Sketch showing the patho physiology of anaphylaxis reaction
anaphylaxis pathophysiology mechanism diagram IgE mast cell
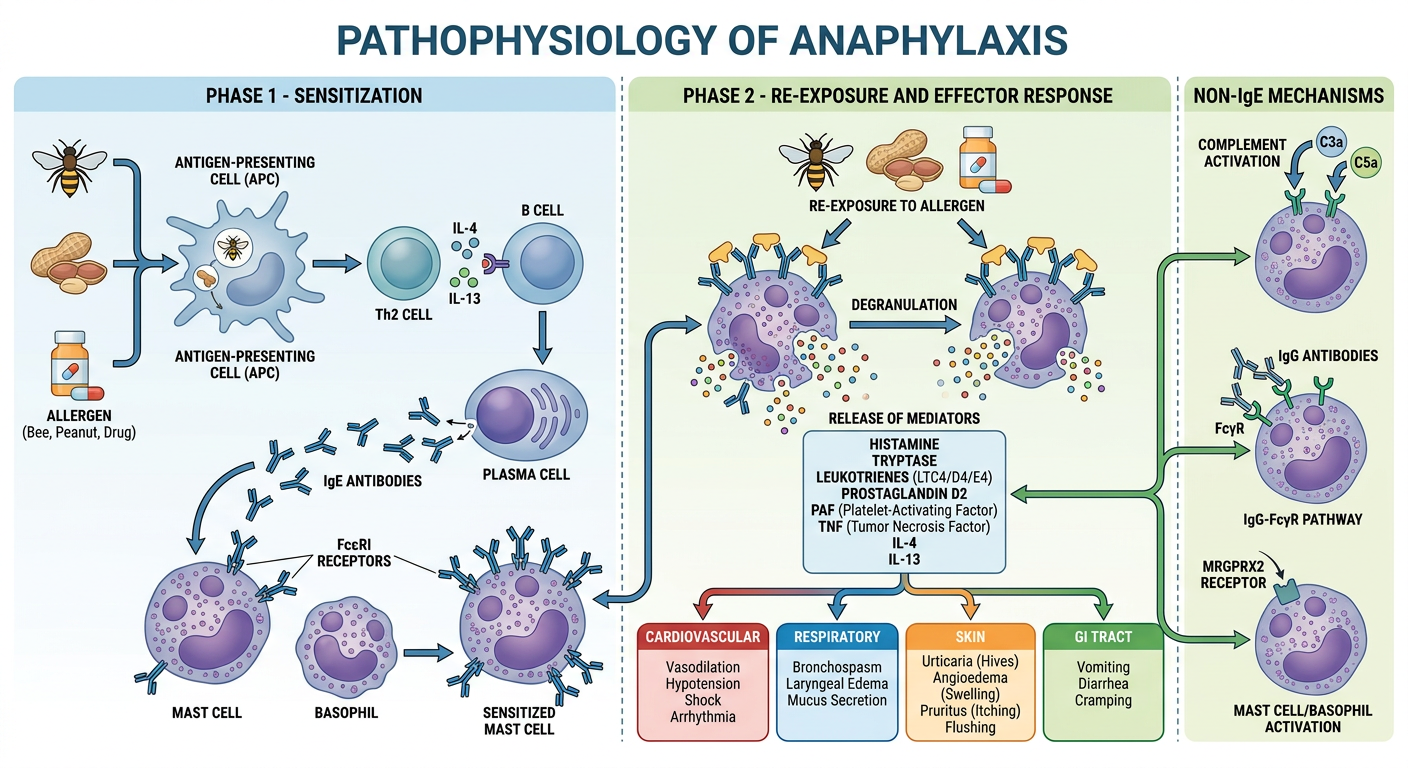
A detailed medical educational diagram showing the pathophysiology of anaphylaxis. The diagram has two phases labeled clearly: Phase 1 - Sensitization and Phase 2 - Re-exposure and Effector Response. Phase 1 shows: Allergen (bee, peanut, drug icons) → Antigen-presenting cell → Th2 cell releasing IL-4 and IL-13 → B cell → Plasma cell producing IgE antibodies → IgE binding to FcεRI receptors on mast cells and basophils (shown as a sensitized mast cell). Phase 2 shows: Re-exposure to allergen → Allergen cross-links IgE on mast cell → Mast cell and basophil degranulation → Release of mediators (histamine, tryptase, leukotrienes LTC4/D4/E4, prostaglandin D2, PAF, TNF, IL-4, IL-13). Below that, arrows show the end-organ effects in separate boxes: Cardiovascular (vasodilation, hypotension, shock, arrhythmia), Respiratory (bronchospasm, laryngeal edema, mucus secretion), Skin (urticaria, angioedema, pruritus, flushing), GI tract (vomiting, diarrhea, cramping). A separate pathway on the side shows non-IgE mechanisms: complement activation (C3a, C5a), IgG-FcγR pathway, and MRGPRX2 receptor. Clean, professional medical illustration style with color coding, arrows, and labeled boxes.
Pathophysiology of Anaphylaxis
Generated Sketch
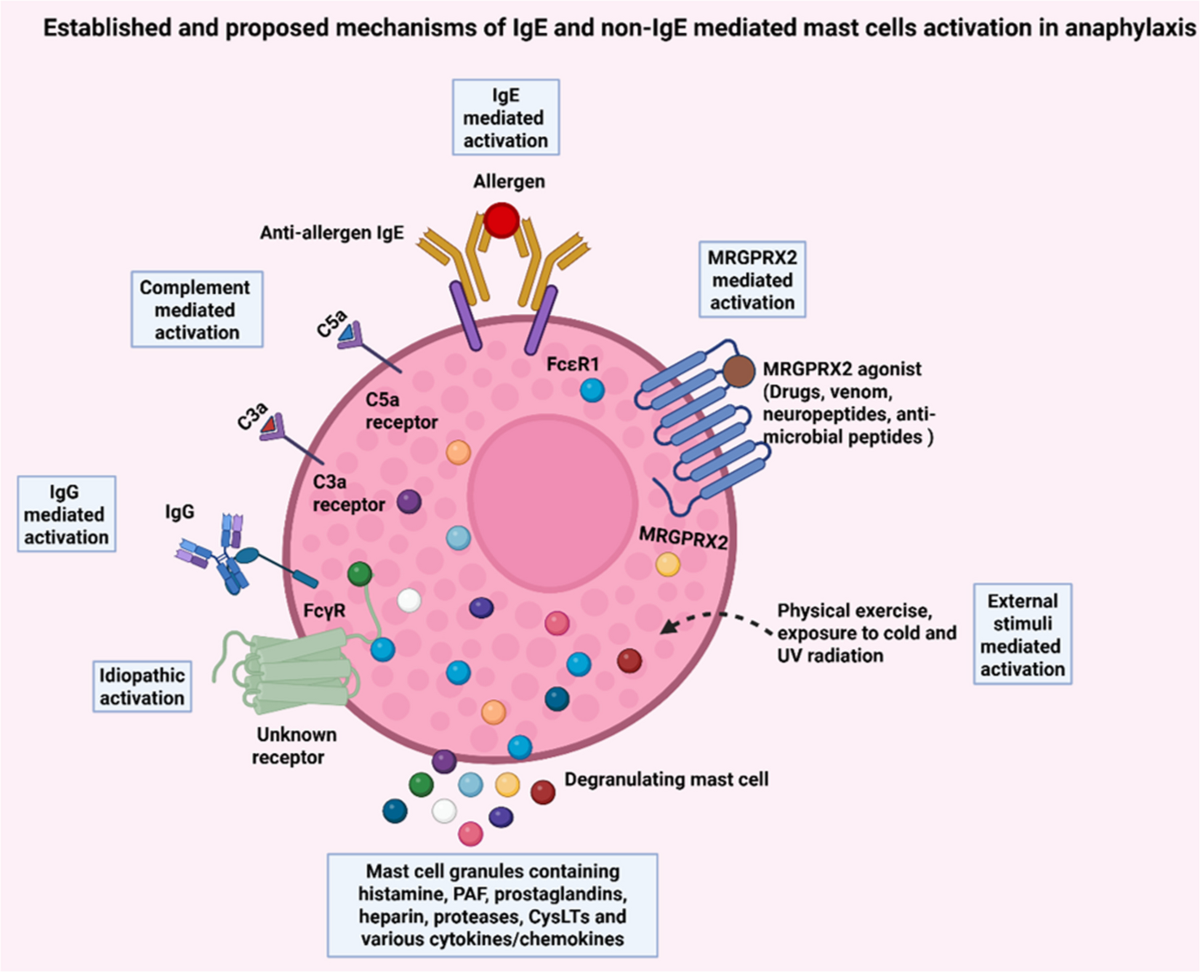
Established & Proposed Mechanisms of Mast Cell Activation (from Springer Nature, 2025)
Step-by-Step Pathophysiology
Phase 1 - Sensitization (First Exposure)
- Allergen entry - A foreign antigen (food, drug, venom, latex) enters the body.
- Th2 polarization - Antigen-presenting cells activate Th2 lymphocytes, which release IL-4 and IL-13.
- IgE production - IL-4/IL-13 drive B cells to undergo class switching, producing allergen-specific IgE antibodies.
- Mast cell arming - IgE binds with high affinity to FcεRI receptors on mast cells (tissue) and basophils (blood). The individual is now sensitized - no symptoms yet.
Phase 2 - Re-exposure and Effector Response
- Allergen cross-linking - On re-exposure, the multivalent allergen bridges two or more IgE molecules on the mast cell surface, cross-linking FcεRI receptors.
- Intracellular signaling - Cross-linking activates Lyn and Syk kinases → PLCγ → IP3 + DAG → rise in intracellular Ca²⁺ → triggers degranulation.
- Mediator release - Mast cells and basophils release a cascade of mediators:
| Mediator | Source | Key Effect |
|---|---|---|
| Histamine | Preformed granules | Vasodilation, increased vascular permeability, bronchoconstriction, pruritus |
| Tryptase | Preformed granules | Activates complement, kallikrein; marker of anaphylaxis |
| Leukotrienes (LTC4, LTD4) | Newly synthesized | Potent bronchoconstriction, mucus secretion, vascular permeability |
| Prostaglandin D2 (PGD2) | Newly synthesized | Vasodilation, platelet aggregation inhibition |
| PAF (Platelet-Activating Factor) | Newly synthesized | Bronchoconstriction, hypotension |
| TNF-α, IL-4, IL-13 | Cytokines | Late-phase inflammation, sustained symptoms |
End-Organ Effects
| System | Manifestation |
|---|---|
| Cardiovascular | Vasodilation → hypotension → distributive shock; tachycardia, arrhythmia |
| Respiratory | Bronchospasm, laryngeal edema (stridor), excess mucus → hypoxia, respiratory arrest |
| Skin/Mucosa | Urticaria, angioedema, flushing, pruritus |
| GI Tract | Nausea, vomiting, cramping, diarrhea |
| Neurological | Anxiety, dizziness, syncope (from hypotension) |
Non-IgE Pathways (Anaphylactoid Reactions)
- Complement activation - C3a and C5a (anaphylatoxins) directly activate mast cells via C3a/C5a receptors.
- IgG-FcγR pathway - IgG immune complexes activate mast cells, neutrophils, and macrophages via FcγR (common with monoclonal antibodies, chemotherapy).
- MRGPRX2 receptor - Drugs (opioids, neuromuscular blocking agents), venom, and neuropeptides directly activate mast cells via this G-protein-coupled receptor - independent of IgE.
- Physical stimuli - Exercise, cold, UV radiation can also trigger degranulation via external stimuli pathways.
The Biphasic Response
- Early phase (0-60 min): Dominated by preformed mediators (histamine, tryptase) - urticaria, bronchospasm, hypotension.
- Late phase (4-12 hrs): Driven by newly synthesized mediators (leukotrienes, cytokines) and recruited eosinophils/neutrophils - can cause recurrence even after initial treatment.
Sources: Goldman-Cecil Medicine, 26th ed.; Andrews' Diseases of the Skin; IgE and non-IgE-mediated pathways in anaphylaxis - Seminars in Immunopathology (2025)