There is dilated tortous vein in anterior aspect of leg and also posterior aspect of leg which vein is involved bailey and love surgery
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive answer based on standard surgical anatomy as covered in major surgical textbooks (including the content referenced in Bailey & Love's Surgery context):
Varicose Veins: Anterior vs. Posterior Leg
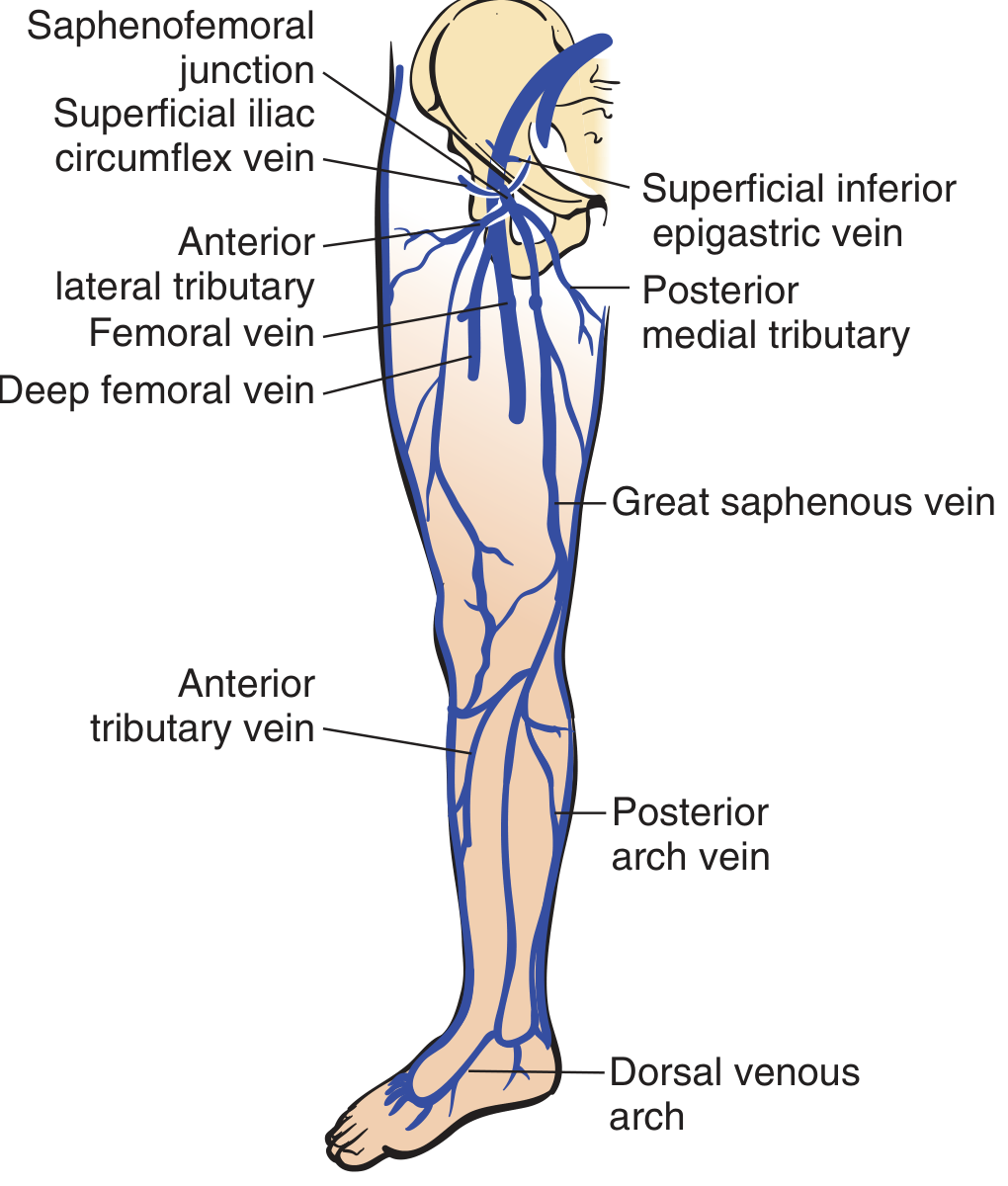
Anterior Aspect of the Leg → Great Saphenous Vein (GSV)
The great saphenous vein (long saphenous vein) is the principal vein responsible for varicosities on the anterior and anteromedial aspect of the leg.
- It originates from the dorsal venous arch of the foot
- Ascends along the anteromedial surface of the leg and thigh
- Drains into the femoral vein at the saphenofemoral junction (saphena varix) just below the inguinal ligament
- Its tributaries include the anterior tributary vein (seen on the anterior calf), the posterior arch vein (vein of Michelangelo/Leonardus), and the posterior medial tributary
Incompetence occurs at:
- The saphenofemoral junction (most common)
- Mid-thigh perforators between the GSV and femoral vein
- Calf perforators (Cockett's perforators) — 5, 10, and 15 cm above the medial malleolus
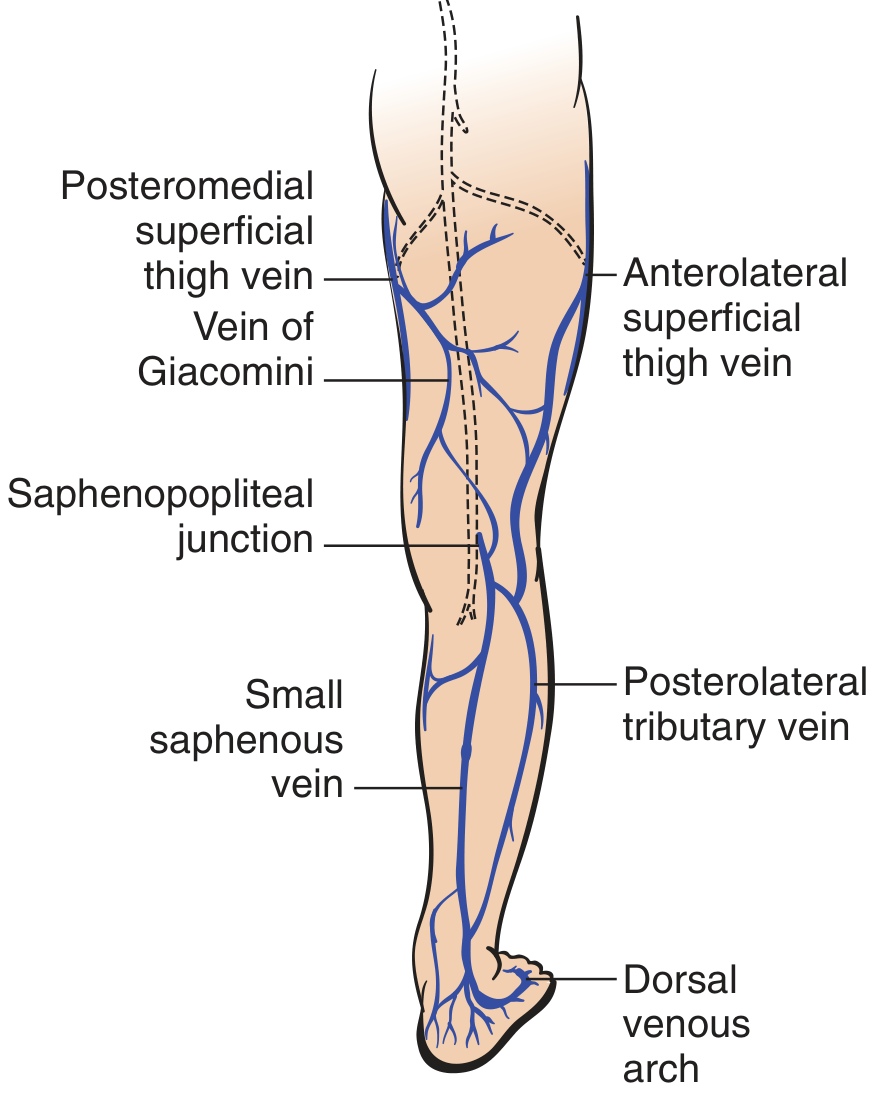
Posterior Aspect of the Leg → Small Saphenous Vein (SSV)
The small saphenous vein (short saphenous vein) is the principal vein responsible for varicosities on the posterior and posterolateral aspect of the leg.
- Originates from the dorsal venous arch at the posterolateral ankle (intimately associated with the sural nerve)
- Runs up the back of the leg in the midline
- Penetrates the deep fascia in the popliteal fossa and drains into the popliteal vein at the saphenopopliteal junction
- Connected to the GSV system via the vein of Giacomini (posteromedial thigh vein)
Incompetence occurs at:
- The saphenopopliteal junction — produces posterior/posterolateral calf varicosities
Summary Table
| Location of Varicosities | Vein Involved | Junction Site |
|---|---|---|
| Anterior / anteromedial leg | Great Saphenous Vein (GSV) | Saphenofemoral junction (groin) |
| Posterior / posterolateral leg | Small Saphenous Vein (SSV) | Saphenopopliteal junction (popliteal fossa) |
Clinical Relevance (Bailey & Love context)
When both anterior and posterior varicosities are present simultaneously, it indicates dual incompetence — both the saphenofemoral and saphenopopliteal junctions are affected. This is assessed clinically using the tourniquet test (Trendelenburg test):
- Tourniquet at upper thigh → controls GSV filling → tests saphenofemoral junction
- Tourniquet below knee → controls SSV filling → tests saphenopopliteal junction
Surgical treatment involves:
- GSV — ligation at the saphenofemoral junction + stripping
- SSV — ligation at the saphenopopliteal junction (care must be taken to avoid the common fibular/peroneal nerve and sural nerve in the popliteal fossa)
— Gray's Anatomy for Students; Pfenninger & Fowler's Procedures for Primary Care
Then is it both sshort and long saphenous vain incompetance what about perforators
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Excellent — here is the complete picture:
Both GSV + SSV Incompetence + Perforators
Yes — Dual Incompetence
When varicosities are present on both anterior and posterior aspects of the leg simultaneously, it indicates:
| System | Incompetent Junction |
|---|---|
| Great Saphenous Vein (GSV) | Saphenofemoral junction (groin) |
| Small Saphenous Vein (SSV) | Saphenopopliteal junction (popliteal fossa) |
The Role of Perforating Veins
Perforating veins (perforators) connect the superficial system → deep system. Their valves normally allow one-way flow inward (superficial to deep). When they become incompetent, blood flows in reverse — from deep to superficial — causing venous hypertension and worsening varicosities.
Clinically Important Perforators Associated with GSV
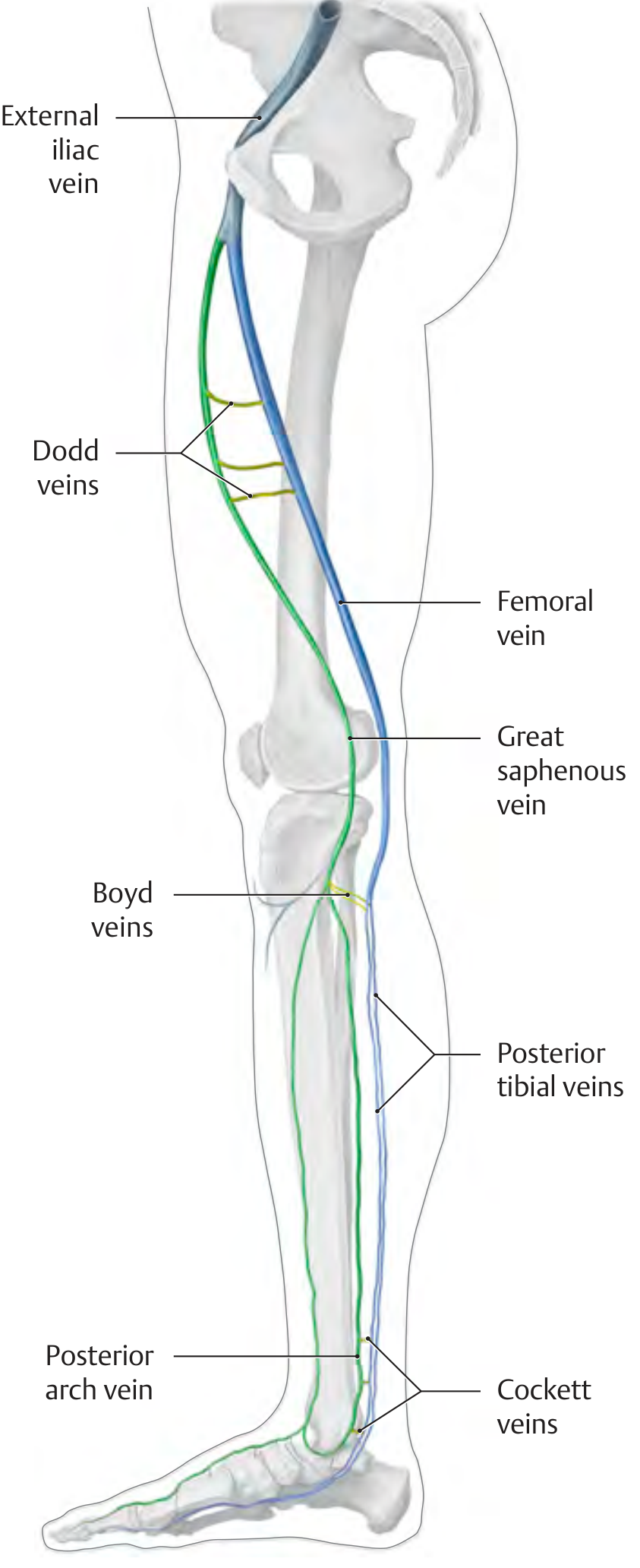
| Perforator | Location | Connects |
|---|---|---|
| Hunterian perforators | Mid/upper thigh | GSV ↔ Femoral vein |
| Dodd perforators | Distal third of thigh (adductor canal level) | GSV ↔ Femoral vein |
| Boyd perforators | Medial proximal leg (below knee) | GSV ↔ Posterior tibial veins |
| Cockett perforators I, II, III | Medial distal leg — 5, 10, 15 cm above medial malleolus | Posterior arch vein ↔ Posterior tibial veins |
Cockett's perforators are the most clinically important — their incompetence is directly responsible for venous ulcers on the medial gaiter area (lower third of leg), the classic site of venous ulceration.
Perforators Associated with SSV (Posterior)
- Popliteal fossa perforators — connect SSV to popliteal vein
- Gastrocnemius perforators — midportion of gastrocnemius muscle belly
- Ankle perforators — two near the lateral ankle
Complete Classification of Incompetence
VARICOSE VEINS
│
├── PRIMARY (junction incompetence)
│ ├── Saphenofemoral junction → GSV → Anterior/medial varicosities
│ └── Saphenopopliteal junction → SSV → Posterior varicosities
│
└── SECONDARY (perforator incompetence)
├── Hunterian → thigh varicosities
├── Dodd → lower thigh / popliteal
├── Boyd → medial calf
└── Cockett I/II/III → medial ankle / venous ulcers
Key Surgical Points (Bailey & Love)
- Tourniquet test localises the level of incompetence before surgery
- Treating only the junction without addressing incompetent perforators leads to recurrence
- Cockett perforators must be ligated (subfascial endoscopic perforator surgery — SEPS) when varicosities coexist with lipodermatosclerosis or ulceration
- Secondary varices (from DVT with perforator destruction) are not correctable by junction surgery alone
— THIEME Atlas of General Anatomy & Musculoskeletal System; Dermatology 5e; Pfenninger & Fowler's Procedures for Primary Care
This is a shared conversation. Sign in to Orris to start your own chat.