Hirsutism
Reading File
Finding Sources
Searching PubMed
hirsutism management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of hirsutism drawn from Harrison's, Fitzpatrick's, Family Medicine, and Goodman & Gilman's.
Hirsutism
Definition
Hirsutism is the presence of excess terminal (coarse, pigmented) hair in women growing in a male-pattern distribution - affecting androgen-sensitive areas such as the upper lip, chin, cheeks, chest, lower abdomen, inner thighs, and back. It is distinct from hypertrichosis, which is a generalized increase in fine vellus hair that is androgen-independent (associated with hypothyroidism, anorexia nervosa, or drugs like minoxidil, diazoxide, diphenylhydantoin).
Prevalence: ~5-15% of women of reproductive age.
Pathogenesis
The hair follicle cycle has three phases: anagen (growth), catagen (involution), and telogen (rest). Androgens drive conversion of vellus hair into terminal hair by activating androgen receptors in the follicle.
- Testosterone and DHT are the key androgens. DHT is the most potent - formed locally within the hair follicle by 5α-reductase acting on testosterone.
- DHT binds nuclear androgen receptors, activating genes that convert vellus to terminal hair in androgen-sensitive regions.
- Androgens are produced by the ovaries (under LH control) and adrenal glands (under ACTH), with additional peripheral conversion.
Two main drivers:
- Elevated circulating androgens (most common)
- Increased end-organ sensitivity to normal androgen levels (idiopathic hirsutism) - due to upregulated 5α-reductase activity or intrinsic androgen receptor hyperresponsiveness
Causes
| Etiology | Key Features |
|---|---|
| Idiopathic hirsutism (IH) | Regular ovulation, normal/slightly elevated androgens; diagnosis of exclusion; prevalence 4-7% |
| PCOS (most common secondary cause) | Chronic anovulation, insulin resistance, infertility; >50% present with hirsutism, often truncal |
| Non-classical CAH (21-hydroxylase deficiency) | Late-onset; elevated 17-hydroxyprogesterone |
| HAIR-AN syndrome | Hyperandrogenism + Insulin Resistance + Acanthosis Nigricans; 1-5% of hyperandrogenic women |
| Androgen-secreting tumors | Ovarian or adrenal; rapid/abrupt onset is a red flag for malignancy |
| Ovarian hyperthecosis | Severe hyperandrogenism; nests of luteinized theca cells in ovarian stroma |
| Hyperprolactinemia | Via stimulation of adrenal androgens |
| Exogenous androgens | Anabolic steroids, danazol, some progestins |
| Cushing syndrome | Cortisol excess with adrenal androgen co-production |
Assessment: Modified Ferriman-Gallwey (mFG) Score
The mFG score is the standard assessment tool. Nine body areas are each scored 0 (no hair) to 4 (frankly virile):
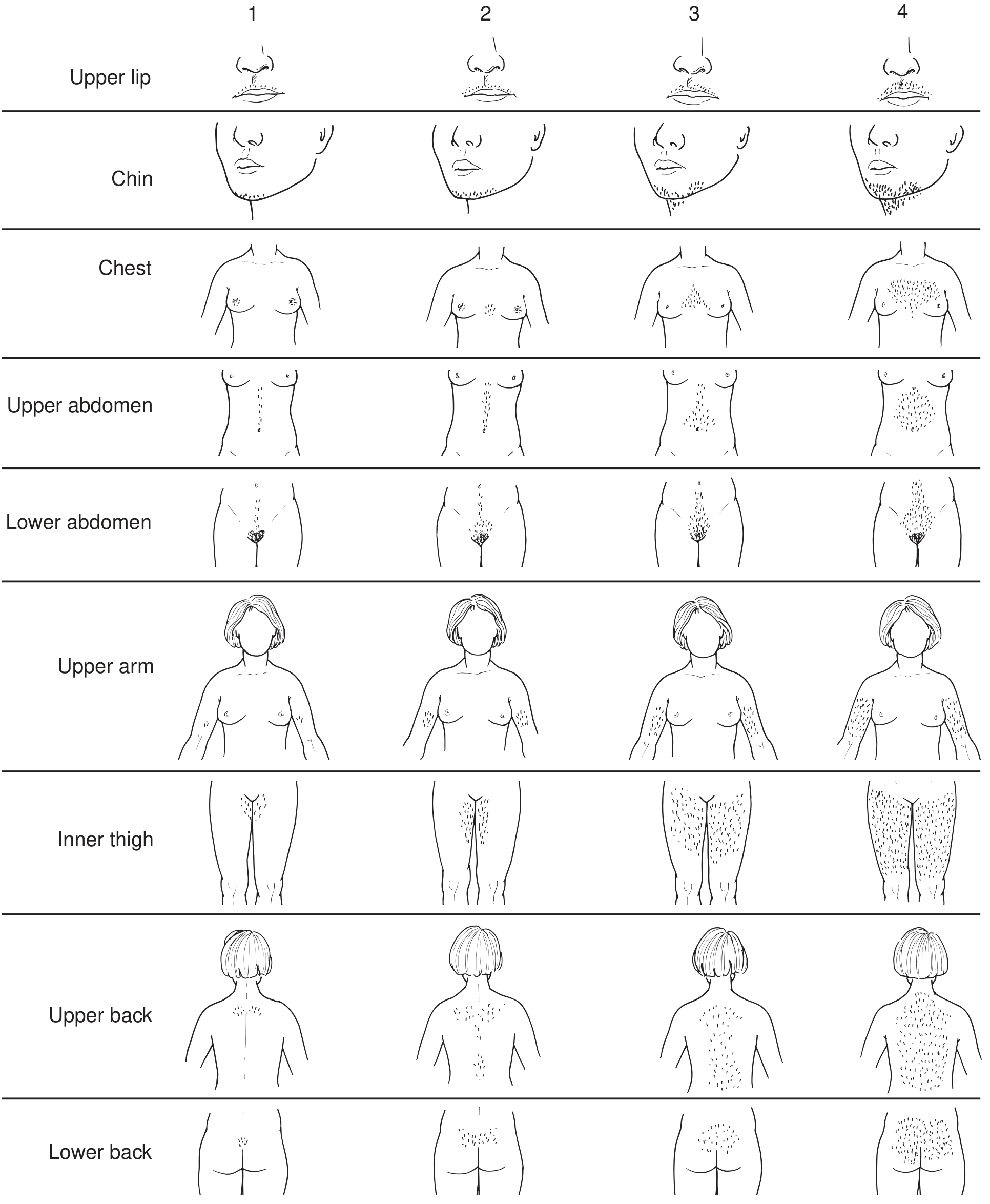
The nine areas: upper lip, chin/cheeks, chest, upper abdomen, lower abdomen, upper arm, inner thigh, upper back, lower back.
| Score | Interpretation |
|---|---|
| ≤8 | Normal |
| 8-14 | Mild hirsutism |
| ≥15 | Moderate to severe hirsutism |
Important: Ethnic variation matters - Asian women have lower baseline hair density, Mediterranean women naturally have higher scores. Normal ethnic variation must be distinguished from pathologic hyperandrogenism.
Clinical Evaluation
History: Age of onset, menstrual irregularity, rate of progression (rapid onset = malignancy concern), medications/supplements, family history, ethnic background.
Signs of virilization (suggests significant androgen excess - investigate aggressively):
- Clitoromegaly
- Male-pattern balding
- Voice deepening
- Decreased breast size
Other cutaneous signs of hyperandrogenism: Acne, acanthosis nigricans, androgenetic alopecia, seborrheic dermatitis.
When to test hormones:
- Mild hirsutism + regular cycles: Likely idiopathic; hormone testing not mandatory
- Moderate-severe hirsutism OR any hirsutism + irregular cycles OR virilization: Mandatory hormone workup
Laboratory workup:
- Total and bioavailable testosterone
- DHEA-S (adrenal androgen marker)
- 17-hydroxyprogesterone (to rule out non-classical CAH)
- Prolactin (if suspected hyperprolactinemia)
- 24-hour urine 17-ketosteroids (if adrenal tumor suspected)
- Imaging: pelvic ultrasound (ovarian cysts/masses), CT/MRI (adrenal masses)
Treatment
Non-pharmacologic (for all patients, alone or as adjunct)
| Method | Notes |
|---|---|
| Shaving | Does NOT increase hair rate or density (common misconception) |
| Chemical depilatory creams | Useful for mild/limited areas; may cause irritation |
| Waxing/plucking | Temporary removal; waxing is uncomfortable |
| Electrolysis | Effective for permanent removal of small areas |
| Laser / Intense Pulsed Light (IPL) | Best for large areas of pigmented terminal hair; selective photothermolysis via melanin absorption; permanent in many patients |
Recent 2024 systematic review (PMID 38630483, JAMA Dermatol) supports laser and light-based therapies for hirsutism in PCOS women.
Pharmacologic
Response is typically not visible for 4-6 months; maximum effect may take 9-12 months (due to the hair growth cycle length).
1. Combined oral contraceptive pills (first-line)
- Suppress LH → reduce ovarian androgen production
- Increase SHBG → reduce free testosterone
- Direct suppressive effect on sebaceous glands
- ~20% improvement in hirsutism; ~50% improvement in acne
- Progestin choice matters: Prefer drospirenone (anti-androgenic, spironolactone analogue) or norgestimate (non-androgenic); avoid norgestrel/levonorgestrel (androgenic)
- Contraindicated in thromboembolic disease, estrogen-dependent cancers; relative CI in smokers, hypertension, migraine
2. Spironolactone (100-200 mg/day)
- Mineralocorticoid antagonist + weak antiandrogen (competitive androgen receptor inhibitor)
- Nearly as effective as cyproterone acetate at adequate doses
- Monitor: hyperkalemia, hypotension
- Must avoid pregnancy (risk of feminization of male fetus)
- Often combined with OCP to regularize cycles and prevent pregnancy
3. Cyproterone acetate (50-100 mg days 1-15)
- Prototypic antiandrogen - competitive inhibitor of testosterone and DHT binding to androgen receptor
- Also enhances hepatic clearance of testosterone
- Combined with ethinyl estradiol (50 μg days 5-26)
- Not available in the US, but widely used in Canada, Mexico, Europe
- Side effects: irregular bleeding, nausea, headache, fatigue, weight gain, decreased libido
4. Finasteride
- Competitive inhibitor of 5α-reductase type 2
- Limited efficacy in hirsutism (type 1 predominates in pilosebaceous unit)
- Avoid in women who may become pregnant (male fetal feminization risk)
- Dutasteride (inhibits both 5α-reductase types 1 and 2) may have better efficacy; evidence growing
5. Flutamide
- Potent nonsteroidal antiandrogen; effective but rarely used
- Risk of hepatocellular toxicity limits use
6. Glucocorticoids
- Used specifically for CAH-related hirsutism
- OCPs preferred first-line even in CAH; glucocorticoids added if OCP response is inadequate
- Use lowest effective dose (e.g., dexamethasone 0.2-0.25 mg/day at bedtime)
7. Topical eflornithine
- Inhibits ornithine decarboxylase in hair follicles → slows growth
- Facial hirsutism; used as adjunct to laser/IPL
8. Metformin / insulin sensitizers
- Used when hirsutism is driven by insulin resistance (PCOS)
- A 2026 systematic review (PMID 41277478, Clin Endocrinol) supports short-term low-dose spironolactone for PCOS-related hyperandrogenism
Summary Algorithm
Hirsutism
|
├── Mild + regular cycles → mFG score, cosmetic treatment, OCP if desired
|
├── Moderate-severe OR irregular cycles → Full hormone workup
| ↓
| Elevated T (>200 ng/dL) or DHEA-S (>700 µg/dL) → Imaging for tumor
| 17-OHP elevated → Non-classical CAH
| PCOS criteria → OCP ± spironolactone + lifestyle
|
└── Virilization → Urgent evaluation, rule out androgen-secreting tumor
Sources: Harrison's Principles of Internal Medicine 22E, p. 3184-3185 | Fitzpatrick's Dermatology Vol. 1-2, pp. 1585-1590 | Textbook of Family Medicine 9e, p. 1053 | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.