Pharmacology drug of peptic ulcer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
I now have comprehensive content from Katzung. Let me compile the full answer.
Here is a comprehensive overview of the pharmacology of drugs used in peptic ulcer disease (PUD), based on Katzung's Basic and Clinical Pharmacology (16th edition).
Pharmacology of Drugs for Peptic Ulcer Disease
Peptic ulcer disease results from an imbalance between aggressive factors (acid, pepsin, H. pylori, NSAIDs) and mucosal defense. Drugs target one of two strategies: reducing acid or enhancing mucosal defense.
I. ACID-REDUCING DRUGS
A. Proton Pump Inhibitors (PPIs) - First-Line
PPIs are the most potent acid suppressants and are the cornerstone of PUD treatment.
Drugs: Omeprazole, Esomeprazole, Lansoprazole, Dexlansoprazole, Pantoprazole, Rabeprazole
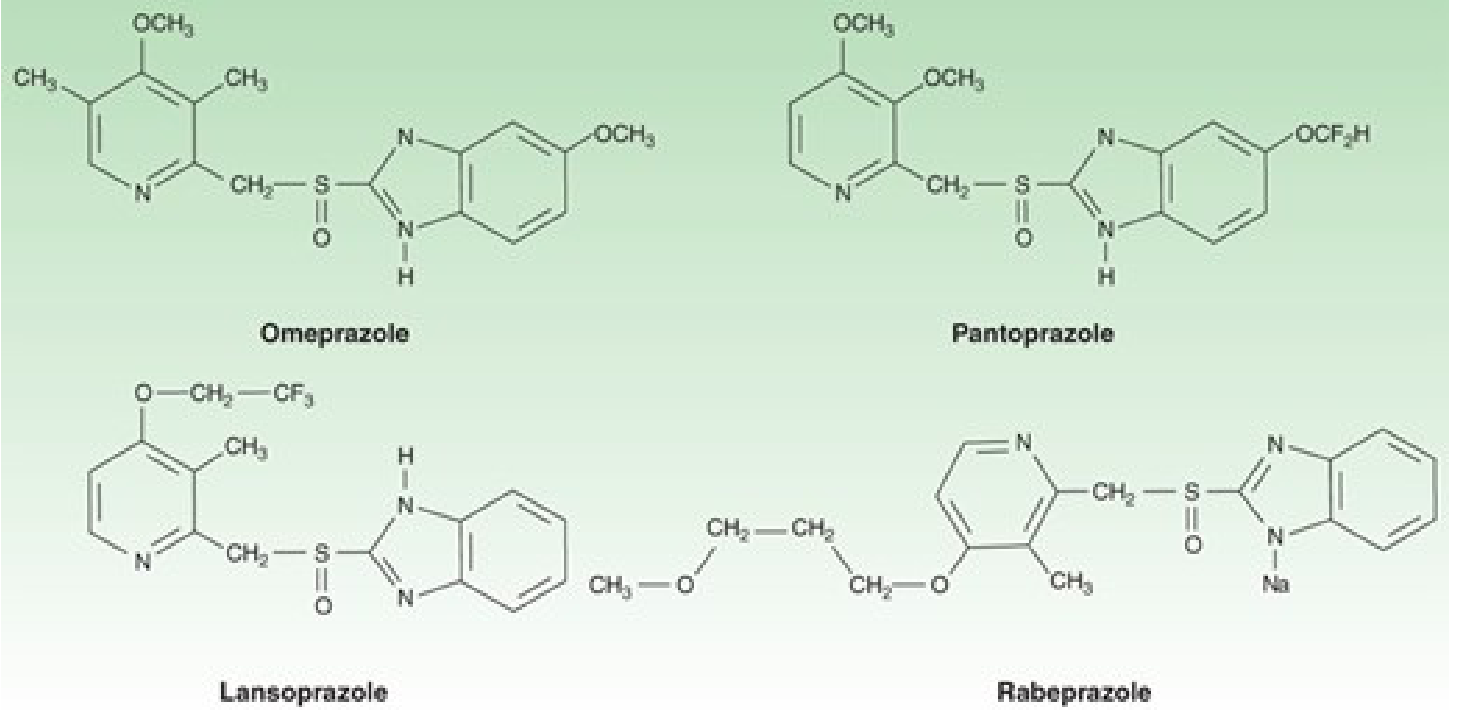
Mechanism of Action
PPIs are prodrugs (substituted benzimidazoles). After oral absorption, they are activated in the acidic canaliculi of the gastric parietal cell, where they form a reactive sulfenamide that covalently and irreversibly binds to H+/K+-ATPase (the proton pump), blocking the final step of acid secretion. Acid secretion resumes only when new pump molecules are synthesized (~18 hours). This makes PPIs more effective than H2 blockers for sustained acid suppression (>90% reduction at steady state).
- Must be taken 30-60 minutes before meals (activate pumps by stimulating acid secretion)
- Full effect takes 2-5 days (not all pumps inactivated on day 1)
Pharmacokinetics (Key Table)
| Drug | Bioavailability | t½ (h) | Usual Dose |
|---|---|---|---|
| Omeprazole | 40-65% | 0.5-1.0 | 20-40 mg once daily |
| Esomeprazole | >80% | 1.5 | 20-40 mg once daily |
| Lansoprazole | >80% | 1.0-2.0 | 30 mg once daily |
| Pantoprazole | 77% | 1.0-1.9 | 40 mg once daily |
| Rabeprazole | 52% | 1.0-2.0 | 20 mg once daily |
Clinical Uses in PUD
- Acute PUD: PPI once daily for 4-8 weeks (faster healing and symptom control than H2 blockers)
- H. pylori eradication: PPI + 2-3 antibiotics (see regimens below)
- NSAID-induced ulcers: PPI once daily promotes healing even if NSAID must be continued
- Prevention of rebleeding: IV bolus (e.g., pantoprazole/esomeprazole 80 mg) + continuous infusion 8 mg/h for 3-5 days to maintain pH >6
- Stress ulcer prophylaxis: Oral PPI preferred when enteral route available
Adverse Effects
- Generally well-tolerated; long-term use may cause:
- Hypomagnesemia, vitamin B12 deficiency, iron malabsorption
- Increased risk of Clostridium difficile infection and community-acquired pneumonia
- Osteoporosis/fractures with prolonged use
- Renal interstitial nephritis (rare)
- Clopidogrel interaction: PPIs (especially omeprazole, esomeprazole) inhibit CYP2C19, reducing clopidogrel activation - prefer pantoprazole or rabeprazole in patients on clopidogrel
B. H2-Receptor Antagonists
Drugs: Cimetidine, Ranitidine (withdrawn in many countries), Famotidine, Nizatidine
Mechanism
Competitive, reversible blockers of H2 receptors on parietal cells, reducing histamine-stimulated acid secretion. Reduce basal and meal-stimulated acid by ~70%.
Clinical Uses
- Mild-moderate PUD (largely replaced by PPIs)
- Short-term use or OTC for dyspepsia/heartburn
- IV H2 blockers for stress ulcer prophylaxis in critically ill patients (continuous infusion preferred over bolus)
Adverse Effects
- Very safe; <3% incidence of headache, diarrhea, fatigue
- Cimetidine - unique effects due to CYP450 inhibition and anti-androgenic activity:
- Gynecomastia and impotence (blocks androgen receptors, raises prolactin)
- Inhibits metabolism of warfarin, phenytoin, theophylline (drug interactions)
- Mental confusion (especially IV, in elderly or renal/hepatic disease)
- Famotidine and nizatidine lack these CYP450 and anti-androgenic effects
C. Antacids
Examples: Aluminum hydroxide, Magnesium hydroxide, Calcium carbonate, Sodium bicarbonate
Mechanism
Neutralize gastric HCl directly (raise intragastric pH). Rapid onset (minutes) but short duration (1-2 hours).
Clinical Uses
- Rapid symptomatic relief (faster than H2 blockers)
- Adjunct therapy; less used as primary PUD treatment today
Adverse Effects
- Aluminum hydroxide: Constipation, phosphate depletion (hypophosphatemia)
- Magnesium hydroxide: Diarrhea; avoid in renal failure (hypermagnesemia)
- Calcium carbonate: "Milk-alkali syndrome" with excess use (hypercalcemia, alkalosis, renal failure); acid rebound
- Sodium bicarbonate: Systemic alkalosis; avoid in hypertension/heart failure
II. MUCOSAL PROTECTIVE AGENTS
A. Sucralfate
Mechanism
A salt of sucrose + sulfated aluminum hydroxide. In acidic conditions, it dissociates to form a highly negative viscous paste that:
- Binds selectively to exposed proteins at the ulcer base (positively charged) - forming a physical barrier up to 6 hours
- Stimulates mucosal prostaglandin and bicarbonate secretion
- Has no significant acid-neutralizing or antisecretory action
Clinical Uses
- 1 g four times daily on an empty stomach (1 hour before meals)
- Stress ulcer prophylaxis in ICU (via NG tube as slurry) - preferred by some because it does NOT raise gastric pH, thus reducing nosocomial pneumonia risk (compared to PPIs/H2 blockers)
Adverse Effects
- Minimal systemic absorption - very safe
- Constipation (2%) from aluminum
- Avoid in chronic renal failure (aluminum accumulation)
- Reduces absorption of fluoroquinolones, tetracyclines, digoxin, warfarin (take 2 hours apart)
B. Misoprostol
Mechanism
A prostaglandin E1 analogue (synthetic). Acts on EP receptors in the gastric mucosa to:
- Inhibit acid secretion
- Stimulate mucus and bicarbonate secretion
- Enhance mucosal blood flow
Clinical Uses
- Prevention of NSAID-induced ulcers (especially in high-risk patients: elderly, prior ulcer, high-dose NSAIDs)
- Given 200 mcg four times daily with food
Adverse Effects
- Diarrhea (most common, dose-dependent; limits compliance)
- Abdominal cramping
- Contraindicated in pregnancy (causes uterine contractions - used medically to induce abortion/labor)
C. Bismuth Compounds
Example: Bismuth subsalicylate (Pepto-Bismol)
Mechanism
- Coats and protects ulcer base
- Direct bactericidal effect against H. pylori
- Stimulates mucus and bicarbonate secretion
- Anti-pepsin activity
Clinical Uses
- Part of bismuth-based quadruple therapy for H. pylori eradication
- Also used for dyspepsia and traveler's diarrhea
Adverse Effects
- Blackening of stools and tongue (harmless bismuth sulfide)
- Salicylate toxicity with overdose
- Bismuth encephalopathy with excessive long-term use
III. H. PYLORI ERADICATION REGIMENS
H. pylori is found in ~70-80% of duodenal ulcers and ~60-70% of gastric ulcers. Eradication is essential for cure and prevention of relapse.
Triple Therapy (14 days) - where clarithromycin resistance is low:
- PPI (twice daily) + Clarithromycin 500 mg BD + Amoxicillin 1 g BD
- (Metronidazole 500 mg BD can replace amoxicillin in penicillin allergy)
Quadruple Therapy (14 days) - first-line in areas of high clarithromycin resistance or prior macrolide exposure:
Option A (Bismuth-based):
- PPI BD + Bismuth subsalicylate 524 mg QID + Metronidazole 500 mg QID + Tetracycline 500 mg QID
Option B (Concomitant):
- PPI BD + Amoxicillin 1 g BD + Clarithromycin 500 mg BD + Metronidazole 500 mg BD
After antibiotics, continue PPI once daily for 4-6 weeks total for ulcer healing.
Confirm eradication with urea breath test or fecal antigen test at least 4 weeks after finishing antibiotics (and 2 weeks after stopping PPI to avoid false negatives).
IV. SUMMARY TABLE
| Drug Class | Examples | Mechanism | Main PUD Use |
|---|---|---|---|
| PPIs | Omeprazole, Pantoprazole | Irreversible H+/K+-ATPase blockade | First-line: H. pylori, NSAID, bleeding ulcers |
| H2 Blockers | Famotidine, Cimetidine | H2 receptor competitive blockade | Mild PUD, stress ulcer prophylaxis |
| Antacids | Mg(OH)2, Al(OH)3 | Neutralize HCl | Symptomatic relief |
| Sucralfate | Sucralfate | Ulcer coating + mucus/HCO3 stimulation | Stress ulcer prophylaxis (ICU) |
| Misoprostol | Misoprostol | PGE1 analogue - inhibit acid, protect mucosa | NSAID ulcer prevention |
| Bismuth | Bismuth subsalicylate | Coat ulcer + anti-H. pylori | Part of quadruple H. pylori therapy |
| Antibiotics | Amoxicillin, Clarithromycin, Metronidazole, Tetracycline | H. pylori eradication | Triple/quadruple therapy |
Source: Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter 62
This is a shared conversation. Sign in to Orris to start your own chat.