PMID 39368417) on systemic treatments in recurrent/metastatic salivary gland cancer confirms no established standard; platinum-based regimens, HER2-targeted therapy (for HER2+ salivary duct carcinoma), and androgen deprivation remain areas of active investigation.
- Proton/carbon ion therapy: emerging for unresectable AdCC and other radio-resistant salivary malignancies.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2, Chapter 26, p. 481-485
- Cummings Otolaryngology Head and Neck Surgery, Chapter 85, p. 1524-1535
- Bailey & Love's Short Practice of Surgery, 28th Ed., Chapter 54, p. 861-862
- KJ Lee's Essential Otolaryngology, Classification of Salivary Gland Disorders
Sialendoscopy
sialendoscopy salivary duct
Sialendoscopy
Definition
Indications
| Category | Specific Conditions |
|---|---|
| Obstructive | Sialolithiasis (stones in Wharton's or Stensen's duct) |
| Inflammatory / chronic | Chronic sialadenitis, recurrent acute sialadenitis |
| Ductal pathology | Congenital and acquired ductal strictures |
| Autoimmune | Sjögren's syndrome (diagnostic and therapeutic) |
| Pediatric | Juvenile Recurrent Parotitis (JRP) - most common pediatric indication (68.9%) |
| Diagnostic | Unexplained salivary gland swelling without identifiable cause on imaging |
| Other | Ductal foreign bodies, duct trauma/injury localization |
- Most frequent indication: JRP (68.9%)
- Sialolithiasis: 14.7%
- Most common complication: ductal perforation
Contraindications
- Active infection - increases risk of ductal rupture and can compromise visualization due to bleeding and pus in the lumen.
- Severe trismus (impairs access to ductal papillae)
- Uncorrectable coagulopathy
Instrumentation
Types
- Equipped with fiberoptic light, image transmission, and occasionally an irrigation channel.
- Do not allow intraductal instrumentation.
- Compact: single non-disassemblable unit combining fiber light, fiber image transmission, a working channel, and an irrigation channel.
- Modular/semirigid: optical fibers combined into a probe that is introduced into sheaths of various sizes; the gap between probe and sheath provides the irrigation channel.
Standard Sizes - Erlangen (Karl Storz) Zero-Degree Telescope
| Size | Features |
|---|---|
| 0.8 mm | Integrated lens + irrigation only; no working channel |
| 1.1 mm | Integrated lens + irrigation + working channel |
| 1.6 mm | Largest; all channels; may be too large for some pediatric patients |
- Microdrill and laser fiber (holmium laser) to fragment larger stones
- Balloon dilator for ductal stenosis
- Wire basket for stone fragment extraction

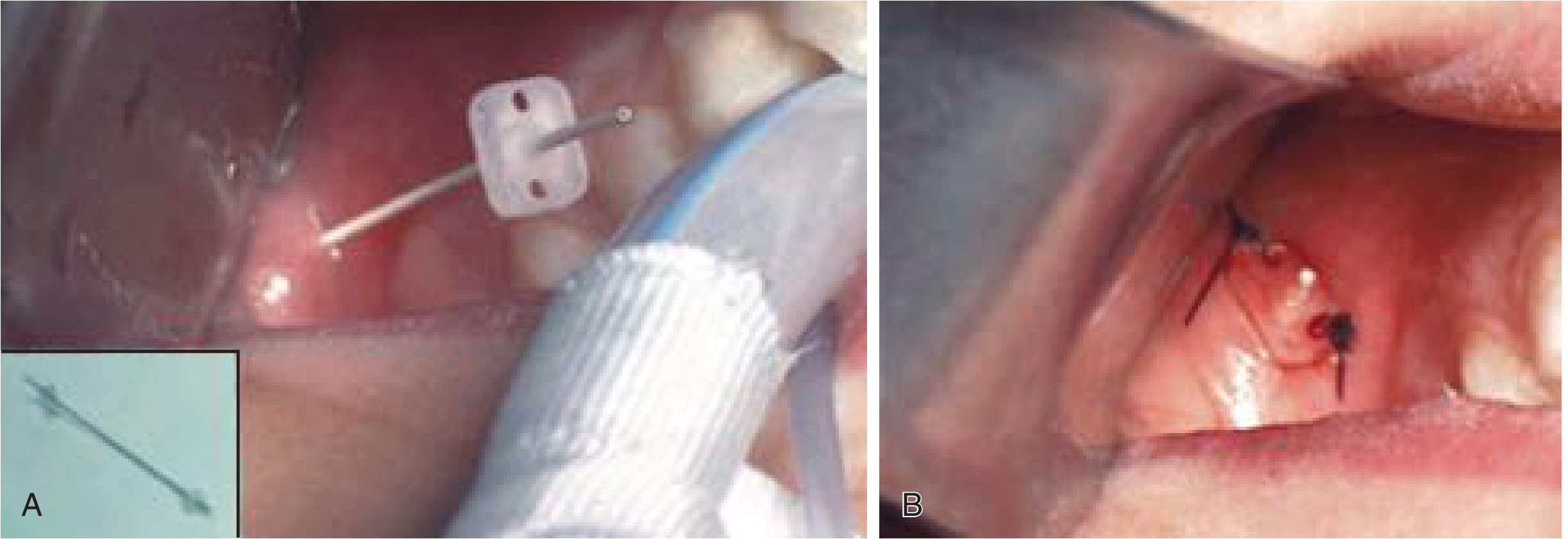
Operative Technique
- Anesthesia: Generally performed under general anesthesia; can be done under local anesthesia in cooperative children above 8 years.
- A bite block is placed on the contralateral side.
- Duct papilla identification: Locate the papilla of the affected gland:
- Parotid (Stensen's duct): opposite upper second molar in the buccal mucosa.
- Submandibular (Wharton's duct): floor of mouth at the sublingual caruncle lateral to the frenulum.
-
Serial dilation: The ductal orifice is serially dilated using salivary duct probes and dilators.
-
Endoscope introduction: The sialendoscope, attached to a camera and monitor, is introduced via the dilated orifice.
-
Exploration: Performed under continuous saline irrigation (keeps the view clear and hydrodilates the duct). The scope is advanced to the first branching point of the main duct; each branch is examined as far as the scope can comfortably pass.
-
Intervention (as required):
- Ductal stenosis: pneumatic balloon dilation.
- Small stones: wire basket retrieval.
- Larger stones: holmium laser or intraductal pneumatic lithotripsy to fragment, then basket retrieval.
- Combined approach: endoscope localizes the stone, then small external/intraoral incision extracts it at its location.
- Stent placement: post-dilation stents to prevent stricture reformation (up to 4 weeks).
Clinical Applications by Indication
Sialolithiasis
- Submandibular gland: 80-90% of sialoliths; most in the duct (Wharton's), making them accessible endoscopically.
- Parotid gland: 6-20%; stones often in the parenchyma, making them less accessible.
- Sialendoscopy can localize stones undetected by imaging.
- Stone size has traditionally been a contraindication to basket retrieval alone, but holmium laser fragmentation now allows treatment of most stone sizes.
- For stones that cannot be retrieved endoscopically: combined approach (endoscopic localization + small intraoral incision).
Chronic Sialadenitis
- Submandibular gland most frequently affected.
- Sialendoscopy serves as both diagnostic and interventional tool.
- Indication: more than one acute attack per year despite conservative management.
- Therapeutic endoscopy provides:
- Ductal lavage with continuous normal saline (washes out precipitated proteins and debris)
- Intraglandular steroid instillation (reduces inflammation)
- Hydrostatic dilation of the ductal system
- Balloon dilation of strictures
- Stenting to prevent stricture reformation
Juvenile Recurrent Parotitis (JRP)
- Self-limiting condition of recurrent painful parotid swelling in children.
- Sialendoscopy is now established as an effective treatment.
- Most common pediatric indication (68.9% of pediatric sialendoscopy cases).
- Mechanism: combines ductal lavage, hydrostatic dilation of sialectatic areas, and steroid instillation.
- Often dramatically reduces or eliminates recurrence episodes.
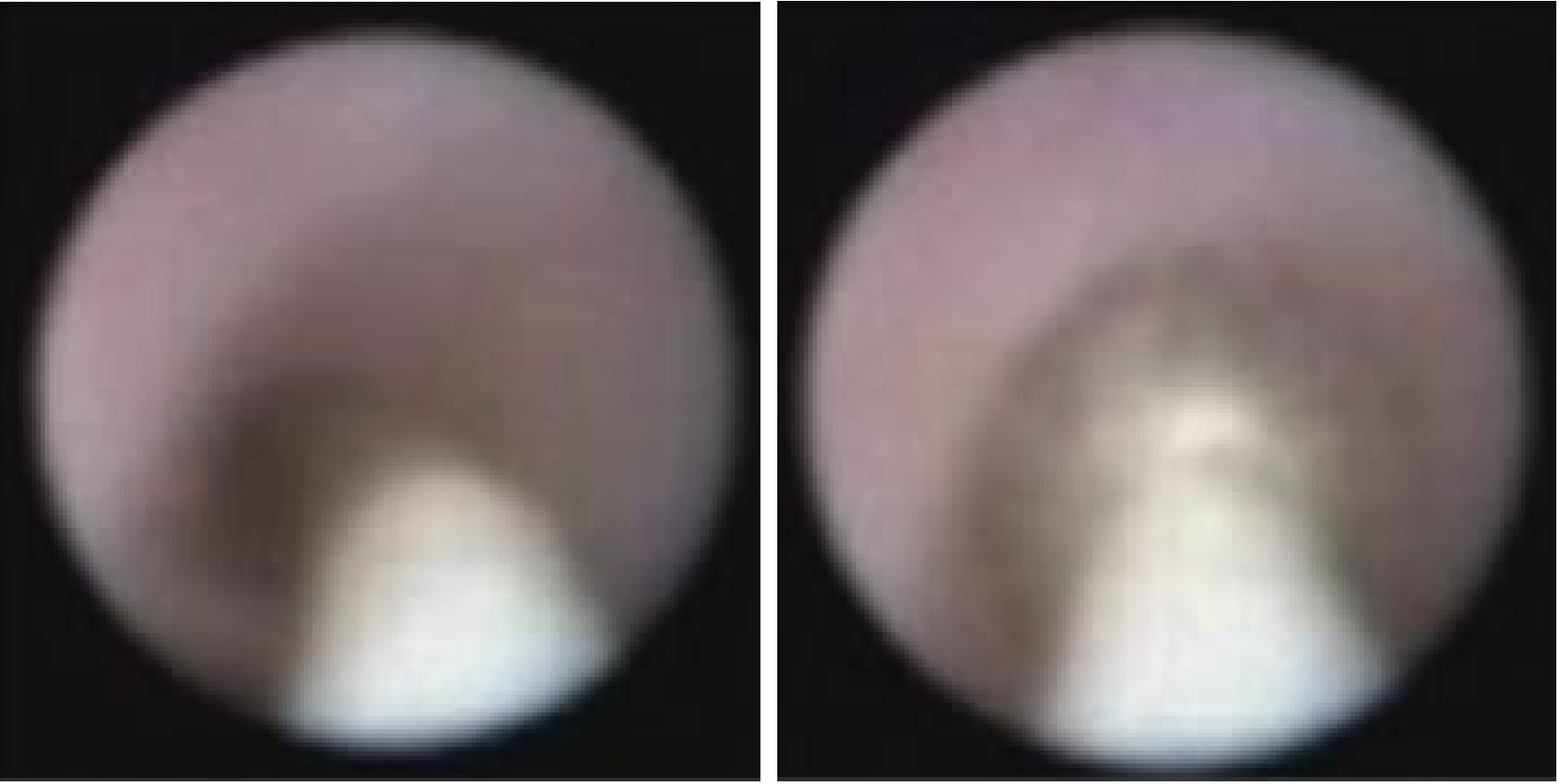
Sjögren's Syndrome
- Sialendoscopy allows direct visualization of characteristic endoscopic findings: mucosal pallor, whitish deposits, vascular pattern changes, and ductal stenoses.
- Therapeutic: ductal irrigation and steroid instillation provide symptomatic relief.
- Can be combined with other diagnostic steps.
Diagnostic Value
- Identifies ductal anatomy, stenoses, mucous plugs, stones, and inflammatory changes.
- Localizes stones beyond the reach of or invisible to traditional imaging (ultrasound, CT, MRI sialography).
- Documents response to treatment (pre- and post-dilation views).
Advantages Over Traditional Surgery
| Feature | Sialendoscopy | Gland Excision |
|---|---|---|
| Gland preservation | Yes | No |
| Access | Transoral/transductal | Open surgery |
| Recovery | Same-day / short | Longer |
| Facial nerve risk | None | Present (parotid) |
| Scarring | None | Yes |
| Repeat treatments | Possible | N/A |
Complications
| Complication | Notes |
|---|---|
| Ductal perforation | Most common, especially in pediatric cases; usually manageable conservatively |
| Ductal avulsion | Excessive force during dilation or basket manipulation |
| Swelling/edema | Post-procedure; usually temporary |
| Infection | Particularly if performed during active infection (contraindicated) |
| Incomplete stone removal | Larger or impacted stones may require combined approach |
| Stricture reformation | Prevented by stenting post-dilation |
Sialolithiasis - Site Distribution (for context)
| Site | Frequency |
|---|---|
| Submandibular gland | 80-90% |
| Parotid gland | 6-20% |
| Sublingual and minor salivary glands | 1-2% |
- Wharton's duct is longer, travels upward against gravity
- Submandibular saliva is more viscous and calcium-rich
- Submandibular stones are more often in the duct (accessible), while parotid stones tend to be in the parenchyma (less accessible)
Summary
- Cummings Otolaryngology Head and Neck Surgery, Chapter 83 (Chronic Sialadenitis, p. 1489-1490) and Chapter 205 (Pediatric Sialendoscopy, p. 3871-3883)
- KJ Lee's Essential Otolaryngology, Sialadenitis section
Sialithiasis
sialolithiasis salivary gland stones treatment
Sialolithiasis (Salivary Calculi)
Definition
Epidemiology
- Patients in their fifth to eighth decades most commonly affected.
- Sialolithiasis in children is rare; when it occurs, presentation is typically around age 10.
- Men develop calculi more frequently than women.
- Unilateral in the vast majority of cases.
Distribution by Gland
| Gland | Frequency | Stone Location |
|---|---|---|
| Submandibular (Wharton's duct) | 80-90% | Usually in the duct |
| Parotid (Stensen's duct) | 10-20% | Usually at the hilum or parenchyma |
| Sublingual / minor glands | ~1-2% | Rare |
Why the Submandibular Gland Is Predominantly Affected
- Longer duct (Wharton's): Greater distance for saliva to travel.
- Tortuous course: The duct angulates around the posterior border of the mylohyoid muscle, travelling against gravity - slowing flow.
- Wider duct lumen: Allows more stagnation.
- More viscous saliva: Submandibular saliva has higher mucin content.
- Higher calcium and phosphate concentration: Submandibular saliva is richer in calcium and phosphate.
- Slower salivary flow rate: Consequent poor salivary egress into the oral cavity.
Composition and Pathogenesis
- The precise etiology remains unknown.
- Salivary stasis + ductal inflammatory changes are the key contributing factors.
- Intermittent stasis → alteration of mucoid elements of saliva → formation of an organic gel → framework for salt deposition → calculus formation.
- Serum calcium and phosphate levels are not related to stone formation.
- Submandibular: Stone forms first → salivary stasis → ascending retrograde bacterial infection → sialadenitis.
- Parotid: Chronic sialadenitis (ductal injury and inflammation) is the inciting event → secondary sialolith formation.
- Obstruction of ductal orifice by impacted food debris or local edema after injury
- Long-term phenothiazines or other drugs reducing salivary secretion
- Dehydration (especially elderly post-major surgery)
Clinical Features
Symptoms
- Salivary colic: recurrent episodes of postprandial pain and swelling of the affected gland - pathognomonic presentation.
- Pain begins with eating (when salivary flow increases against the obstruction).
- Swelling typically subsides over 1-2 hours as salivary flow diminishes.
- History of multiple episodes of acute suppurative sialadenitis.
- Foul-tasting fluid on massaging the gland (retrograde bacterial contamination with mucopus).
Signs
- Swelling of the affected gland (firm, tender during episodes).
- Bimanual palpation (one finger intraoral, one external): may reveal a palpable stone in Wharton's duct coursing through the floor of the mouth.
- Parotid stones may be palpable at the Stensen's duct orifice (opposite the upper second molar) or along the duct.
- Reduced or absent salivary flow on bimanual palpation/massage of the obstructed gland.
- Saliva quality may be mucoid, particulate, or mucopurulent from the affected duct orifice.
Investigations
Imaging
- Cost-effective, no radiation, repeatable, and dynamic.
- Can detect 90% of stones >2 mm.
- Provides excellent definition of the salivary gland and stone mobility.
- Can be used intraoperatively for stone localization.
- Bedside USS is useful in the emergency setting.

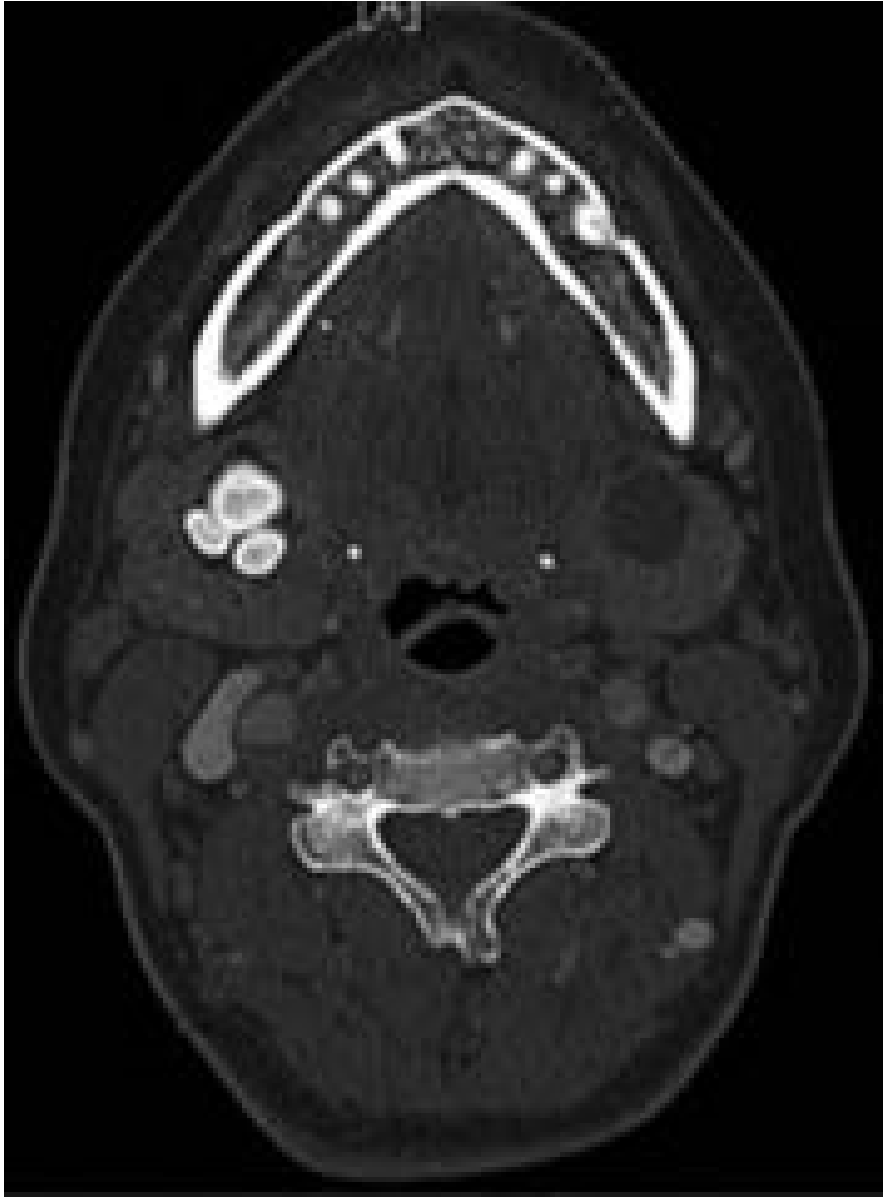
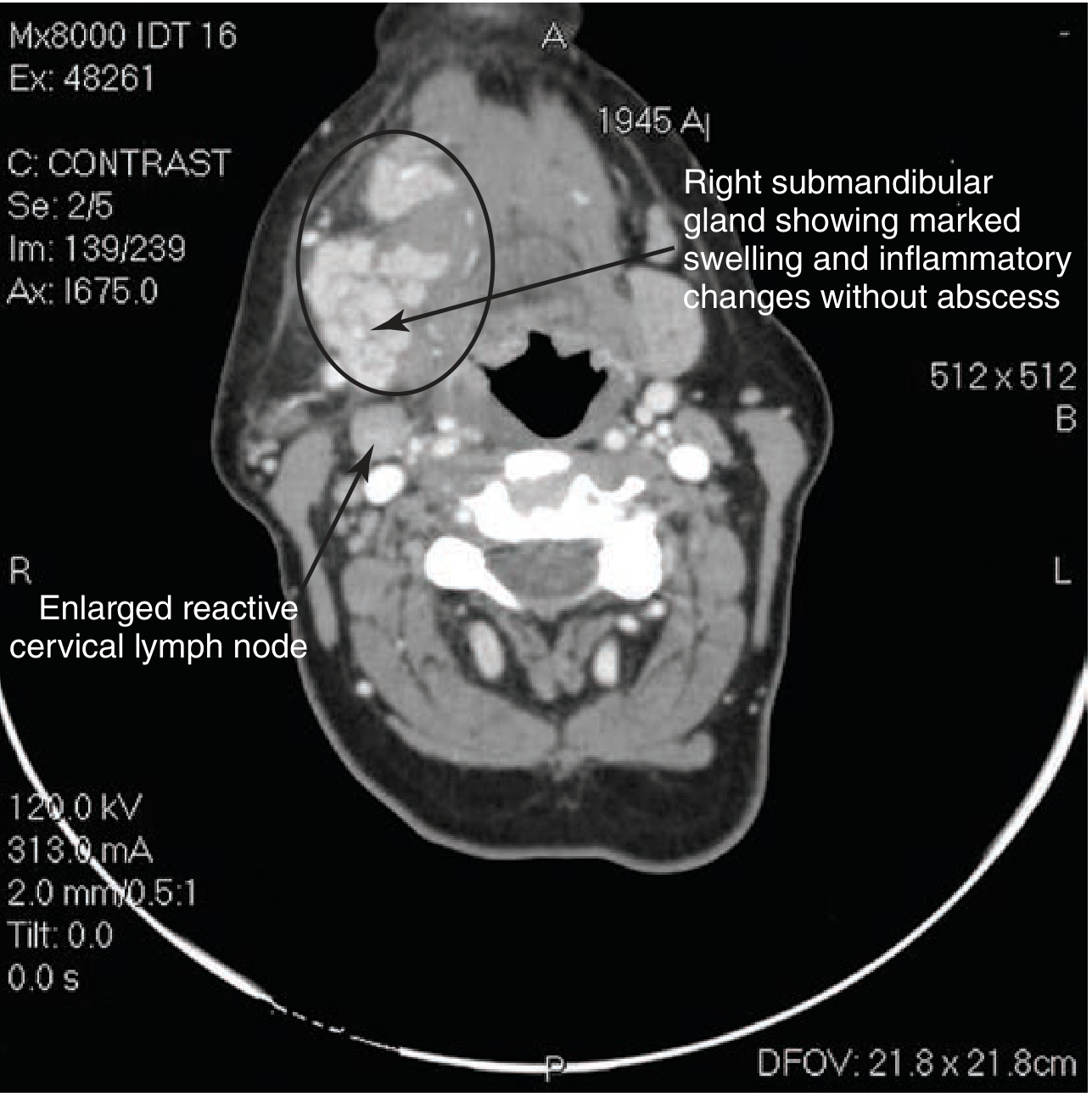
- Fine cuts (1-2 mm) are extremely accurate for detecting stones.
- Non-contrast preferred: contrast-enhanced vessels can be confused with sialoliths.
- In cases where malignancy is also suspected, CT with and without contrast should be obtained.
- Findings: enlarged gland + ductal dilation + hyperdense stones.
- Can make the diagnosis from glandular swelling and inflammatory changes even when the stone is not directly visible in the duct.
- Saliva acts as natural contrast medium (T2-weighted).
- Non-invasive; accuracy similar to digital sialography.
- Stone appears as low signal intensity focus on T1 and T2.
- Superior to ultrasound; useful when digital sialography is contraindicated.
- Limitation: ductal metaplasia of sialolithiasis may be misinterpreted as mucoepidermoid carcinoma.
- Traditionally used; now largely replaced.
- Stones are radiopaque in ~70% of cases (stones with less calcium may be radiolucent).
- Misses radiolucent stones; may confuse stones with phleboliths, arterial calcification (lingual artery), or calcified cervical lymphadenopathy.
- Sensitivity 95-100% for detecting radiolucent stones.
- Invasive; contraindicated in active infection and for stones in the oral portion of Wharton's duct.
- Reserved for complex cases alongside 3D reconstructions.
Management
Conservative (First-Line for All)
- Sialagogues (lemon drops, sour candy, vitamin C) - stimulate saliva flow to flush the stone.
- Hydration - corrects dehydration contributing to stasis.
- Gland massage - manually expressed from proximal to distal.
- Local heat - warm compresses over the gland.
- NSAIDs/analgesics - symptom relief.
- Antibiotics - if infection is suspected (not routine).
- "Milking" - palpable distal duct stones can sometimes be manually expressed through the orifice.
Interventional Management
Step 1 - Transoral Duct Incision (for palpable, distal stones)
- Submandibular stones ≤2 cm from the duct orifice, distal to the posterior edge of the mylohyoid, palpable in the floor of the mouth.
- Transoral incision directly into the duct over the stone, under local anaesthesia.
- Stone retrieved; the duct is marsupialized (left open) rather than sutured, to prevent stricture.
- Care taken to avoid the lingual nerve (runs close to the duct in the floor of the mouth).
Step 2 - Sialendoscopy (Minimally Invasive, Gland-Preserving)
- Wire basket retrieval: direct visualization; basket ensnares and extracts the stone.
- Holmium laser lithotripsy or pneumatic lithotripsy: fragments larger stones into pieces manageable with a basket.
- Success rates: 80-100% using endoscopic ± combined approaches.
- A salivary stent may be left in place for 2-4 weeks post-procedure to prevent ductal stenosis.
Step 3 - Combined / Hybrid Approach
- Endoscope localizes the stone under direct visualization; an external or intraoral incision is made over the stone to extract it.
- Used when pure endoscopic retrieval fails (impacted stone, stone too large for basket).
- For parotid stones: may require a partial/complete parotidectomy incision and SMAS flap elevation to access the stone.
Step 4 - Gland Excision (When All Else Fails)
- Submandibular gland excision: traditionally the management for proximal, hilar, intraglandular, impacted, large stones (megaliths), or when conservative/endoscopic approaches fail.
- Parotidectomy: for intraglandular parotid stones not amenable to endoscopic removal.
Summary - Management Algorithm
Stone detected on imaging
↓
Conservative: Sialagogues + hydration + massage + heat
↓ (if not passed)
Location assessment:
┌─────────────────────────────────────────────────────────────┐
│ Distal, palpable, ≤2 cm from orifice │
│ → Transoral duct incision (milking or direct excision) │
│ │
│ Proximal, impacted, or not palpable │
│ → Sialendoscopy ± lithotripsy (wire basket/laser) │
│ → If fails: Combined approach (endo + external incision)│
│ → If fails: Gland excision │
└─────────────────────────────────────────────────────────────┘
Complications of Untreated/Recurrent Sialolithiasis
| Complication | Notes |
|---|---|
| Chronic sialadenitis | Recurrent inflammation → fibrosis and acinar atrophy |
| Acute suppurative sialadenitis | Retrograde bacterial infection; S. aureus most common |
| Ductal stricture | Post-inflammatory; causes ongoing obstruction |
| Gland atrophy | Progressive fibrotic replacement of acinar tissue |
| Abscess formation | Severe, untreated infection |
Surgical Anatomy Notes (Transoral Wharton's Duct Approach)
- Wharton's duct runs in the floor of the mouth alongside the lingual nerve.
- Intraoral stone excision: incise along the duct (not across it); marsupialize rather than suture to prevent stricture.
- The lingual nerve crosses the duct laterally then inferiorly - risk of injury with overzealous dissection.
Recent Evidence
- Cummings Otolaryngology Head and Neck Surgery, Chapter 83, p. 1487-1488
- Tintinalli's Emergency Medicine, Chapter 243, p. 1611
- Robbins & Cotran Pathologic Basis of Disease, Chapter 16
- Bailey & Love's Short Practice of Surgery, 28th Ed.
Parotid anatomy
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.3.content.30.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.
Parotid anatomy
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.9.content.35.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.