Can you explain me renal calculus for my surgery exam in easy language as also I can use it as a detailed answer of 10 marks with diagram
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information I need for a comprehensive, exam-ready answer. Let me compose the full detailed answer.
Renal Calculus (Urolithiasis) - Complete 10-Mark Answer
Definition
A renal calculus (plural: calculi) is a stone-like deposit that forms within the kidney or anywhere in the urinary collecting system. The condition is called urolithiasis (or nephrolithiasis when specifically in the kidney). Calculi form when the concentration of stone-forming substances in urine exceeds their solubility - a state called supersaturation.
- More common in males than females (2:1 ratio)
- Peak incidence: 4th to 6th decade of life
- Lifetime risk: ~9% in men, ~5% in women
- Strong familial tendency - runs in families
Diagram 1 - Sites of Calculi & Urinary Obstruction
(From Robbins Basic Pathology - Causes of urinary tract obstruction)
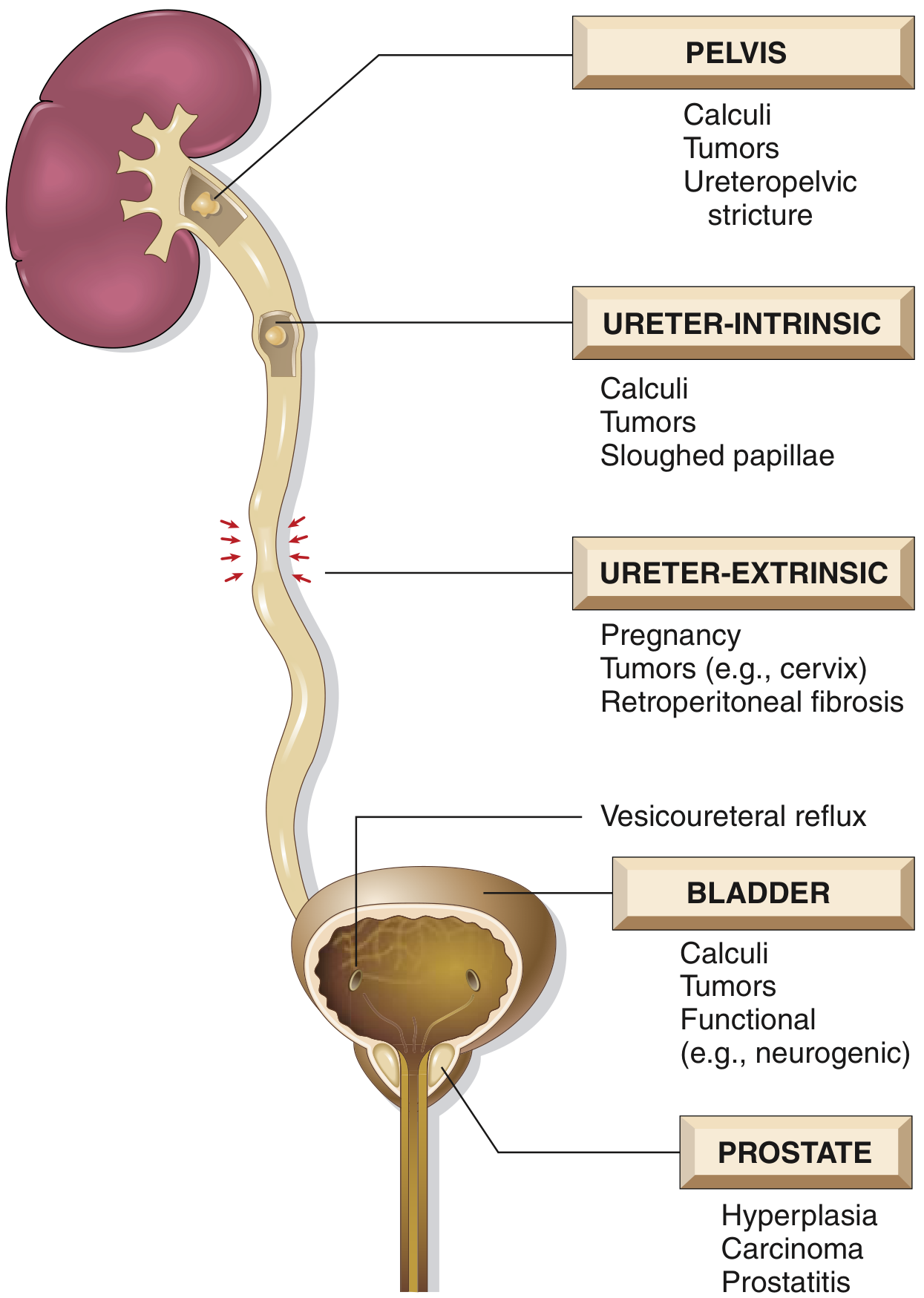
Calculi can lodge at: (1) pelviureteric junction (PUJ), (2) pelvic brim where ureter crosses iliac vessels, (3) vesicoureteric junction (VUJ) - the narrowest point.
Etiopathogenesis (How Stones Form)
The basic mechanism is supersaturation of urine - when the concentration of a mineral exceeds its ability to stay dissolved. Three factors tip the balance:
- Concentration of solute - dehydration raises all mineral concentrations
- Changes in urine pH - acidic urine favors uric acid/cystine stones; alkaline urine favors calcium phosphate and struvite stones
- Bacterial infections - urea-splitting organisms raise urine pH and release ammonia
- Absence of inhibitors - citrate, magnesium, pyrophosphate normally prevent crystal aggregation; low citrate = stone-prone
- Nidus formation - bacteria, desquamated epithelial cells (e.g., in vitamin A deficiency) act as seeds for crystal deposition
An organic mucoprotein matrix (~2.5% of stone weight) is present in all stone types and holds the crystal lattice together.
Types of Renal Stones
| Stone Type | Composition | Frequency | Key Cause | Radiopacity | pH | Shape/Feature |
|---|---|---|---|---|---|---|
| Calcium oxalate / phosphate | CaC₂O₄ or CaHPO₄ | 80% | Hypercalciuria, hyperoxaluria | Radiopaque | Acidic (oxalate), Alkaline (phosphate) | Spiky "jackstone" appearance |
| Struvite (Triple phosphate) | Mg-NH₄-PO₄ | 10% | UTI with urea-splitting bacteria (Proteus vulgaris, Staphylococcus) | Radiopaque | Alkaline | Can form staghorn calculus filling entire renal pelvis |
| Uric acid | Uric acid | 6-7% | Gout, leukemia treatment, hyperuricosuria | Radiolucent | Acidic | Smooth, yellow |
| Cystine | Cystine | 1-2% | Hereditary cystinuria (autosomal recessive) | Faintly opaque | Acidic | Hexagonal crystals in urine |
Memory trick - "CSUC": Calcium (80%), Struvite (10%), Uric acid (7%), Cystine (2%)
Causes of Hypercalciuria (most common predisposing factor):
- Absorptive - gut absorbs too much calcium (most common)
- Renal - kidney fails to reabsorb calcium - excretes excess
- Resorptive - hyperparathyroidism causes bone breakdown releasing calcium
- Immobilization, sarcoidosis, vitamin D excess, malignancy
Clinical Features (Symptoms)
The Classic Presentation - Renal Colic
- Sudden, severe, colicky flank pain radiating to groin ("loin to groin" pain)
- Pain waxes and wanes but position changes do NOT relieve it (differentiates from musculoskeletal)
- Nausea and vomiting (visceral response to ureteric distension)
- Hematuria - either visible (gross) or on dipstick (microscopic) - present in >80%
- Dysuria and urinary frequency - when stone is near vesicoureteric junction
Danger Signs (Emergency):
- Fever + obstruction = Pyonephrosis/urosepsis - SURGICAL EMERGENCY
- Anuria = bilateral obstruction or obstruction of a solitary kidney
Chronic/Asymptomatic Stones:
- Detected incidentally on imaging (e.g., during hematuria workup)
- Staghorn calculi may present with recurrent UTIs and flank dull ache
Investigations
1. Urine Examination
- Dipstick/microscopy: Hematuria (>80%), pyuria if infected
- Urine culture: Identify infecting organism
- 24-hour urine: pH, calcium, oxalate, uric acid, citrate, creatinine, sodium - for metabolic workup
2. Blood Tests
- Serum calcium, phosphate, uric acid - identify metabolic cause
- Serum creatinine + eGFR - assess renal function
- CBC - leukocytosis suggests infection
- Parathyroid hormone (PTH) - if hypercalcemia present
3. Imaging
First-line: Non-contrast CT abdomen & pelvis (NCCT KUB)
- Gold standard - sensitivity ~97%, specificity ~97%
- Detects ALL stone types (including radiolucent uric acid stones)
- Shows stone size, location, degree of hydronephrosis, and secondary signs
Plain X-ray KUB (Kidneys-Ureters-Bladder)
- Quick and cheap
- Shows only radiopaque stones (85% of stones)
- Uric acid stones are INVISIBLE on plain X-ray
Ultrasound
- No radiation - ideal for pregnant women and children
- Shows hydronephrosis and large stones well
- Misses small ureteric stones
Intravenous Urogram (IVU/IVP)
- Older technique but still used in some centers
- Shows anatomy and degree of obstruction
Diagram 2 - Staghorn Calculus on X-ray KUB
(Bailey & Love's Surgery - Staghorn calculus in left kidney)

Management
A. Immediate/Emergency Management (Acute Renal Colic)
- Pain relief (first priority):
- IV NSAIDs (Ketorolac) - first line; reduces ureteral spasm
- IV Opioids (Morphine) - if NSAIDs contraindicated
- IV fluids for hydration
- If infection + obstruction = EMERGENCY decompression:
- Cystoscopic ureteral stent placement, OR
- Percutaneous nephrostomy - to drain the obstructed kidney
- Then treat infection; plan definitive stone removal later
B. Medical Expulsive Therapy (MET) - For Small Stones <10mm
- Tamsulosin (alpha-1 blocker) - relaxes smooth muscle of ureter, promotes stone passage
- High fluid intake (>2 liters/day)
- Most stones <5mm pass spontaneously within 4-6 weeks
- Patient must be observed with re-imaging if no evidence of passage
C. Interventional / Surgical Treatment
| Procedure | Indications | Notes |
|---|---|---|
| ESWL (Extracorporeal Shock Wave Lithotripsy) | Renal/upper ureteric stones <2cm | Shockwaves crush stone; fragments pass in urine. May cause "steinstrasse" (stone street) |
| Ureteroscopy (URS) + Laser | Ureteric stones, small renal stones | Endoscope inserted through urethra; laser fragmentation (holmium laser) |
| PCNL (Percutaneous Nephrolithotomy) | Large stones >2cm, staghorn calculi | Needle puncture through back into kidney; tract dilated; nephroscope removes stone |
| Laparoscopic/Open surgery | Failed minimally invasive treatment | Rare today; pyelolithotomy, nephrolithotomy |
D. Prevention (Long-term Medical Management)
| Stone Type | Dietary/Lifestyle | Drug Treatment |
|---|---|---|
| Calcium stones | Increase fluid, reduce salt & animal protein, normal calcium intake | Thiazide diuretics (reduce urinary calcium), Potassium citrate (increases citrate, raises pH) |
| Uric acid stones | Reduce purine-rich foods (red meat, organ meats), increase fluids | Allopurinol (reduces uric acid), Potassium citrate (alkalinizes urine) |
| Struvite stones | Treat underlying UTI completely | Long-term antibiotics; complete stone removal essential |
| Cystine stones | High fluid intake (>3L/day), reduce methionine | D-penicillamine or Tiopronin (chelate cystine) |
Complications of Renal Calculus
- Hydronephrosis - progressive dilatation of collecting system due to obstruction
- Pyelonephritis / Pyonephrosis - infected, obstructed kidney - life-threatening
- Urosepsis - systemic sepsis from infected obstructed kidney
- Chronic kidney disease (CKD) - from repeated obstruction and infection
- Renal atrophy / loss of kidney - end-stage untreated obstruction
- Squamous cell carcinoma of renal pelvis - rare, associated with chronic staghorn calculi
- Steinstrasse - "stone street" - multiple stone fragments blocking ureter after ESWL
Key Points for Exam Memory
- Commonest stone = Calcium oxalate (80%); radiopaque
- Radiolucent stone = Uric acid (appears on CT but not X-ray)
- Staghorn calculus = Struvite (from Proteus UTI); fills entire renal pelvis
- Most dangerous complication = Pyonephrosis (infected obstructed kidney)
- Gold standard imaging = Non-contrast CT (NCCT KUB)
- MET drug = Tamsulosin (alpha-blocker)
- ESWL for stones <2cm; PCNL for stones >2cm or staghorn
- Pain of renal colic is NOT relieved by position change (unlike musculoskeletal)
Sources: Robbins & Kumar Basic Pathology (Table 12.5); Sabiston Textbook of Surgery, 21e; Bailey & Love's Short Practice of Surgery, 28e
Adenocarcinoma (renal cell carcinoma)
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive content from all major surgical textbooks. Let me compile the complete answer.
Renal Cell Carcinoma (RCC) / Adenocarcinoma of the Kidney
Complete 10-Mark Surgery Exam Answer
Definition
Renal Cell Carcinoma (RCC) is a malignant tumor arising from the proximal renal tubular epithelium of the renal cortex. It is histologically classified as an adenocarcinoma and accounts for:
- 80-90% of all primary malignant neoplasms of the kidney
- 2-3% of all cancers in adults
- Male : Female ratio = 2:1
- Peak age: 6th to 7th decade (55-75 years)
It is also called Grawitz tumor, hypernephroma, or clear cell carcinoma (for the most common subtype).
Etiology / Risk Factors
| Risk Factor | Notes |
|---|---|
| Cigarette smoking | Single strongest environmental risk factor |
| Obesity | Risk increases with BMI |
| Hypertension | Independent risk factor |
| Chronic renal dialysis (ARCD) | Acquired renal cystic disease on long-term haemodialysis - 30x increased risk |
| Cadmium exposure | Occupational risk |
| Petrochemicals/dyes | Occupational risk |
| Diuretics | Associated risk |
| Von Hippel-Lindau (VHL) disease | Autosomal dominant; 40-60% develop bilateral clear cell RCC |
| Family history | 4-6% of RCC are familial |
Pathology
Gross Appearance
- Located in the renal cortex, usually upper pole
- Characteristically solitary, well-circumscribed, rounded mass
- Bulges out of the renal contour, often compressing normal parenchyma
- Cut surface: bright yellow-orange (due to high lipid content) with areas of hemorrhage, necrosis, and cystic change
- Has a pseudocapsule of compressed renal tissue
Diagram 1 - Gross Pathology of Clear Cell RCC
(Bailey & Love's Surgery - Cut surface of kidney showing large clear-cell RCC in upper pole with characteristic yellowish areas)

Histological Types
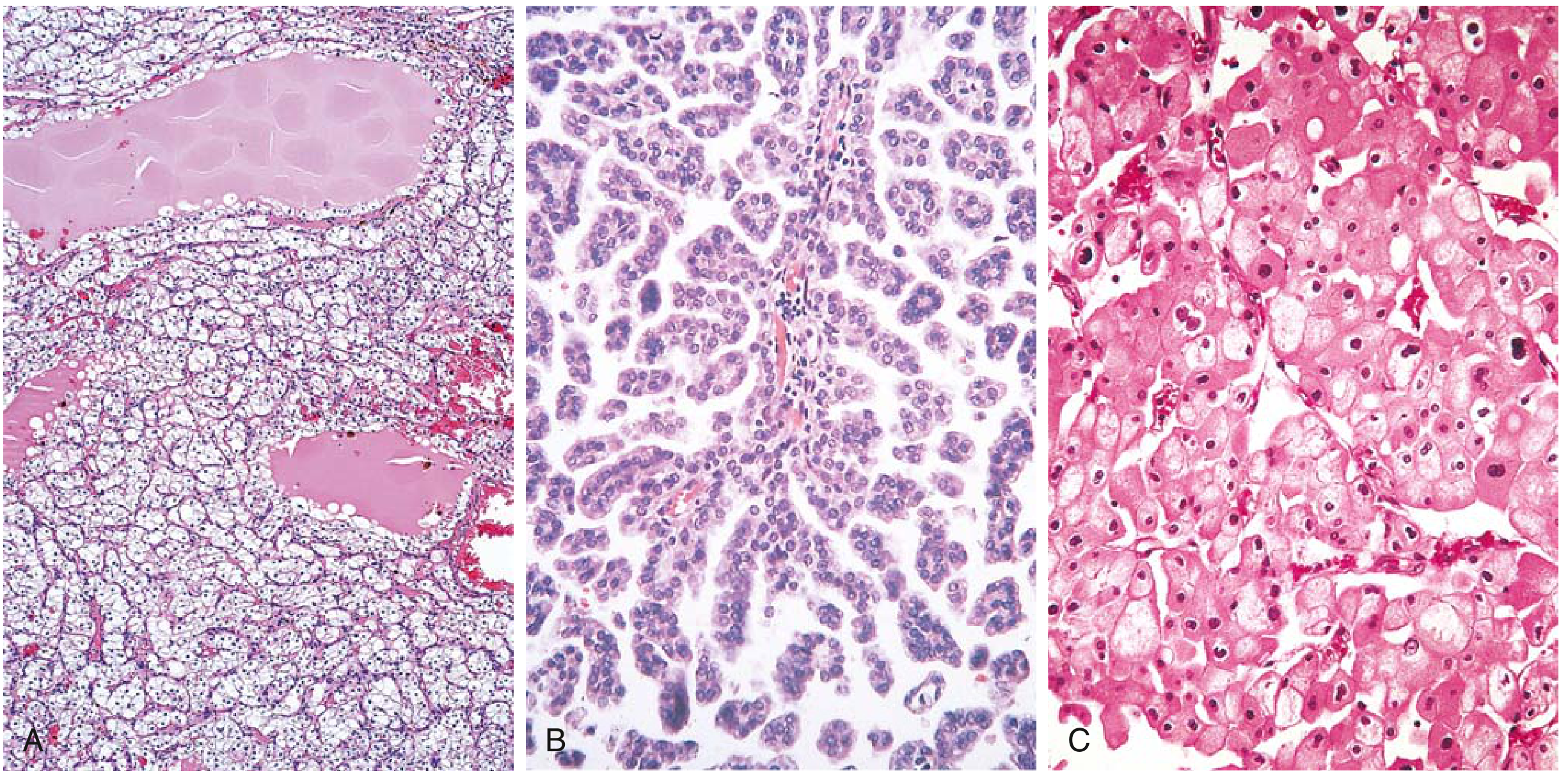
Diagram 2 - Histology of RCC Subtypes (H&E stain)
(Robbins Basic Pathology - A: Clear cell, B: Papillary, C: Chromophobe)
| Subtype | Frequency | Origin | Genetics | Key Features | Prognosis |
|---|---|---|---|---|---|
| Clear Cell RCC | 65% | Proximal tubule | VHL gene deletion (chr 3p) | Clear cytoplasm (lipid-rich); bright yellow gross; highly vascular | Intermediate |
| Papillary RCC | 10-15% | Proximal tubule | MET gene (chr 7q) amplification | Papillary fronds; often bilateral/multifocal; less yellow | Relatively better |
| Chromophobe RCC | 5% | Intercalated cells of collecting duct | Chromosome losses (1, 2, 6, 10, 17) | Eosinophilic cytoplasm; perinuclear halos; tan-brown | Best prognosis |
| Collecting duct carcinoma | 1-2% | Collecting duct (medulla) | - | Centrally located; aggressive | Poor |
| Renal medullary carcinoma | <0.5% | Collecting duct | - | Young patients; sickle cell trait; centrally located | Very poor |
Molecular Pathogenesis of Clear Cell RCC (most important for exams):
- VHL gene (Tumor suppressor) on chromosome 3p25 is mutated/lost
- VHL protein normally degrades HIF (Hypoxia Inducible Factor)
- Without VHL → HIF accumulates even in normal oxygen conditions
- HIF stimulates VEGF (Vascular Endothelial Growth Factor) → rich tumor vascularity
- This is why RCC is highly vascular and why anti-VEGF drugs work in RCC treatment
Spread of RCC
RCC is notorious for unusual patterns of spread - a key exam point:
1. Local Spread
- Through the renal capsule into perinephric fat
- Into the renal sinus and collecting system
2. Venous Extension (Characteristic of RCC!)
- RCC has a special tendency to grow into the renal vein as a tumor thrombus
- Can extend into the Inferior Vena Cava (IVC) and even up to the right atrium
- This is a unique hallmark of RCC
3. Lymphatic Spread
- To para-aortic and paracaval lymph nodes
4. Hematogenous Spread (Most common route)
- Lungs - "Cannonball metastases" (large round deposits on CXR) - most common site
- Bones - osteolytic; pathological fractures; bone pain
- Liver
- Brain
- Opposite kidney
- Adrenal gland
Special feature: RCC is famous for late metastases - solitary lung or bone metastases may appear years after nephrectomy. Even then, surgical removal of the metastasis can be curative!
Clinical Features
Classic Triad (seen in only 10% of cases today):
- Painless hematuria (most common presenting symptom, >50% cases)
- Loin/flank pain (dull ache)
- Palpable flank/abdominal mass
Today most RCCs are detected incidentally on imaging done for other reasons.
Other Features:
- Constitutional symptoms: fever, weight loss, malaise, anorexia (advanced disease)
- Varicocele (usually right-sided): sudden-onset, non-reducing varicocele = RCC until proven otherwise (IVC or renal vein obstruction by tumor thrombus prevents drainage of testicular vein)
- Bilateral lower limb edema - IVC thrombus extension
Paraneoplastic Syndromes (PNS) - Very Important!
RCC produces various ectopic hormones - found in up to 1/3 of patients:
| Paraneoplastic Syndrome | Hormone/Mechanism | Frequency |
|---|---|---|
| Elevated ESR | - | Most common PNS |
| Polycythemia (Erythrocytosis) | Ectopic Erythropoietin (EPO) | 5-10% |
| Hypercalcemia | Ectopic PTHrP | Causes confusion, constipation, bone pain |
| Hypertension | Ectopic Renin | Common |
| Cushing syndrome | Ectopic ACTH | Rare |
| Feminization/Masculinization | Ectopic gonadotropins | Rare |
| Stauffer syndrome | Non-metastatic liver dysfunction | Reverses after nephrectomy |
| Anemia | Suppressed erythropoiesis | Common |
PNS may disappear after nephrectomy and return with metastases - a useful marker of recurrence.
Investigations
1. Blood Tests
- CBC: anemia (common) or polycythemia
- ESR: elevated (most common PNS)
- Serum calcium: hypercalcemia (PTHrP)
- LDH: elevated in advanced disease; used for risk stratification
- Liver function tests (ALP elevated = bone/liver metastasis)
- Serum creatinine / eGFR: renal function assessment
2. Urine Tests
- Urinalysis: hematuria (micro or macro)
- Urine cytology: not helpful (unlike TCC/urothelial cancer)
3. Imaging
Ultrasound (USG):
- First investigation for a renal mass
- Differentiates solid from cystic lesion
- Solid enhancement = suspicious for malignancy
CT Abdomen (Triphasic CECT - Gold Standard):
- Investigation of choice for diagnosis AND staging
- Key finding: contrast enhancement >15 Hounsfield Units (HU) = significant; confirms RCC
- Shows: tumor size, local extension, venous involvement, lymph nodes, adrenal glands, opposite kidney
- IVC thrombus is well shown
MRI:
- Superior to CT for assessing IVC thrombus level and vein wall invasion
- Used when CT is contraindicated (e.g., allergy to contrast, pregnancy)
CXR / CT Chest:
- Cannonball metastases on CXR
- CT chest for staging
Bone scan:
- If alkaline phosphatase elevated, bone pain, or hypercalcemia
Staging - TNM Classification
| Stage | Description | 5-Year Survival |
|---|---|---|
| T1a | Tumor ≤4 cm, confined to kidney | ~95% |
| T1b | Tumor 4-7 cm, confined to kidney | ~85% |
| T2 | Tumor >7 cm, confined to kidney | ~70% |
| T3a | Invades renal vein, perinephric fat, renal sinus fat | ~55% |
| T3b | Tumor thrombus in IVC below diaphragm | ~40% |
| T3c | Tumor thrombus in IVC above diaphragm | ~30% |
| T4 | Invades beyond Gerota's fascia (adrenal) | ~20% |
| M1 | Distant metastases | ~10% |
Poor prognostic factors:
- Vein wall invasion (worse than mere tumor thrombus)
- Lymph node involvement
- Sarcomatoid differentiation
- High WHO/ISUP nuclear grade
-
10 cm size
Management
A. Localized Disease (Surgical - Primary Treatment)
1. Radical Nephrectomy (Gold Standard for localized disease)
- Removal of: kidney + Gerota's fascia + perinephric fat + ipsilateral adrenal gland + regional lymph nodes
- Can be done open, laparoscopic, or robotic
- For tumors >7 cm or involving renal sinus
2. Partial Nephrectomy (Nephron-sparing surgery)
- Preferred for tumors <4 cm
- Also indicated for: bilateral tumors, tumor in solitary kidney, renal insufficiency, 4-7 cm well-selected tumors
- Oncological outcomes equal to radical nephrectomy for T1 tumors
3. IVC Thrombectomy
- If tumor thrombus extends into IVC, the thrombus must be surgically removed at the same time as nephrectomy
- May require cardiopulmonary bypass for supradiaphragmatic thrombus
4. Ablative Therapies (for small tumors in high surgical risk patients)
- Radiofrequency ablation (RFA)
- Cryotherapy
B. Metastatic Disease
1. Cytoreductive Nephrectomy
- Removing the primary tumor even in metastatic disease to improve response to systemic therapy
2. Targeted Molecular Therapy (First-line systemic treatment)
Since RCC is relatively resistant to chemotherapy and radiotherapy, targeted therapy is used:
| Drug Class | Examples | Target |
|---|---|---|
| VEGF pathway inhibitors (TKIs) | Sunitinib, Sorafenib, Pazopanib, Axitinib | VEGF receptor |
| mTOR inhibitors | Everolimus, Temsirolimus | mTOR pathway |
| Anti-VEGF antibodies | Bevacizumab | VEGF |
| Immune checkpoint inhibitors | Nivolumab, Pembrolizumab (anti-PD1/PD-L1) | Immune activation |
RCC is one of the few cancers where immunotherapy has worked for decades (old IL-2/IFN-α, now checkpoint inhibitors).
3. Surgery for Solitary Metastasis
- Surgical removal of isolated lung or bone metastases can be curative in selected patients.
4. Radiotherapy
- Not effective against the primary tumor
- Used for palliative treatment of bone or brain metastases
Prognosis Summary
- Organ-confined disease (T1-T2): 70-95% 5-year survival with surgery
- Metastatic disease: 10% 5-year survival
- RCC can have very long latency - metastases can appear 10-20 years after nephrectomy
Key Exam Points (Quick Recall)
| Point | Fact |
|---|---|
| Origin | Proximal renal tubular epithelium (cortex) |
| Most common type | Clear cell (65%); VHL gene mutation |
| Classic triad | Hematuria + flank pain + palpable mass (only 10%) |
| Most common symptom | Painless hematuria |
| Unique spread | Tumor thrombus into renal vein/IVC |
| Cannonball mets | Lung (most common distant site) |
| PNS | Polycythemia (EPO), hypercalcemia (PTHrP), hypertension (renin) |
| Right varicocele | Sudden non-reducing = suspect RCC |
| Gold standard imaging | Triphasic CECT abdomen |
| Gold standard treatment | Radical nephrectomy |
| Nephron-sparing | Tumors <4 cm; partial nephrectomy |
| Resistant to | Conventional chemotherapy & radiotherapy |
| Systemic therapy | TKIs (Sunitinib), mTOR inhibitors, checkpoint inhibitors |
Sources: Bailey & Love's Short Practice of Surgery, 28e; Robbins & Kumar Basic Pathology; Campbell Walsh Wein Urology, 3-Volume Set
This is a shared conversation. Sign in to Orris to start your own chat.