I now have extensive, high-quality data from Harrison's 22E, Washington Manual, Rosen's EM, Goldman-Cecil, and GOLD 2026. Let me compile the comprehensive answer.
Acute Exacerbations of COPD (AECOPD) - Management
Definition
An AECOPD is an
acute event (symptoms worsening over a few days, up to 14 days) characterized by increased dyspnea and/or cough and sputum production that is beyond normal day-to-day variation and requires a change in management. It may be accompanied by tachypnea and/or tachycardia. The
GOLD 2026 Pocket Guide notes exacerbations are often driven by increased local and systemic inflammation from airway infection or pollution.
Precipitating Causes
| Category | Examples |
|---|
| Viral infections | Rhinovirus, influenza, RSV (>50% of exacerbations per PCR studies) |
| Bacterial infections | H. influenzae, S. pneumoniae, M. catarrhalis, new bacterial strains |
| Environmental | Air pollution, allergens, temperature changes |
| Other | Pulmonary embolism, medication non-adherence |
| Unknown | ~25–30% of cases have no identifiable precipitant |
Differential Diagnosis
Always exclude mimics before labeling as AECOPD:
-
Pneumonia
-
Pulmonary embolism (incidence is increased in AECOPD)
-
Acute decompensated heart failure
-
Pneumothorax
-
Cardiac ischemia
-
Pleural effusion
-
Large airway tumor
-
Washington Manual of Medical Therapeutics, p. 319
Severity Classification (GOLD / Rome Proposal)
| Severity | Features |
|---|
| Mild | Treated with SABAs alone; no change in other medications |
| Moderate | Treated with SABAs + antibiotics and/or systemic corticosteroids |
| Severe | Requires hospitalization or ER visit; may have acute respiratory failure |
Initial Assessment
History
- Degree and change in dyspnea (activities of daily living)
- Fever, sputum character change, wheezing, GI symptoms
- Frequency and severity of prior exacerbations (prior hospitalization = biggest risk factor for re-hospitalization)
- Comorbidities (heart disease, diabetes)
Physical Examination
Focus on:
- Tachycardia, tachypnea
- Use of accessory muscles, intercostal retractions
- Ability to speak in complete sentences
- Mental status (confusion/somnolence suggests hypercarbia)
- Asymmetric chest findings (pneumothorax), paradoxical abdominal wall movement
- Signs of right or left heart failure
Investigations
| Test | Indication |
|---|
| Pulse oximetry | All patients |
| ABG | Moderate-severe distress, suspected hypercarbia (PCO₂ >45 mmHg has key therapeutic implications), mental status changes |
| CXR | Abnormal in ~15-25%; always order if chest pain, leukocytosis, history of heart disease |
| ECG | Assess for cardiac ischemia, arrhythmia |
| CBC, BMP | Screen for anemia, metabolic acidosis, hyperglycemia |
| BNP/NT-proBNP | If left heart failure suspected |
| Troponin | If myocardial ischemia is a concern |
| D-dimer | Only if PE is suspected after appropriate pre-test probability risk stratification |
| Sputum culture | Generally not indicated in routine exacerbations |
- Harrison's 22E, pp. 2302-2303; Rosen's Emergency Medicine, p. 2560
Indications for Hospitalization
-
Significant increase in symptom severity
-
Severe underlying COPD (e.g., FEV₁ very low at baseline)
-
Respiratory acidosis / hypercarbia
-
New or worsening hypoxemia
-
Significant comorbidities (heart failure, arrhythmia)
-
Failure to respond to initial outpatient/ED treatment
-
Insufficient home support or inability to manage at home
-
Diagnostic uncertainty
-
Washington Manual, p. 320; Goldman-Cecil Medicine, p. 3148
Indications for ICU Admission
- Need for invasive mechanical ventilation
- Hemodynamic instability
- Severe dyspnea not responding to therapy
- Altered mental status
- Persistent or worsening hypoxemia, hypercapnia, or respiratory acidosis despite supplemental O₂ and NIV
Pharmacological Management
1. Bronchodilators (First-Line)
Short-acting beta-2 agonists (SABAs) are first-line:
| Drug | MDI Dose | Nebulizer Dose |
|---|
| Albuterol (Salbutamol) | 2-4 puffs q1-4h | 2.5 mg q1-4h (hourly x 1-3h, then q2-4h) |
Short-acting anticholinergics (SAACs) are added if SABA response is inadequate:
| Drug | MDI Dose | Nebulizer Dose |
|---|
| Ipratropium | 2 puffs q4h | 0.5 mg q4h |
-
In the emergency setting, nebulizers are preferred over MDIs requiring complex technique
-
Use air-driven nebulizers (not oxygen-driven) when possible
-
Continuous nebulization is NOT indicated
-
Methylxanthines (theophylline) are not recommended due to poor side-effect profile without added benefit
-
Washington Manual, p. 320; Rosen's EM, p. 2574; GOLD 2026
2. Systemic Corticosteroids
Recommended for moderate and severe exacerbations:
-
Prednisone 40 mg/day orally for 5 days (5-day courses are as effective as longer courses)
-
Parenteral route (methylprednisolone) only if patient cannot tolerate oral medication
-
Benefits: decreased recovery time, improved oxygenation, improved FEV₁, shorter hospital stay
-
Oral and parenteral bioavailability are similar - prefer oral when tolerated
-
Rosen's EM, p. 2579; GOLD 2026
3. Antibiotics
Indications for antibiotics (GOLD 2026 / Anthonisen criteria):
- Increased dyspnea + increased sputum volume + increased sputum purulence (all three = strongest indication)
- Patients requiring NIV or mechanical ventilation (clear mortality benefit in these)
- CRP-guided or procalcitonin-guided prescribing can reduce unnecessary antibiotic use in non-critically ill patients
Antibiotic duration: 5 days
| Patient Profile | Pathogens | Antibiotic Choice |
|---|
| No risk factors for poor outcome or resistant organism | H. influenzae, S. pneumoniae, M. catarrhalis | Macrolide, 2nd/3rd-gen cephalosporin, doxycycline, TMP/SMX |
| Risk factors present (severe COPD, recent hospitalization, prior Pseudomonas colonization) | Above + gram-negative rods including Pseudomonas | Antipseudomonal fluoroquinolone (e.g., levofloxacin 750 mg/day x 7-10d) or antipseudomonal beta-lactam |
Note: In critically ill patients on ICU, PCT-guided antibiotic therapy was associated with worse 3-month mortality - do NOT withhold antibiotics based on PCT in the ICU.
- Washington Manual, p. 320; Goldman-Cecil, p. 3150; Rosen's EM, p. 2582-2584
Oxygen Therapy
- Target SpO₂: 88-92% (controlled oxygen therapy to avoid hypercapnic drive suppression)
- High-flow nasal therapy (HFNT) is increasingly used for hypoxemic AECOPD
- Avoid high-concentration uncontrolled oxygen
Ventilatory Support
Non-Invasive Ventilation (NIV) - First-Line for Respiratory Failure
NIV (BiPAP/BPAP) is the preferred initial mode of ventilatory support in AECOPD with acute respiratory failure when no contraindications exist.
Indications for NIV:
- Severe dyspnea with increased work of breathing
- Moderate-to-severe respiratory acidosis (pH <7.35) + hypercapnia (PCO₂ >45 mmHg)
- Persistent hypoxemia despite supplemental oxygen
Benefits of NIV in AECOPD:
-
Decreased respiratory rate
-
Increased tidal volume and minute ventilation
-
Reduced need for endotracheal intubation
-
Decreased in-hospital mortality
-
Shorter ICU and hospital length of stay
-
Mechanism: improved alveolar ventilation and respiratory mechanics
-
Fishman's Pulmonary Diseases, p. 2630; Roberts and Hedges' Clinical Procedures, p. 231; Murray & Nadel's Respiratory Medicine
Key point: NIV must be initiated early alongside standard medical therapy. Late initiation (after medical treatment failure) eliminates the survival and intubation-reduction benefits.
Contraindications to NIV
- Respiratory or cardiac arrest
- Hemodynamic instability
- Uncooperative or agitated patient
- High aspiration risk
- Inability to protect airway
- Recent upper airway/GI surgery
Invasive Mechanical Ventilation
Indicated when NIV fails or for:
-
Respiratory arrest
-
Severe respiratory failure not responding to NIV
-
Decreased consciousness / significant agitation
-
Hemodynamic instability
-
Massive aspiration
-
Persistent inability to clear secretions
-
Harrison's 22E, p. 2303; Tintinalli's EM, p. 1745
Discharge Criteria and Follow-Up
GOLD 2026 discharge criteria:
- Patient on maintenance therapy every 4 hours or less
- Walking stable (patient ambulatory)
- Eating, sleeping not disturbed by dyspnea
- Clinically stable for 12-24 hours
- ABG stable for 12-24 hours
- Patient/family understands medication use
Post-exacerbation management:
- Initiate/optimize long-acting bronchodilators (LABDs) as soon as possible
- If ≥1 moderate/severe exacerbation and elevated blood eosinophil count: add ICS to dual bronchodilator regimen at discharge
- Full recovery takes 4-6 weeks - some patients never return to pre-exacerbation baseline
- Review COPD management plan and comorbidities
- Implement exacerbation prevention strategies (vaccination, smoking cessation, pulmonary rehabilitation)
Prevention of Future Exacerbations
| Strategy | Evidence |
|---|
| LAMA +/- LABA (triple therapy LAMA/LABA/ICS for high-risk) | First-line maintenance |
| Smoking cessation | Most important modifiable factor |
| Pneumococcal + annual influenza + COVID-19 vaccination | Reduces infective triggers |
| Pulmonary rehabilitation | Reduces re-hospitalization |
| Roflumilast (PDE4 inhibitor) | For frequent exacerbators with chronic bronchitis |
| Azithromycin (long-term) | Selected patients with recurrent exacerbations |
| Mepolizumab / Dupilumab | For eosinophilic COPD phenotype (GOLD 2025/2026) |
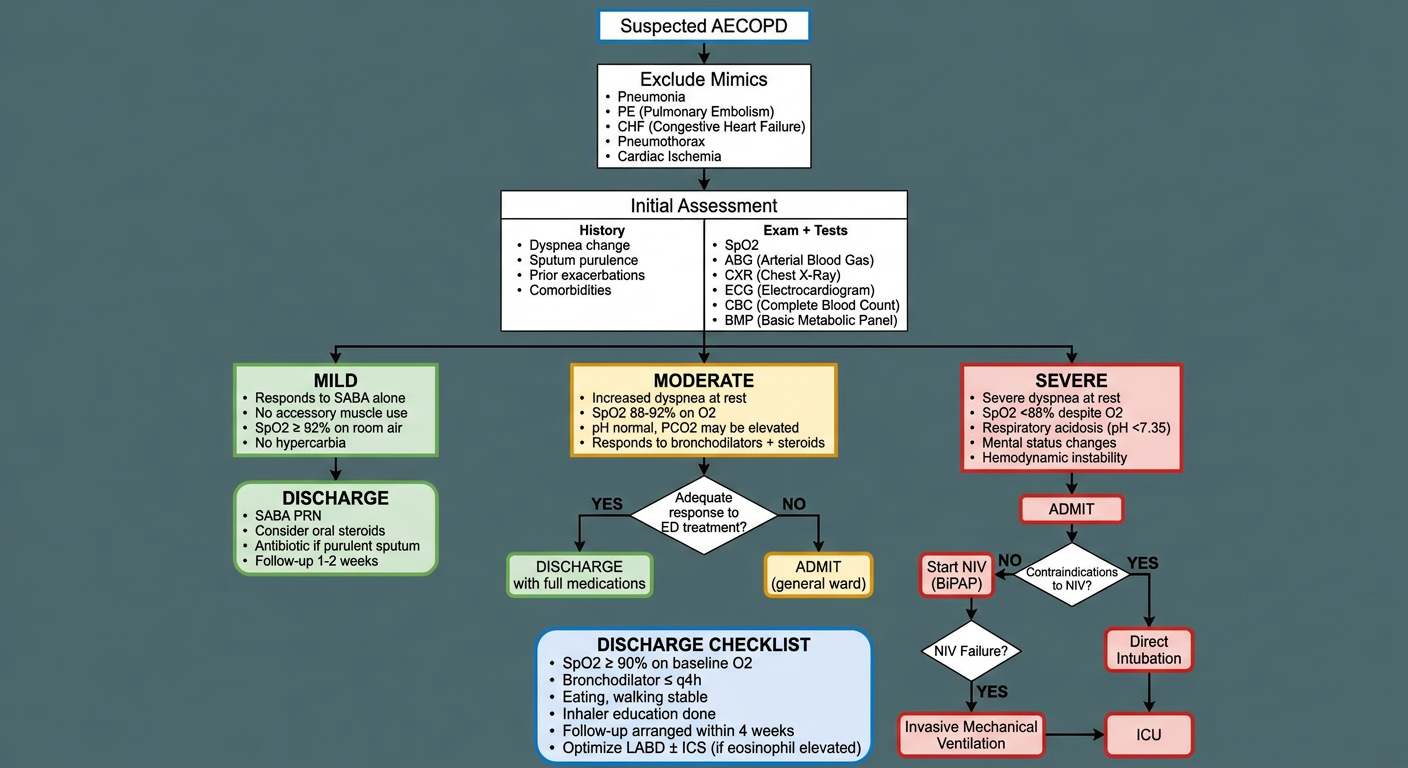
Summary Algorithm
AECOPD suspected
↓
Exclude mimics (PE, pneumonia, CHF, pneumothorax)
↓
Assess severity → Mild / Moderate / Severe
↓
All patients: SABA ± SAAC bronchodilators
Moderate/Severe: + systemic steroids (prednisone 40mg x 5d)
Purulent sputum/infection signs: + antibiotics x 5d
↓
Hypoxemia → controlled O₂ (SpO₂ 88-92%)
↓
Respiratory acidosis / increased WOB → NIV (BiPAP)
↓
NIV failure / contraindications → invasive MV
↓
Discharge with LABD optimization, follow-up in 1-4 weeks
Sources: Harrison's Principles of Internal Medicine 22E (2025) | The Washington Manual of Medical Therapeutics | Rosen's Emergency Medicine | Goldman-Cecil Medicine | Fishman's Pulmonary Diseases |
GOLD 2026 Pocket Guide