Leprosy
Reading File
Finding Sources
Searching PubMed
leprosy Hansen disease
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Reading File
I now have rich content for a comprehensive answer. Let me compile the full response.
Leprosy (Hansen Disease)
Overview
Leprosy is a slowly progressive chronic infection caused primarily by Mycobacterium leprae (and rarely M. lepromatosis, proposed name since 2008) that mainly affects the skin and peripheral nerves. Despite its low communicability, it remains endemic with approximately 200,000 new cases per year in low-resource tropical nations, particularly Southeast Asia, East Africa, and Brazil.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 357
Etiology & Pathogenesis
- M. leprae is an obligate intracellular pathogen - it cannot be cultured in vitro
- Replicates optimally at 32-34°C (temperature of human skin and superficial tissues), which explains why the CNS and vital organs are usually spared
- Transmission: mainly via respiratory droplet/secretion from untreated patients; rare zoonotic transmission from armadillos
- Virulence is determined by cell wall lipid PGL-1, which enables invasion of host cells
- M. leprae inhibits mitochondrial energy metabolism to evade immunity
- Similar enough to M. tuberculosis that BCG vaccination confers partial protection
- The spectrum of disease is determined by the host's T-helper lymphocyte response
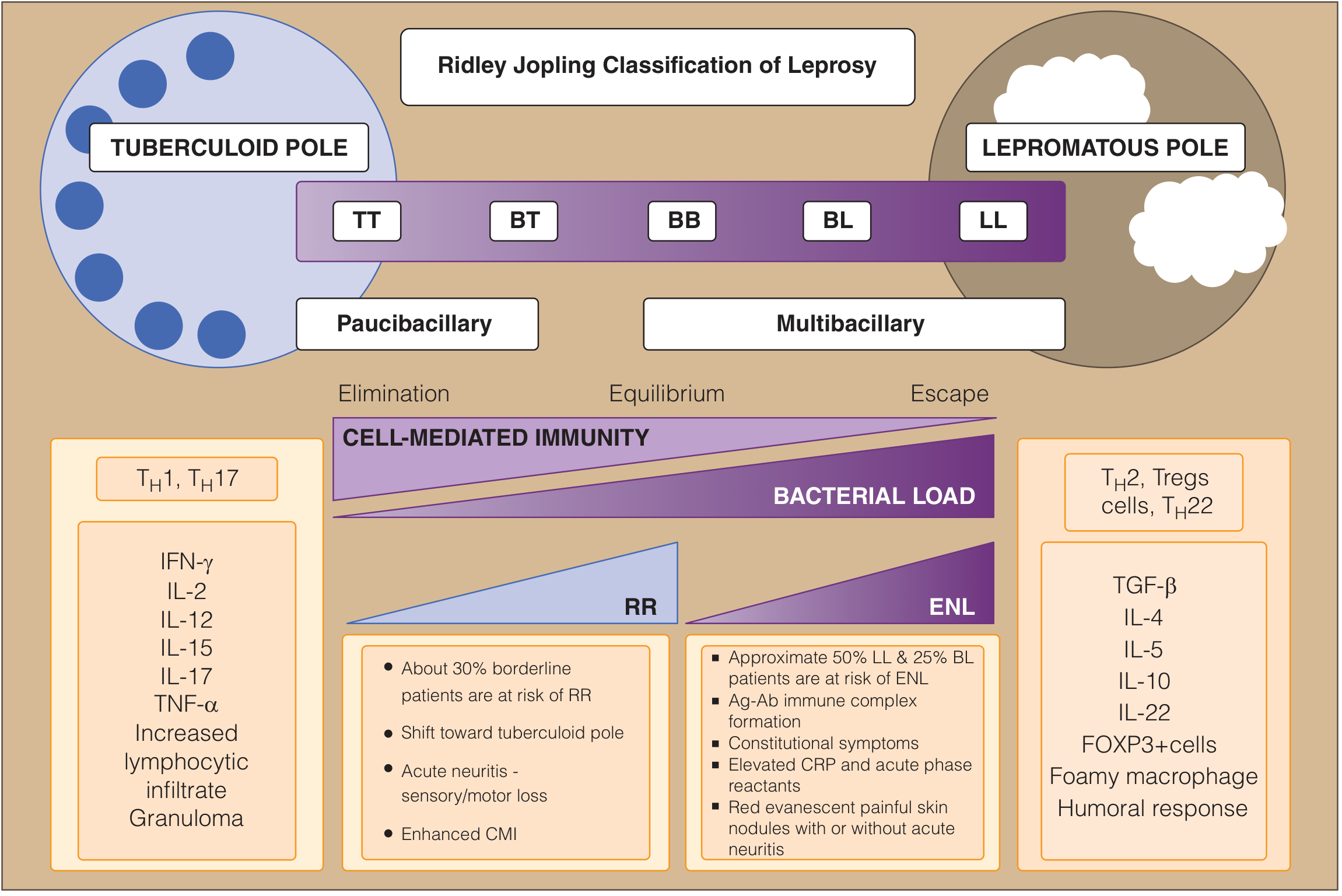
Classification
Ridley-Jopling Spectrum
The disease spans a spectrum from tuberculoid (strong cell-mediated immunity) to lepromatous (weak cell-mediated immunity):
WHO Operational Classification
| Type | Criteria |
|---|---|
| Paucibacillary (PB) | 1-5 skin lesions, negative slit-skin smear, no nerve involvement |
| Multibacillary (MB) | >5 skin lesions, OR nerve involvement (pure neuritic), OR positive slit-skin smear regardless of lesion count |
PB roughly corresponds to TT and BT; MB to BB, BL, and LL.
- Goldman-Cecil Medicine, Table 301-1
Clinical Features
Tuberculoid Leprosy (TT/BT)
- 1-3 skin lesions, well-defined erythematous plaques with raised edges sloping inward
- Surface is dry, scaly, hairless, and anesthetic (loss of sensation is hallmark)
- Asymmetric large peripheral nerve involvement dominates - nerves become enclosed in granulomatous reactions
- Nerve degeneration causes anesthesia, muscle atrophy, and susceptibility to trauma
- Contractures, paralyses, and autoamputation of digits can ensue
- Facial nerve involvement - eyelid paralysis, keratitis, corneal ulceration
- Histology: granulomas resembling tuberculosis; bacilli almost never found (paucibacillary)
- Strong Th1/Th17 response with IL-2, IFN-γ production
Lepromatous Leprosy (LL/BL)
- Symmetric widespread skin thickening and nodules
- Involves: skin, peripheral nerves, anterior eye chamber, upper airways (to larynx), testes, hands, and feet
- Macular, papular, or nodular lesions on face, ears, wrists, elbows, knees
- With progression: nodules coalesce to yield leonine facies
- Sensory loss in typical stocking-and-glove distribution
- Nasal involvement in up to 40%: crusting, bleeding, septal perforation, anosmia
- Testes extensively involved: destruction of seminiferous tubules, sterility, gynecomastia
- Peripheral nerves (ulnar, peroneal) symmetrically invaded with minimal inflammation
- Histology: lepra cells - large aggregates of lipid-laden macrophages filled with masses ("globi") of acid-fast bacilli (multibacillary)
- Weak Th1, relative increase in Th2/Tregs: poor bacterial control
Borderline (BB)
- Most clinically unstable form
- Annular skin lesions with "punched-out" inner edge and ill-defined outer edge
Histopathology
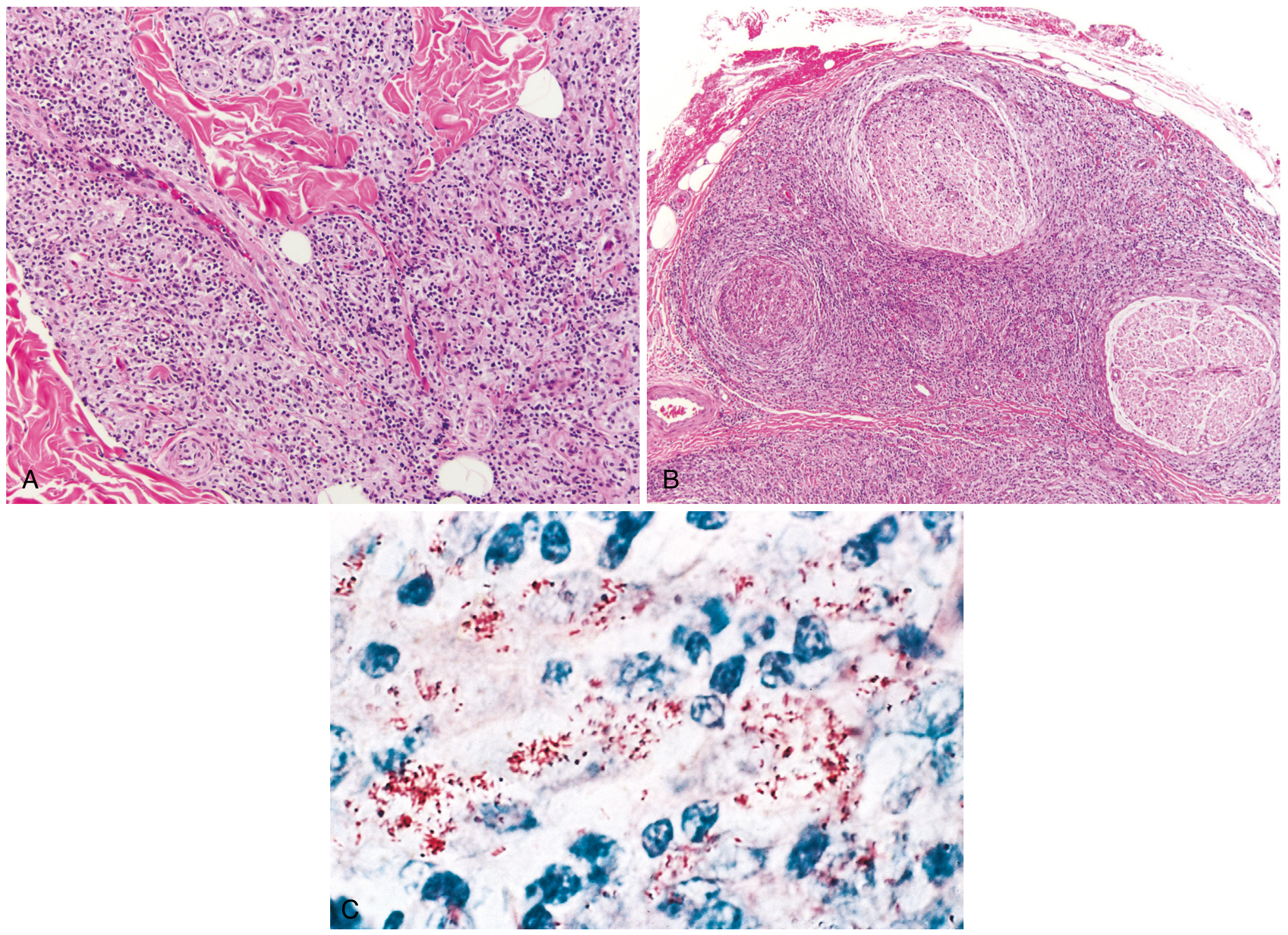
Fig. 8.33 Leprosy - Robbins Pathology: (A) Tuberculoid type: dense dermal macrophage infiltration around adnexa, vessels and nerves. (B) Lepromatous type: dense lymphocytic and macrophage infiltration into large nerve bundles. (C) Acid-fast bacilli within macrophages (lepromatous form).
Lepra Reactions (Immunologic Complications)
Reactions are immunologically mediated episodes of acute/subacute inflammation affecting skin and nerves - major causes of nerve damage and disability.
Type 1 Reaction (Reversal Reaction - RR)
- Delayed hypersensitivity reaction; sudden alteration of cell-mediated immunity
- Mostly in borderline disease (~30% of borderline patients)
- Represents a shift toward the tuberculoid pole (enhanced CMI)
- Existing skin patches become erythematous, swollen, tender
- Rapid, painful swelling of peripheral nerves (acute neuritis); nerve abscesses possible
- Edema of extremities and face
Type 2 Reaction (Erythema Nodosum Leprosum - ENL)
-
Immune complex (Ag-Ab) mediated reaction
-
Occurs in lepromatous (LL) and borderline lepromatous (BL) disease (~50% LL, ~25% BL patients)
-
Presents with red, evanescent, painful skin nodules; systemic features (fever, constitutional symptoms)
-
Elevated CRP and acute-phase reactants; may cause acute neuritis
-
Can cause vasculitis and glomerulonephritis through immune complex deposition
-
Goldman-Cecil Medicine, pp. 3275-3276
Diagnosis
- Slit-skin smear - most simple and valuable test; used to count and grade acid-fast bacilli (Bacteriologic Index 0 to 6+); Morphologic Index assesses viability (solid = live; granular/fragmented = dead)
- Skin biopsy - confirms diagnosis and type; identifies reactions
- Fine needle aspiration cytology - useful in neuritic leprosy
- Clinical diagnosis is standard in endemic settings
- M. leprae cannot be cultured in vitro - no in-vitro culture test available
Treatment: WHO Multidrug Therapy (MDT)
MDT consists of rifampicin + dapsone ± clofazimine. The current regimen dates to 1982 and is highly successful for curing all forms of leprosy.
| Regimen | Drugs | Duration |
|---|---|---|
| Paucibacillary | Rifampicin 600 mg once monthly (supervised) + Dapsone 100 mg daily (self-administered) | 6 months |
| Multibacillary | Rifampicin 600 mg once monthly (supervised) + Dapsone 100 mg daily (self-administered) + Clofazimine 300 mg once monthly (supervised) + Clofazimine 50 mg daily (self-administered) | 12 months |
Key drug roles:
- Rifampicin: highly bactericidal; given monthly (as opposed to daily dapsone/clofazimine)
- Dapsone: bacteriostatic; daily; dapsone-resistance drove the move from monotherapy to MDT in the 1970s
- Clofazimine: bacteriostatic + anti-inflammatory; well-tolerated
Reactions management:
-
Type 1 (RR): oral corticosteroids
-
Type 2 (ENL): thalidomide (drug of choice where available) or corticosteroids
-
Goldman-Cecil Medicine, Table 301-3; Fitzpatrick's Dermatology; Goodman & Gilman's
Complications & Deformities
- Peripheral neuropathy (glove and stocking sensory loss)
- Claw hand, foot drop (ulnar, peroneal nerve palsy)
- Plantar ulcers from repeated painless trauma
- Facial disfigurement (leonine facies, nasal collapse)
- Blindness (corneal anesthesia, lagophthalmos, uveitis)
- Testicular destruction and infertility
- Amyloidosis in long-standing disease
Special Notes
- Pregnancy: cell-mediated immunity is suppressed during pregnancy, so leprosy becomes more active; relapse and reactivation can occur despite MDT; some drugs may be contraindicated
- Animals: nine-banded armadillos are the only known natural reservoir besides humans (relevant in the southern United States)
- Most patients die with leprosy rather than of it, given its extremely slow course spanning decades
Recent Evidence (PubMed, 2024-2026)
- A 2024 systematic review on leprosy immunopathogenesis (PMID 39308868) updates the immune mechanisms underlying the tuberculoid-lepromatous spectrum
- A 2024 systematic review on self-healing in leprosy (PMID 39264863) examines spontaneous resolution
- A 2026 systematic review on corticosteroid adverse effects in leprosy reactions management (PMID 41886473) is particularly relevant for treating Type 1 and Type 2 reactions safely
Hemiplegia
Reading File
Finding Sources
Finding Sources
Searching PubMed
hemiplegia stroke rehabilitation
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have enough comprehensive content to write a thorough answer. Let me compile the full response.
Hemiplegia
Definition
Hemiplegia is paralysis (complete loss of voluntary movement) of one side of the body - arm, leg, and often the lower face on the same side. Hemiparesis refers to weakness rather than complete paralysis. It is the most frequent form of paralysis in clinical neurology and, with rare exceptions, always results from a lesion in the corticospinal (pyramidal) pathways.
- Adams and Victor's Principles of Neurology, 12th Ed.
Anatomy: The Corticospinal Pathway
The corticospinal tract courses from motor cortex → corona radiata → internal capsule (posterior limb) → cerebral peduncle → pons → medullary pyramid → decussation → contralateral spinal cord. A lesion at any level can cause hemiplegia:
| Level | Motor Features | Distinguishing Clues |
|---|---|---|
| Cerebral cortex | Focal weakness (arm, face, or leg predominant) | Aphasia (dominant), neglect (non-dominant), seizures, sensory loss |
| Corona radiata / subcortical WM | Arm + leg + face contralateral | May have cortical signs |
| Internal capsule | Contralateral arm + leg + lower face (equivalent involvement) | Pure motor hemiplegia; no cortical signs |
| Brainstem | Contralateral limbs + ipsilateral cranial nerve palsy ("crossed hemiplegia") | CN palsies, diplopia, vertigo, ataxia |
| Spinal cord (cervical) | Ipsilateral hemiplegia (rare); face spared | Brown-Séquard if unilateral; bilateral signs common |
Note: attribution of a capsular hemiplegia solely to the pyramidal tract is not entirely correct - in the internal capsule, corticospinal fibers are intermingled with corticostriate, corticothalamic, corticorubral, corticopontine, and corticoreticular fibers. The term "upper motor neuron (UMN) paralysis" is more accurate.
- Adams and Victor's Principles of Neurology
Upper Motor Neuron (UMN) Features
Hemiplegia from a central (UMN) lesion is characterized by:
- Spasticity - velocity-dependent increase in muscle tone (due to corticoreticulospinal pathway involvement)
- Hyperreflexia - exaggerated deep tendon reflexes
- Extensor plantar response (Babinski sign) - upgoing toe on plantar stimulation
- Clonus - rhythmic involuntary contractions, especially at ankle
- No significant muscle atrophy (disuse atrophy only; no denervation atrophy)
- Weakness in a pyramidal distribution - extensors weaker in arms, flexors weaker in legs
- Preservation of bilaterally-innervated movements - eyes, jaw, upper face, pharynx, larynx, diaphragm, abdomen spared (bilateral cortical innervation)
Important: Acute lesions (hyperacute stroke, spinal shock) initially present as flaccid paralysis with absent reflexes - spasticity and hyperreflexia develop over days to weeks.
- Adams and Victor's Principles of Neurology; Bradley and Daroff's Neurology
Causes of Hemiplegia
By Frequency (Adams and Victor's)
- Ischemic and hemorrhagic cerebrovascular disease - exceeds all others; most common cause
- Trauma (brain contusion, epidural hematoma, subdural hemorrhage) - second most common
- Brain tumors (primary or metastatic)
- Demyelinating disease (Multiple Sclerosis)
- Brain abscess
- Vascular complications of meningitis/encephalitis
- Migraine (hemiplegic migraine, migrainous infarction)
- Functional/psychogenic (conversion disorder, malingering)
Additional Causes by Setting
- Lacunar infarct (posterior limb of internal capsule or base of pons) - pure motor hemiplegia
- Alternating hemiplegia of childhood - rare; ATP1A3 mutation; attacks before age 18 months
- Todd (postictal) paralysis - transient, contralateral to seizure focus; lasts minutes to 36 hours
- Ictal paralysis - weakness during the seizure discharge itself (rare)
- Hemiplegic migraine (familial) - CACNA1A, ATP1A2, SCN1A mutations
Localization Clues: Crossed Brainstem Syndromes
Brainstem lesions produce ipsilateral CN palsy + contralateral hemiplegia ("alternating" or "crossed" hemiplegia):
| Syndrome | Level | Features |
|---|---|---|
| Weber syndrome | Midbrain (cerebral peduncle) | Ipsilateral CN III palsy (ptosis, mydriasis, "down and out") + contralateral hemiplegia |
| Millard-Gubler syndrome | Ventral pons | Ipsilateral CN VI (lateral rectus) + CN VII (peripheral facial) palsy + contralateral hemiplegia |
| Foville syndrome | Dorsal pons | Ipsilateral conjugate gaze palsy + CN VII + contralateral hemiplegia |
| Medial medullary (Dejerine) syndrome | Medulla (pyramid) | Ipsilateral CN XII palsy + contralateral hemiplegia (face spared) + contralateral proprioceptive loss |
Rule of thumb: cranial nerve palsies on the same side as the lesion with limb weakness on the opposite side = brainstem localization.
- Adams and Victor's; Localization in Clinical Neurology, 8e
Pure Motor Hemiplegia (Lacunar Stroke)
A lacunar infarct in the posterior limb of the internal capsule or base of pons (territory of lenticulostriate or pontine perforating arteries) causes:
- Complete contralateral hemiplegia (face, arm, leg equally affected)
- No cortical signs (no aphasia, no neglect, no visual field defect)
- No sensory loss
This pattern is highly characteristic and clinically important.
- Adams and Victor's Principles of Neurology
Cortical vs. Capsular vs. Brainstem Localization
| Feature | Cortex | Internal Capsule | Brainstem |
|---|---|---|---|
| Weakness distribution | Focal (face OR arm OR leg) | Equal arm, face, leg | Contralateral limbs + ipsilateral CN |
| Aphasia/neglect | Yes (dominant/non-dominant) | Rarely | No |
| CN palsies | No | No | Yes (ipsilateral) |
| Sensory loss | Cortical type (discriminative) | May occur | Variable |
| Visual field defect | Possible (optic radiations) | Rarely | Possible |
| Seizures | Yes | Rare | No |
- Bradley and Daroff's Neurology in Clinical Practice
Differential Diagnosis: Mimics of Hemiplegia
Migraine vs. TIA vs. Seizure
| Feature | Migraine | Stroke/TIA | Seizure |
|---|---|---|---|
| Onset | Gradual (marching) | Abrupt | Abrupt |
| Positive symptoms | Visual aura, scintillations | Rare | Jerking/stiffness common |
| Duration | 20-60 min | TIA: 5 min-1 hr | Minutes (postictal hours) |
| Headache | Yes (after deficit) | Hemorrhage only | Rare |
| Progression | Spreads (spreading depression) | Maximal at onset | Abrupt on/off |
Psychogenic (Functional) Hemiplegia
Clues pointing to functional weakness:
-
Give-way weakness (strength varies with effort/coaching)
-
Inconsistencies on exam (e.g., unable to dorsiflex foot but can walk on heels)
-
Hoover sign - patient supine: if a leg is truly paralyzed, the opposite heel should press down as the patient tries to lift it; absence of this downward pressure = Hoover sign positive for functional weakness
-
Paralysis with normal tone and reflexes
-
Obvious secondary gain
-
Bradley and Daroff's Neurology
Special Patterns
Brown-Séquard Syndrome (Spinal Cord)
- Lesion in cervical spinal cord
- Ipsilateral hemiplegia + loss of vibration/proprioception
- Contralateral loss of pain and temperature
- Face spared
Infantile Hemiplegia
- Developmental failure of affected limbs/skeleton on the hemiplegic side
- Usually from ischemic necrosis in utero or perinatally
- Does not occur if paralysis develops after puberty
Alternating Hemiplegia of Childhood
- Attacks of unilateral weakness before 18 months; may alternate sides
- Associated dyskinesias, oculomotor abnormalities (nystagmus)
- Deficits accumulate over years; linked to ATP1A3 mutations
Complications of Established Hemiplegia
- Spastic equinovarus deformity (foot drop)
- Shoulder subluxation and hemiplegic shoulder pain (common post-stroke)
- Deep vein thrombosis from immobility
- Pressure ulcers
- Depression and cognitive impairment
- Contractures from prolonged spasticity
- In childhood onset: limb length discrepancy, scoliosis
Rehabilitation
Multidisciplinary rehabilitation is the cornerstone of recovery. Recent evidence:
- A 2025 network meta-analysis (PMID 41204516) found that combined rehabilitation approaches (e.g., task-oriented training + neurostimulation) outperform single modalities for upper extremity function and ADLs in hemiplegic stroke patients
- A 2025 systematic review and meta-analysis (PMID 40022760) found virtual reality therapy significantly improves upper limb motor impairments post-stroke
- A 2025 systematic review (PMID 39745590) supports repetitive transcranial magnetic stimulation (rTMS) for hemiplegic shoulder pain
Key rehabilitation strategies include:
- Physiotherapy (task-oriented training, constraint-induced movement therapy)
- Occupational therapy (ADL retraining, splinting)
- Spasticity management (baclofen, botulinum toxin, tizanidine)
- Speech therapy (if associated aphasia/dysarthria)
- Virtual reality and robot-assisted therapy (emerging evidence)
Peripheral neuritis
Reading File
Finding Sources
Finding Sources
Searching PubMed
peripheral neuropathy etiology treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive, authoritative content. Let me compile the full answer.
Peripheral Neuritis (Peripheral Neuropathy)
Terminology
"Peripheral neuritis" is an older clinical term now largely replaced by peripheral neuropathy, which refers to any disorder affecting the peripheral nervous system - the sensory, motor, and autonomic nerves outside the brain and spinal cord. The term "neuritis" implies an inflammatory component (now reserved for truly inflammatory causes), while "neuropathy" is the broader, correct descriptor.
Anatomy & Fiber Types
Peripheral nerves contain three major fiber classes, each susceptible to injury in different ways:
| Fiber Type | Size | Function | Affected In |
|---|---|---|---|
| Large myelinated | Large | Motor, proprioception, vibration | CMT, CIDP, GBS |
| Small myelinated | Small | Pain, temperature (Aδ) | Diabetes (early), amyloid |
| Small unmyelinated (C fibers) | Smallest | Pain, temperature, autonomic | Small fiber neuropathy, diabetes |
Motor axons are typically large myelinated fibers conducting at ~50 m/s. The majority of neuropathies are predominantly sensory in nature.
- Harrison's Principles of Internal Medicine 22E
Pathological Mechanisms
There are four main pathological processes in peripheral nerves:
1. Wallerian Degeneration
- Follows focal nerve injury (compression, laceration, ischemia)
- Distal axon and myelin break down after axonal interruption
- EMG: loss of voluntary motor unit activity; CMAP amplitude falls from day 2, nadir by day 5-6
- SNAP loss delayed by 2-3 days further (nadir at day 10-11)
- Chromatolysis occurs in the cell body
- Regeneration from proximal stump at 2-3 mm/day; often incomplete
- Recovery depends on preservation of Schwann cell basal lamina tube
2. Axonal Degeneration ("Dying-Back" / Length-Dependent Polyneuropathy)
- The most common pathological reaction in peripheral nerve
- Distal axonal breakdown from metabolic derangement or vascular compromise (ischemia)
- Begins at the distal end of the nerve and works proximally
- Causes: systemic metabolic disorders (diabetes, uremia), toxins, vasculitis, inherited neuropathies
- Clinical result: symmetric distal sensory and motor loss, stocking-and-glove pattern; distal areflexia; distal muscle atrophy
3. Demyelinating Neuropathy (Myelinopathy)
- Primary damage to Schwann cells and myelin sheaths
- Nerve conduction velocity markedly slowed
- Causes: GBS, CIDP, CMT type I, leprosy, diphtheria
- Remyelination produces onion-bulb formation (seen histologically)
- Conduction block possible with focal demyelination
4. Neuronopathy / Ganglionopathy
-
Damage to the cell body of the neuron (dorsal root ganglion for sensory; anterior horn for motor)
-
Non-length-dependent; may affect arms > legs or asymmetrically
-
Causes: paraneoplastic (anti-Hu), cisplatin, pyridoxine (B6) toxicity, Sjögren syndrome, HIV
-
Bradley and Daroff's Neurology in Clinical Practice; Robbins Cotran & Kumar Pathologic Basis of Disease
Etiology - Classification
| Category | Examples |
|---|---|
| Nutritional/Metabolic | Diabetes mellitus (most common), uremia, thiamine (B1), B6, B12 deficiency |
| Toxic | Alcohol; drugs: vincristine, vinblastine, paclitaxel, cisplatin, oxaliplatin, bortezomib, colchicine, isoniazid; heavy metals: lead, arsenic, mercury, aluminum; acrylamide |
| Inflammatory/Autoimmune | GBS (acute demyelinating), CIDP (chronic demyelinating), lupus, Sjögren syndrome, mixed connective tissue disease |
| Vasculopathic/Infiltrative | Vasculitis, amyloidosis, sarcoidosis, lymphoma |
| Infectious | Leprosy (most common worldwide), herpes zoster, HIV, Lyme disease, CMV |
| Hereditary | Charcot-Marie-Tooth (CMT types I, II, X-linked), HSAN, hereditary amyloid neuropathy |
| Paraneoplastic | Small cell lung cancer (anti-Hu), others |
| Idiopathic/Cryptogenic | ~50% of cases have no identifiable cause (CSPN - cryptogenic sensory/sensorimotor polyneuropathy) |
In developed countries: diabetes and alcoholism are the most common causes in adults.
Worldwide: leprosy is the most common preventable cause.
- Robbins & Kumar Basic Pathology; Textbook of Family Medicine 9e
Clinical Patterns (Harrison's 10-Pattern Classification)
| Pattern | Features | Key Diagnoses |
|---|---|---|
| 1 | Symmetric proximal + distal weakness | GBS, CIDP |
| 2 | Symmetric distal sensory loss ± distal weakness | Diabetes, alcoholism, drugs, toxins, idiopathic |
| 3 | Asymmetric distal weakness + sensory loss (multiple nerves) | Vasculitis, leprosy, Lyme, HIV, multifocal CIDP |
| 4 | Asymmetric proximal + distal weakness + sensory loss | Polyradiculopathy, plexopathy (diabetic amyotrophy) |
| 5 | Asymmetric distal weakness without sensory loss | Motor neuron disease, multifocal motor neuropathy |
| 6 | Symmetric sensory loss + distal areflexia + UMN signs | B12/B6/copper deficiency, adrenomyeloneuropathy |
| 7 | Symmetric weakness without sensory loss | SMA, hereditary motor neuropathy |
| 9 | Asymmetric proprioceptive loss without weakness | Sensory neuronopathy: paraneoplastic, cisplatin, B6 toxicity, HIV |
| 10 | Autonomic dysfunction | Diabetes, amyloidosis, GBS, porphyria, HSAN |
- Harrison's Principles of Internal Medicine 22E
Key Specific Neuropathies
Diabetic Peripheral Neuropathy
- Most common cause of peripheral neuropathy globally
- Up to 80% of patients with DM >15 years have evidence of neuropathy
- Distal symmetric sensorimotor polyneuropathy: commonest form; sensory axons > motor axons; paresthesias, numbness; features of both axonal and demyelinating injury
- Autonomic neuropathy: orthostatic hypotension, bowel/bladder/sexual dysfunction
- Lumbosacral radiculopathy (diabetic amyotrophy): asymmetric pain, weakness, atrophy
- Pathogenesis: AGE accumulation, reactive oxygen species, microvascular changes, altered axonal metabolism
- Treatment: strict glycemic control is the best therapy
Guillain-Barré Syndrome (GBS)
- Rapidly progressive acute demyelinating polyneuropathy
- Ascending weakness; progresses over ~2 weeks, nadir by 4 weeks
- One of the most common life-threatening peripheral nerve diseases
- ~2/3 triggered by preceding infection: Campylobacter jejuni, EBV, CMV, Zika virus
- Mechanism: molecular mimicry - microbial antigens cross-react with nerve sheath antigens
- Treatment: IV immunoglobulin (IVIg) or plasmapheresis; ventilatory support if needed
Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)
- Chronic (>8 weeks) acquired demyelinating polyneuropathy
- Symmetric proximal + distal weakness; sensory involvement
- Treatment: IVIg, corticosteroids, plasmapheresis
Alcoholic Peripheral Neuropathy
- Combination of direct toxic effect of ethanol + thiamine (B1) deficiency
- Distal symmetric, predominantly sensory; painful paresthesias common
- Stocking-and-glove distribution
Thiamine Deficiency (Beriberi/Peripheral Neuritis)
- "Dry beriberi" - symmetric peripheral neuropathy of motor and sensory systems, diminished reflexes
- "Wet beriberi" - adds high-output heart failure and edema
- Wernicke encephalopathy (acute) and Korsakoff psychosis (chronic) are CNS manifestations
- Harrison's Principles of Internal Medicine; Harper's Illustrated Biochemistry
Charcot-Marie-Tooth Disease (CMT)
- Most common hereditary peripheral neuropathy
- CMT1 (demyelinating): presents 1st-3rd decade; foot drop, high arches, "inverted champagne bottle legs"; slowed NCV (20-25 m/s); onion bulbs on biopsy
- CMT1A: most common (70%) - chromosome 17p duplication, PMP-22 gene triplication
- CMT1B: MPZ (myelin protein zero) mutation
- CMT2 (axonal): presents 2nd decade; normal or near-normal NCVs
- No disease-modifying therapy; supportive and rehabilitative management
Investigations
-
Nerve Conduction Studies (NCS) / Electromyography (EMG)
- Axonal neuropathy: reduced CMAP and SNAP amplitudes; normal or mildly reduced NCV
- Demyelinating neuropathy: markedly slow NCV; conduction block; prolonged distal latencies
- EMG: fibrillation potentials, reduced recruitment (axonal loss); normal or mild changes (demyelinating)
-
Blood tests: FBS/HbA1c, renal function, LFTs, B12, thiamine, TSH, serum/urine protein electrophoresis, ANA, ANCA, anti-Ro/La (Sjögren), paraneoplastic antibodies (anti-Hu), heavy metals
-
Nerve biopsy (sural nerve): for vasculitis, amyloidosis, leprosy, CIDP; axonal loss vs. demyelination; onion bulbs (CMT1)
-
Skin biopsy (punch biopsy): intraepidermal nerve fiber density - used for small fiber neuropathy
-
Genetic testing: for suspected CMT and other hereditary neuropathies
-
Lumbar puncture: GBS - albuminocytologic dissociation (high protein, normal cell count)
Symptoms & Signs
Sensory symptoms:
- Numbness, tingling, paresthesias (pins and needles)
- Burning pain (especially small fiber neuropathy)
- Loss of proprioception and vibration (large fiber)
- Positive Romberg sign; sensory ataxia
Motor signs:
- Distal weakness (foot drop, wrist drop)
- Muscle atrophy (distal)
- Loss of deep tendon reflexes (areflexia/hyporeflexia) - particularly ankle jerks first
Autonomic features (if autonomic nerves involved):
- Orthostatic hypotension
- Anhidrosis or hyperhidrosis
- Gastroparesis, constipation, diarrhea
- Urinary retention or incontinence
- Erectile dysfunction
Treatment
Treat the Underlying Cause
- Diabetes: strict glycemic control
- Nutritional: replace thiamine, B12, B6 as appropriate
- Toxic: remove offending drug or toxin
- GBS/CIDP: IVIg or plasmapheresis
- Vasculitis: immunosuppression (corticosteroids, cyclophosphamide)
- Leprosy: WHO multidrug therapy (rifampicin, dapsone, clofazimine)
Neuropathic Pain Management
First-line agents (FDA-approved or widely used):
- Pregabalin and duloxetine - FDA approved for diabetic peripheral neuropathy pain
- Gabapentin - widely used, effective
- Tricyclic antidepressants (amitriptyline, nortriptyline)
- SNRIs (venlafaxine)
- Tramadol - effective in two multicenter trials; use if refractory to first-line
- Opioids - only in consultation with pain specialist
- NSAIDs are generally not effective for neuropathic pain
- Topical capsaicin - possibly effective
Rehabilitative Care
-
Foot care education (especially in diabetes)
-
Podiatry referral for structural foot abnormalities
-
Orthotic devices (ankle-foot orthoses for foot drop)
-
Physical and occupational therapy
-
Screening for peripheral arterial disease (ankle-brachial index)
-
Symptom to Diagnosis, 4th Ed.; Harrison's Principles of Internal Medicine 22E
Recent Evidence (PubMed 2024-2026)
- A 2025 Lancet Neurology systematic review and meta-analysis (PMID 40252663) provides updated evidence comparing pharmacotherapy and non-invasive neuromodulation (TMS, tDCS, TENS) for neuropathic pain - both approaches have efficacy, supporting their combination
- The first-line pharmacological agents (gabapentinoids, SNRIs, TCAs) remain consistent with prior guidelines
Burgers disease
Reading File
Finding Sources
Searching PubMed
thromboangiitis obliterans Buerger disease
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compose the complete answer.
Buerger's Disease (Thromboangiitis Obliterans - TAO)
Definition
Buerger's disease, formally known as thromboangiitis obliterans (TAO), is a progressive, non-atherosclerotic, segmental, occlusive inflammatory disease affecting the small- and medium-sized arteries, veins, and nerves of the upper and lower extremities. First described by Leo Buerger in 1908 from 11 amputated limbs.
The cause remains unknown, but tobacco use is essential to both the diagnosis and the progression of the disease.
- Schwartz's Principles of Surgery 11e; Robbins & Kumar Basic Pathology
Epidemiology
- Predominantly affects young male smokers (age 20-50 years, typically onset before 40-45 years)
- Women now account for nearly 20% of cases, likely reflecting increased tobacco use among women
- Worldwide distribution: highest prevalence in Eastern Europe, Mediterranean, and Asian countries
- Incidence in the US: ~20 per 100,000; accounts for <1% of severe limb ischemia cases in North America
- In young adults with lower limb ischemia at the Mayo Clinic (1953-1981), Buerger's disease was diagnosed in 24%
Pathogenesis
The exact etiology is unknown, but several mechanisms are implicated:
- Tobacco (cigarettes, cigars, smokeless/chewing tobacco, snuff) - all forms are implicated
- Endothelial dysfunction: reduced endothelium-dependent vasodilation + release of prothrombotic substances
- Direct endothelial cell toxicity from tobacco components
- Immune/hypersensitivity response: most patients are hypersensitive to tobacco extracts; tobacco antigens may modify vessel wall components and trigger an immune response
- Genetic predisposition: association with certain HLA haplotypes
Key point: Unlike atherosclerosis, there is no association with diabetes, hyperlipidemia, or hypertension (these are exclusion criteria).
- Robbins & Kumar Basic Pathology
Pathology / Morphology
The histological features are distinctive and differ from other vasculitides in that the internal elastic lamina and vessel wall architecture are largely preserved:
Acute/early phase:
- Sharply segmental acute and chronic vasculitis of small- and medium-sized vessels
- Luminal thrombosis with a mixed inflammatory infiltrate
- Small microabscesses (sterile), occasionally rimmed by granulomatous inflammation within the thrombus
- Polymorphonuclear leukocyte aggregation and multinucleated giant cells
Chronic/late phase:
- Decrease in hypercellularity
- Recanalization of the vessel lumen
- Inflammation extends into adjacent veins and nerves (this extension into nerves is rare in other vasculitides and explains the severe pain)
- End-stage: organized thrombus + blood vessel fibrosis; artery and adjacent structures encased in fibrous tissue
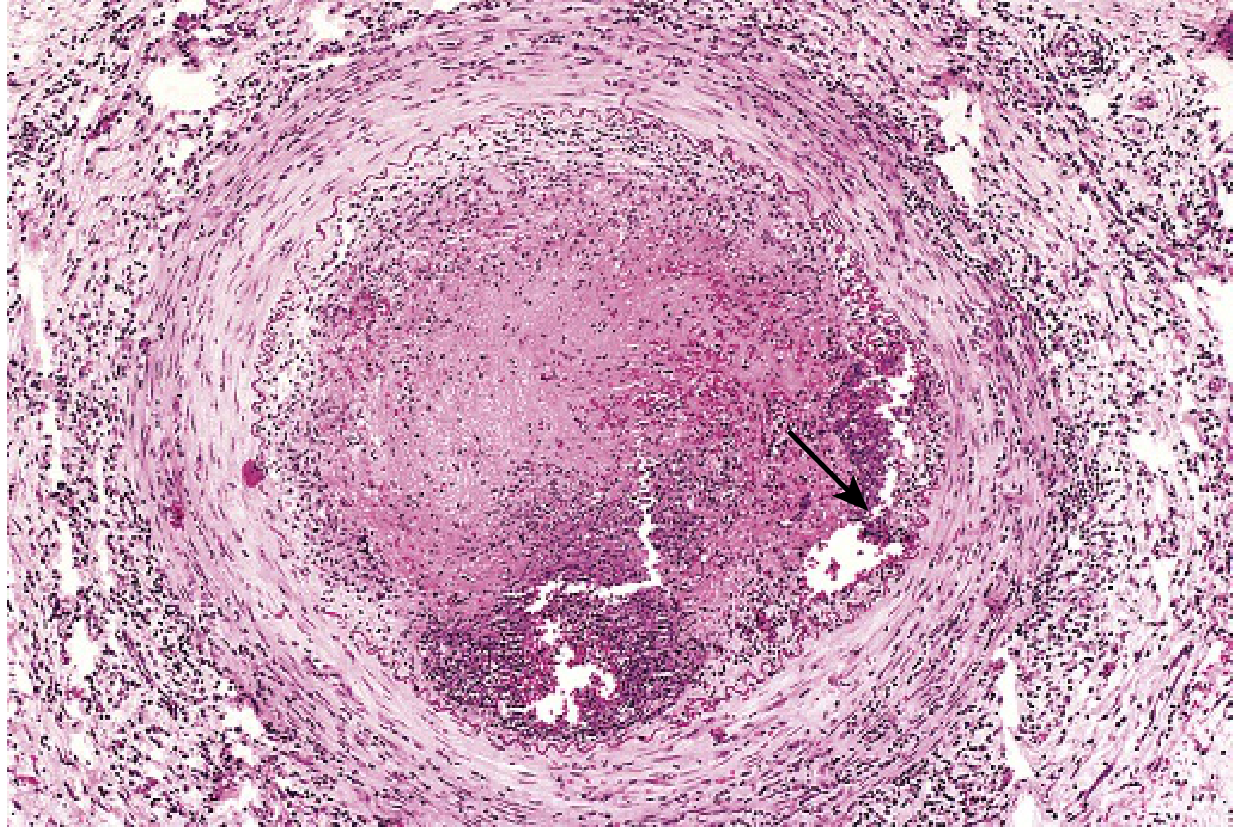
Histology of Buerger's disease: thrombus occupies the lumen with a sterile microabscess (arrow); the vessel wall shows leukocytic infiltration with preserved architecture. (Robbins & Kumar Basic Pathology)
- Schwartz's Principles of Surgery 11e; Robbins & Kumar Basic Pathology
Clinical Features
The disease typically starts in the distal small arteries and veins of the hands and feet and progresses proximally. At least 2 or more extremities are always involved; 40% of cases affect all four limbs.
Symptoms in order of progression:
| Stage | Manifestations |
|---|---|
| Early | Cold sensitivity, Raynaud phenomenon (~50%), instep/foot claudication, superficial migratory thrombophlebitis |
| Intermediate | Calf and leg claudication, hand claudication, rest pain |
| Late | Ischemic ulcerations of toes, fingers, and feet; gangrene |
Key clinical hallmarks:
- Instep/foot claudication - pain in the arch of the foot on exertion (caused by infrapopliteal arterial occlusion) - distinguishes TAO from atherosclerotic PAD (which typically causes calf claudication)
- Superficial migratory thrombophlebitis (phlebitis migrans) - painful tender nodules over peripheral veins; occurs in up to 16% and indicates systemic inflammatory response; often an early feature
- Raynaud phenomenon - triphasic color response (white-blue-red) to cold in ~50% of patients
- Intense rubor of the affected extremity, especially with dependency
- Foot pulses absent in the presence of normal femoral and popliteal pulses
- Severe rest pain (due to neural involvement - the extension of inflammation into adjacent nerves is unique to TAO)
- Upper extremity: digital arteries more involved than radial or ulnar arteries; fingertip ulcers
Diagnostic Criteria (Clinical)
TAO is a diagnosis of exclusion - no laboratory test confirms it. The following criteria are used:
- Age < 45-50 years at onset
- History of tobacco use (essential)
- Distal extremity ischemia in two or more limbs
- Angiographic findings suggestive of TAO
- Absence of atherosclerotic risk factors other than smoking (no DM, no hyperlipidemia, no hypertension, no hypercoagulable state)
Investigations
Laboratory (to exclude other diagnoses):
- CBC with differential, BMP, LFTs, fasting glucose, urinalysis
- ESR, CRP (usually normal or mildly elevated in TAO)
- Hypercoagulability screen + antiphospholipid antibodies
- ANA, rheumatoid factor, complement, anti-Scl-70, anti-centromere (CREST)
- All expected to be negative/normal in true TAO
Vascular studies:
- Ankle-brachial index (ABI) - reduced; segmental pressures; arterial waveform analysis
- Allen test - positive in a young smoker with distal upper limb ischemia is suggestive
- Echocardiography + CT/MR angiography - to exclude proximal embolic sources
Angiography (gold standard imaging):
Characteristic angiographic findings:
- Disease confined to the distal circulation (infrapopliteal; distal to brachial artery in upper limb)
- Segmental occlusions with "skip" lesions
- "Corkscrew" collaterals - pathognomonic appearance of extensive collateralization
- No atherosclerotic changes (smooth vessel wall between lesions)
- All four limbs should be imaged even if only one is symptomatic
Biopsy:
- Rarely necessary; reserved for atypical presentations
- The only means of definitive diagnosis
- Shows the characteristic segmental inflammatory thrombosis with microabscesses
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Atherosclerotic PAD | Age >50, risk factors (DM, HTN, hyperlipidemia), proximal disease, calcified vessels |
| Autoimmune (SLE, scleroderma) | Positive ANA, anti-Scl-70; young women; systemic features |
| Embolic disease | Proximal source on echo/CT; unilateral; abrupt onset |
| Hypercoagulable states | Positive thrombophilia screen |
| Vasculitis (PAN, GPA) | Systemic features, ANCA positivity, visceral involvement |
Treatment
First-line and Only Definitive Treatment: Complete Tobacco Cessation
This is the single most important intervention. All tobacco products must be stopped completely.
- Patients who quit: benign clinical course, disease remission, impressive amputation avoidance
- Patients who continue smoking: 67% limb loss vs 35% in those who quit
- No disease progression with tissue loss after tobacco discontinuation (Oregon Health Sciences Center experience)
- Established arterial occlusions do not reverse after cessation, but further progression is halted
Medical Therapy (adjunctive):
| Agent | Role |
|---|---|
| Prostacyclin (iloprost) and analogues | Most evidence; improves rest pain and ulcer healing |
| Aspirin | Antiplatelet; routine use |
| PDE5 inhibitors (sildenafil) | Vasodilatory; some evidence |
| Bosentan (dual endothelin-1 receptor antagonist) | Vasodilation |
| Serotonin blockers / sarpogrelate | Antiplatelet/vasodilatory |
| Intraarterial streptokinase (low-dose) | Selected acute cases |
| Cyclophosphamide | Refractory inflammatory cases |
| Prostaglandin E1 (IV or IA) | Rest pain and ulcer healing |
| Guanethidine sympathetic blocks | Pain relief |
| Intramuscular VEGF | Experimental angiogenesis |
Surgical Options:
| Procedure | Indication |
|---|---|
| Sympathectomy (lumbar or thoracic) | Rest pain, cutaneous ulcers not responding to medical therapy |
| Arterial reconstruction / bypass | Limited by lack of suitable distal target vessels and poor conduit quality (coexisting thrombophlebitis damages vein conduits) |
| Endovascular (angioplasty) | Individual tibial/foot vessel obstructions in selected cases |
| Amputation | End-stage disease with uncontrollable gangrene/infection |
Key surgical limitation: The distal nature of the disease means there is often no acceptable target vessel for bypass. Autogenous vein conduits are also limited due to coexisting migratory thrombophlebitis damaging the veins.
- 31% limb loss over 15 years reported even with surgical management (Mayo series)
- Current Surgical Therapy 14e; Schwartz's Principles of Surgery 11e; Rosen's Emergency Medicine
Prognosis
- Patients who completely abstain from tobacco: disease arrests, excellent prognosis, most avoid amputation
- Patients who continue smoking: relentless progression with alternating exacerbations, severe rest pain, tissue loss, and eventual amputation
- Rare large-vessel involvement (coronary, cerebral, mesenteric arteries) carries poor prognosis - mesenteric TAO warrants prompt surgery for bowel ischemia
Recent Evidence (PubMed 2024-2026)
- A 2025 systematic review and meta-analysis (PMID 39847853) on treatment options for Buerger's disease confirms that smoking cessation remains the cornerstone, with prostanoids (iloprost) showing the best evidence for limb salvage among medical therapies
- A 2026 systematic review and meta-analysis (PMID 41887323) comparing open surgical vs. endovascular revascularization in TAO with chronic limb-threatening ischemia found that neither approach shows clear superiority, reinforcing that smoking cessation is the primary determinant of outcomes
- A 2024 Mendelian randomization study (PMID 38788766) identified causal relationships between specific circulating inflammatory proteins and TAO, supporting the immune/inflammatory pathogenesis hypothesis
This is a shared conversation. Sign in to Orris to start your own chat.