Classify mycobacteria, describe the morphology and clinical manifestations of M. tuberculosis, add a note on laboratory diagnosis of pulmonary tuberculosis.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
1) Classification of mycobacteria
A practical medical microbiology classification is:
- Mycobacterium tuberculosis complex (MTBC)
- M. tuberculosis, M. bovis, M. africanum, M. caprae, M. microti, M. pinnipedii (plus proposed species in some texts).
- Nontuberculous mycobacteria (NTM)
- Slow growers (>7 days on subculture), e.g. MAC, M. kansasii, M. marinum, M. xenopi.
- Rapid growers (<7 days), e.g. M. fortuitum, M. chelonae, M. abscessus.
- Some older systems further classify NTM by Runyon groups (photochromogens, scotochromogens, nonchromogens, rapid growers).
(From Tietz and Medical Microbiology textbook sections.)
2) Morphology of Mycobacterium tuberculosis
- Slender, straight or slightly curved rod-shaped bacillus.
- Strongly acid-fast (due to lipid-rich, mycolic acid-rich cell wall).
- Weakly Gram-positive appearance but not reliably seen on routine Gram stain.
- Obligate aerobe, nonmotile, non-spore-forming, non-capsulated.
- Slow grower: colonies on LJ/Middlebrook usually visible in weeks (commonly 2-8 weeks on solid media; earlier in liquid systems).
- Intracellular survival in macrophages; inhibits phagolysosome fusion.
3) Clinical manifestations of tuberculosis (especially pulmonary TB)
Typical pulmonary features:
- Persistent cough (may be productive)
- Fever (often low-grade), night sweats
- Weight loss, malaise, fatigue, anorexia
- Hemoptysis (usually in more advanced disease)
- Chest pain, dyspnea in some patients
Patterns:
- Primary TB: often middle/lower zone involvement with hilar lymphadenopathy; may have pleural effusion.
- Reactivation TB: classically upper lobe/apical-posterior disease, often cavitary.
- Disseminated (miliary) TB: hematogenous spread with severe systemic illness.
- Extrapulmonary disease can involve lymph nodes, meninges, bone/joint, genitourinary tract, pericardium, etc., especially in immunocompromised patients.
4) Note on laboratory diagnosis of pulmonary tuberculosis
A concise exam-style outline:
A. Specimen
- Sputum (spot + early morning; many guidelines still use 2-3 specimens).
- Induced sputum/BAL if non-productive cough.
B. Microscopy
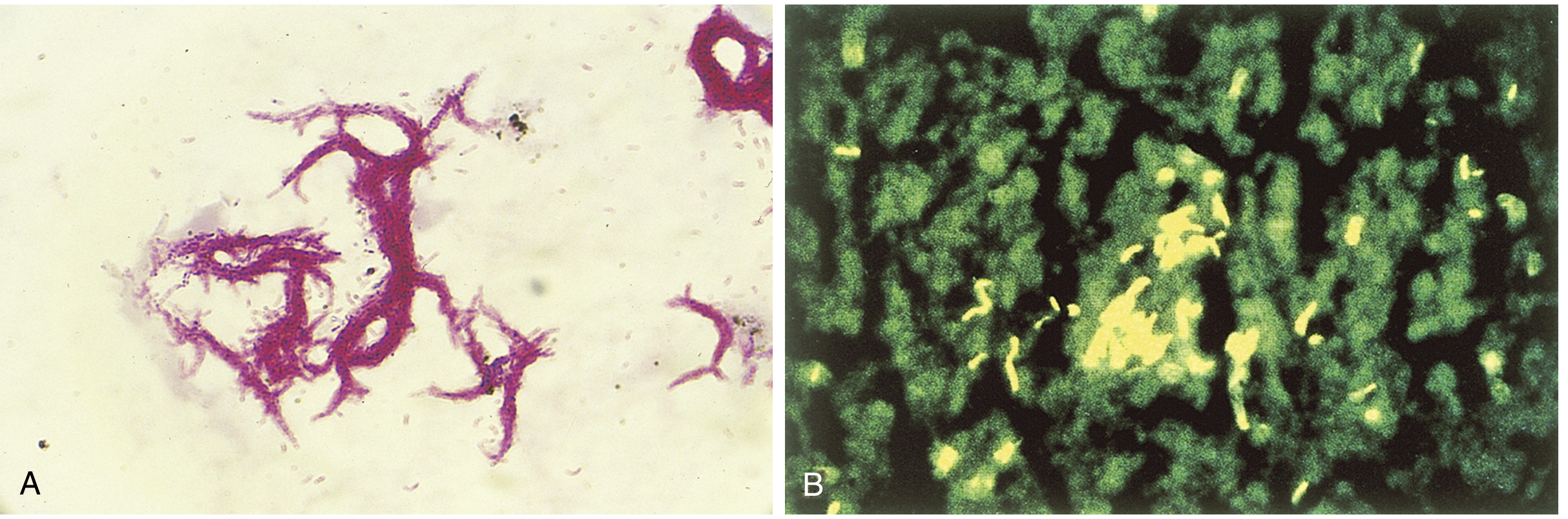
- AFB smear:
- Ziehl-Neelsen (hot), Kinyoun (cold), or fluorochrome (auramine-rhodamine).
- Rapid and inexpensive, but limited sensitivity; cannot distinguish MTBC from all NTM by smear alone.
C. Nucleic acid amplification tests (NAAT)
- Recommended on at least one initial respiratory specimen.
- Provides rapid detection of MTBC DNA and often rifampicin resistance markers (e.g., Xpert platforms).
- Positive NAAT with compatible clinical picture supports early diagnosis.
- Negative NAAT does not fully exclude TB in high-suspicion cases.
D. Culture (gold standard for confirmation)
- Solid media (LJ, Middlebrook) and/or liquid broth systems.
- Higher sensitivity than smear; enables species ID and full drug susceptibility testing.
- Liquid culture detects growth faster than solid media.
E. Identification and drug resistance testing
- Molecular probes/line probe assays, sequencing, MALDI-TOF (from cultured isolates depending on setup).
- Phenotypic or genotypic DST for INH, rifampicin, and other drugs, especially with MDR/XDR risk.
F. Supportive tests
- Chest radiography/CT supports diagnosis but is not definitive.
- TST/IGRA indicate infection/exposure, not reliable stand-alone tests for active pulmonary TB diagnosis.
Source used: Medical Microbiology 9e, Tietz Textbook of Laboratory Medicine, and Murray & Nadel's Textbook of Respiratory Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.