Steps of open cholecystectomy
Reading File
Finding Sources
Searching the Web
open cholecystectomy surgical steps technique
Reading File
Searching Images
open cholecystectomy Calot triangle dissection surgical technique
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed from multiple authoritative surgical textbooks (Schwartz's, Sabiston, Current Surgical Therapy, Mulholland & Greenfield's). Here is the comprehensive answer:
Open Cholecystectomy — Surgical Steps
Open cholecystectomy is now mostly performed as a conversion from laparoscopy or when laparoscopy is contraindicated (hemodynamic instability, uncontrolled coagulopathy, severe COPD/CHF, frank peritonitis). It can be performed via two approaches: retrograde (fundus-down) or anterograde (Calot-first).
1. Preoperative Preparation
- CBC and liver function tests
- DVT prophylaxis: LMWH or compression stockings
- Patient empties bladder preoperatively
- Informed consent including discussion of conversion risk, bile duct injury, and bleeding
2. Position & Anesthesia
- Supine position under general anesthesia
- Nasogastric tube and urinary catheter placed
- Right upper quadrant exposure optimized; reverse Trendelenburg with right-side-up tilt is helpful
3. Incision
Two options:
- Right subcostal (Kocher) incision — most commonly used; provides excellent exposure of the gallbladder bed and cystic duct
- Upper midline incision — acceptable alternative, especially if another concurrent procedure is planned (e.g., pancreaticoduodenectomy)
A wound protection device is often placed.
4. Abdominal Exploration & Exposure
- Systematic abdominal exploration for unexpected pathology
- Adhesions between omentum, duodenum, or colon and the gallbladder are taken down
- Retractors placed for adequate exposure of the right upper quadrant
- Liver retracted superiorly; duodenum retracted inferiorly to expose the hepatoduodenal ligament
5. Gallbladder Retraction
- The fundus and body of the gallbladder are grasped
- Countertraction is applied to place the gallbladder on stretch
- This exposes the triangle of Calot (hepatocystic triangle: bounded by the cystic duct, common hepatic duct, and inferior liver margin)
6. Dissection — Two Approaches
A. Retrograde / Fundus-Down (Traditional)
- Electrocautery dissects the peritoneum at the fundus of the gallbladder off the liver bed
- Dissection proceeds downward toward the infundibulum and Calot's triangle
- The posterior wall of the gallbladder is peeled off the liver bed (cystic plate plane)
- Caution: when working below the midpoint of the gallbladder fossa, re-enter a superficial plane to avoid injury to hilar structures
- Medial and lateral peritoneum overlying the gallbladder and infundibulum are incised with cautery
- Continue until infundibulum and cystic duct–artery junction are exposed
B. Anterograde / Calot-First
- Dissection begins at the triangle of Calot
- Peritoneum, fat, and loose areolar tissue around the cystic duct–gallbladder junction are dissected off and reflected inferiorly
- The critical view of safety (CVS) is achieved before dividing any structure (see Step 7)
- After ligation/division of cystic duct and artery, the gallbladder is dissected off the liver bed
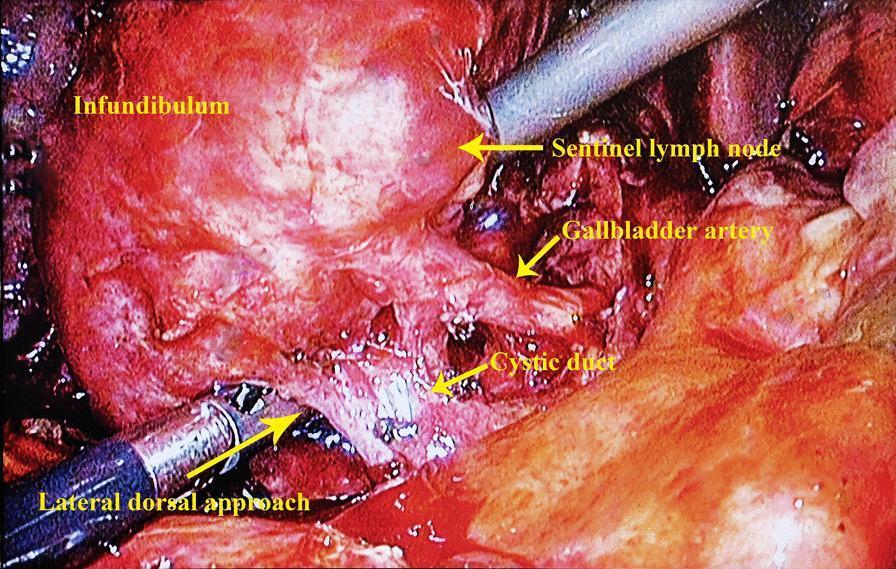
7. Identification of Cystic Artery and Cystic Duct (Critical View of Safety)
Before ligating anything, confirm the Critical View of Safety:
- Hepatocystic triangle is cleared of fat and fibrous tissue
- The lower one-third of the gallbladder is separated from the liver
- Only two structures are seen entering the gallbladder (cystic duct + cystic artery)
The cystic artery typically runs parallel to and slightly behind the cystic duct, often posterior to the node of Calot (sentinel lymph node — a reliable landmark). Blunt dissection with thumb and index finger can be used in inflamed cases.
8. Ligation of Cystic Artery
- Cystic artery is doubly ligated with suture ligatures or clips and divided
- Early ligation limits blood loss — but must be done only after positive identification
- Be aware: right hepatic artery may be mistaken for the cystic artery in anatomic variants
9. Division of Cystic Duct
- Cystic duct is ligated distally (near the common bile duct junction) and proximally (at the gallbladder neck) and divided between
- Intraoperative cholangiogram (IOC) may be performed at this stage: a small opening is made in the cystic duct, a catheter inserted, and contrast injected to delineate biliary anatomy and detect choledocholithiasis
- Duct and artery can be divided between clips and/or sutures
10. Gallbladder Dissection from Liver Bed
- Gallbladder is dissected off the cystic plate using electrocautery
- Direction: either fundus-down (already separated) or infundibulum upward to fundus
- The cystic plate is a fibrous layer separating the gallbladder from liver parenchyma — staying in this plane minimizes bleeding
11. Hemostasis & Inspection
- Liver bed is inspected for bleeding and bile leakage
- Electrocautery or suture ligatures used for hemostasis
- The bile duct, right hepatic artery, and portal vein are visually confirmed to be intact
12. Drain Placement (Selective)
- Routine drains are NOT recommended for uncomplicated cholecystectomy (no evidence of benefit, may increase harm)
- Drain may be considered in: necrotic gallbladder, gangrene, empyema, subtotal cholecystectomy, or high bile-leak risk
13. Closure
- Abdominal wall closed in layers
- Fascial layer closed with continuous or interrupted sutures
- Subcutaneous layer irrigated if contaminated
- Skin closed with staples or sutures
Key Safety Points
| Risk | Prevention |
|---|---|
| Bile duct injury (0.2–0.3% open; higher laparoscopic) | Achieve Critical View of Safety before dividing any structure |
| Right hepatic artery injury | Confirm cystic artery is small and enters gallbladder wall before ligation |
| Portal vein injury | Avoid dissecting too far inferiorly near the hepatoduodenal ligament |
| Retained CBD stones | Perform IOC when indicated |
| Stone spillage | Remove all spilled stones to prevent abscess/fistula |
Sources: Schwartz's Principles of Surgery (11e), Sabiston Textbook of Surgery, Current Surgical Therapy (14e), Mulholland & Greenfield's Surgery (7e)
This is a shared conversation. Sign in to Orris to start your own chat.