Brain cancer
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"brain tumor" OR "brain neoplasm" classification epidemiology
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
brain cancer types epidemiology incidence 2024 2025 overview
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have enough rich content to deliver a thorough overview. Here it is:
Brain Cancer: Overview
What Is It?
"Brain cancer" covers a broad spectrum of tumors that arise either within the brain itself (primary tumors) or spread there from elsewhere in the body (secondary/metastatic tumors). Primary brain tumors account for only about 2% of all cancers, yet they carry disproportionate morbidity and mortality because of their location.
Epidemiology
-
~93,000 new brain/CNS tumor diagnoses are projected in the US in 2025, including both benign and malignant types (National Brain Tumor Society, 2025).
-
Of these, ~26,000 are malignant primary CNS tumors per year.
-
Malignant incidence rate: ~9 per 100,000 person-years in adults over 40.
-
Childhood rate: ~5.5 per 100,000 - pediatric brain tumors are the #1 childhood cancer by mortality.
-
Incidence rises sharply after age 55.
-
A slight male predominance exists for malignant tumors (7.5 vs. 5.4 per 100,000). However, when benign tumors are included, women have a higher overall rate, largely due to the female predominance of meningiomas.
-
Race: White individuals have higher incidence rates than Black individuals (8.5 vs. 4.8 per 100,000 in males).
-
5-year survival: Overall ~35% for malignant primary brain tumors - the sixth lowest among all cancers. Varies dramatically by subtype (see below).
-
Bradley and Daroff's Neurology in Clinical Practice, Ch. 71
Major Types
Brain tumors are classified by the WHO system (most recently updated in 2021) based on cell of origin, histological grade (I-IV), and increasingly on molecular markers.
1. Primary Brain Tumors
Gliomas (most common malignant primary brain tumor)
Arise from glial cells (astrocytes, oligodendrocytes, ependymal cells). The 2021 WHO Classification now divides them into adult-type and pediatric-type based on molecular genetics.
| Tumor | Key Feature | 5-Year Survival |
|---|---|---|
| Glioblastoma (GBM) | WHO grade IV; IDH-wildtype; most aggressive | ~5.6% |
| Astrocytoma | IDH-mutant; grade II-IV | 30% (anaplastic) |
| Oligodendroglioma | IDH-mutant + 1p/19q co-deletion; slower | ~81.6% |
| Ependymoma | Arises near ventricles | Variable |
GBM accounts for roughly 52% of all brain cancer cases and has a median survival of only 12-18 months even with treatment.
Meningioma (most common primary brain tumor overall, ~35%)
- Arises from the dura mater (meningothelial/arachnoidal cap cells).
- More common in women and with increasing age.
- WHO grades I (benign) to III (malignant).
- Many found incidentally on imaging. Small, asymptomatic ones can be monitored; larger ones are resected.
- Associated with NF2 and prior cranial radiation.
Schwannoma (~9% of primary brain tumors)
- Arises from Schwann cells of cranial nerve roots.
- Most common: vestibular schwannoma (acoustic neuroma), from cranial nerve VIII.
- Generally benign; bilateral in NF2.
Medulloblastoma
- Most common malignant childhood brain tumor.
- Arises in the cerebellum (posterior fossa).
- Associated with Gorlin syndrome and Li-Fraumeni syndrome.
Pituitary Adenoma
- Common, often benign.
- May be functional (e.g., prolactinoma causing amenorrhea/galactorrhea) or non-functional.
2. Metastatic Brain Tumors (Secondary)
- More common than primary malignant brain tumors.
- Most frequent sources: lung, breast, melanoma, kidney, colon.
- Typically multiple lesions; enhance with gadolinium on MRI.
- Serum tumor markers (e.g., beta-hCG for testicular cancer) may be elevated.
Symptoms
Brain tumors produce two broad categories of symptoms (Harrison's Principles of Internal Medicine 22E):
General (from raised intracranial pressure or hydrocephalus):
- Headache - often worse in the morning, may worsen with exertion or position change
- Nausea and vomiting (vomiting preceding headache by weeks is characteristic of posterior fossa tumors)
- Cognitive difficulties, personality change, apathy
- Gait disorder
Focal/Lateralizing (from local tissue disruption):
- Hemiparesis (weakness on one side)
- Aphasia (language difficulty, often mistaken for confusion)
- Visual field defects
- Seizures - occur in ~25% of patients with malignant gliomas or brain metastases; in up to 90% of low-grade glioma patients as the presenting symptom. All brain tumor seizures have a focal onset.
Imaging (Diagnosis)
MRI with gadolinium contrast is the gold standard diagnostic test.
- Malignant tumors (primary or metastatic): typically enhance with gadolinium, show central necrosis, and are surrounded by white matter edema.
- Low-grade gliomas: do NOT typically enhance; best seen on FLAIR sequences.
- Meningiomas: extra-axial, densely enhancing, with a characteristic dural tail.
Below is a post-gadolinium T1 MRI demonstrating multiple meningiomas along the falx and left parietal cortex:
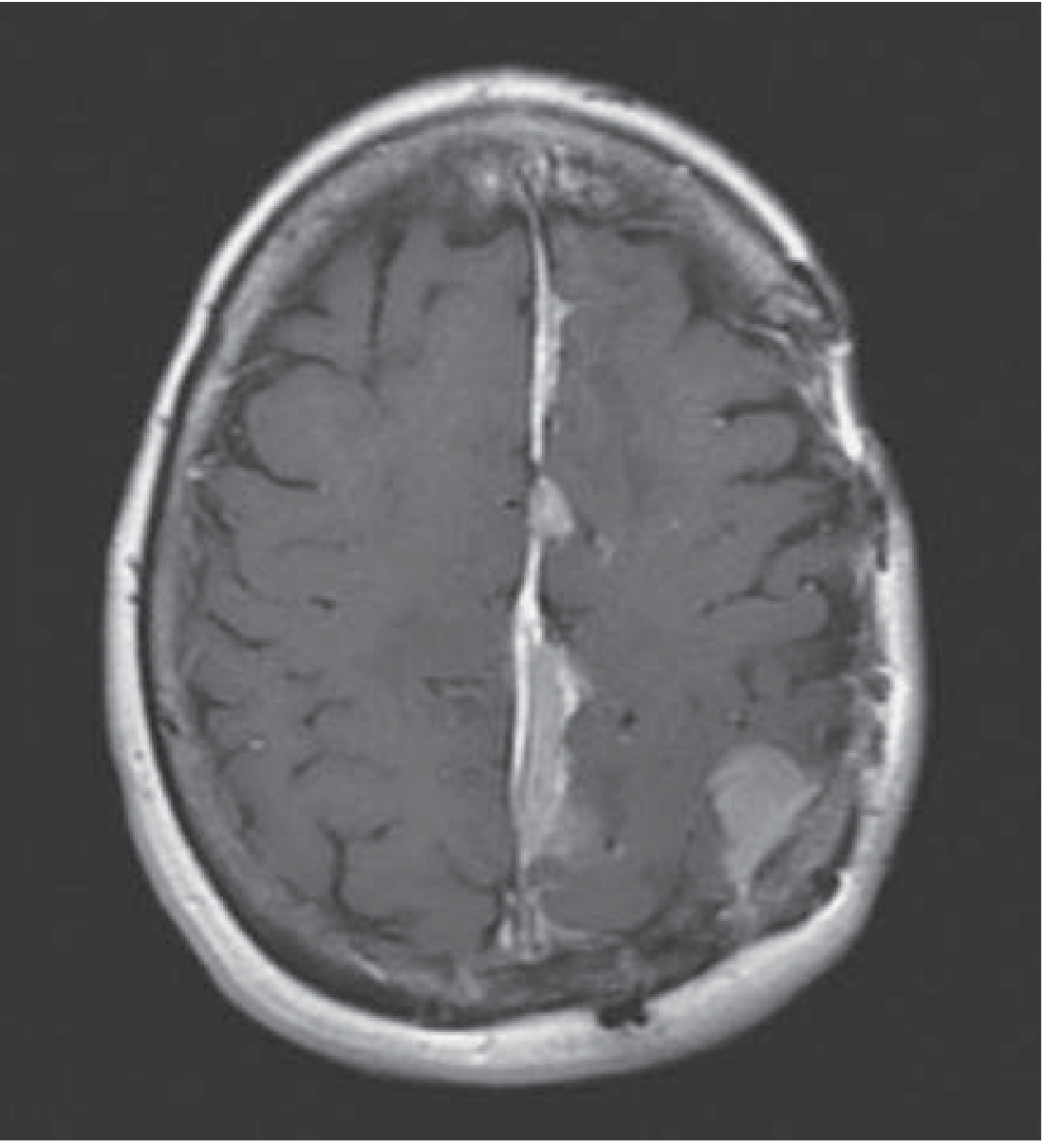
CT is used when MRI is not possible. Additional tools include PET (metabolic activity), MR perfusion/spectroscopy, and functional MRI (presurgical planning for eloquent cortex).
Hereditary / Genetic Risk Syndromes
Some brain tumors arise in the context of inherited syndromes:
| Syndrome | Gene | Associated Brain Tumors |
|---|---|---|
| NF1 | NF1/neurofibromin (chr17) | Optic glioma, astrocytoma |
| NF2 | NF2/merlin (chr22) | Vestibular schwannomas, meningiomas, ependymomas |
| Li-Fraumeni | TP53 (chr17p13) | Gliomas, medulloblastomas |
| Gorlin syndrome | PATCHED1 (chr9q22) | Medulloblastomas |
| Turcot syndrome | APC or hMLH1 | Glioma, medulloblastoma |
| VHL | VHL (chr3p25) | Hemangioblastomas |
Other risk factors include prior cranial irradiation (established) and certain genetic susceptibility loci. Notably, there are no known lifestyle or environmental risk factors that reliably cause brain tumors.
Prognosis by Subtype
| Tumor | 5-Year Survival |
|---|---|
| Oligodendroglioma | ~81.6% |
| Schwannoma/meningioma (gr I) | >90% with complete resection |
| Anaplastic astrocytoma | ~30% |
| Glioblastoma (GBM) | ~5.6% |
Favorable prognostic factors: younger age, lower histological grade, long symptom duration, no cognitive changes at diagnosis, cerebellar location, small tumor, complete surgical resection.
Sources: Harrison's Principles of Internal Medicine 22E, Ch. 95 | Bradley and Daroff's Neurology in Clinical Practice, Ch. 71 | National Brain Tumor Society 2025 | CBTRUS 2025 Fact Sheet
This is a shared conversation. Sign in to Orris to start your own chat.