Appendicitis incision
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete overview of incisions used for appendicitis (appendicectomy):
Incisions for Appendicitis (Appendicectomy)
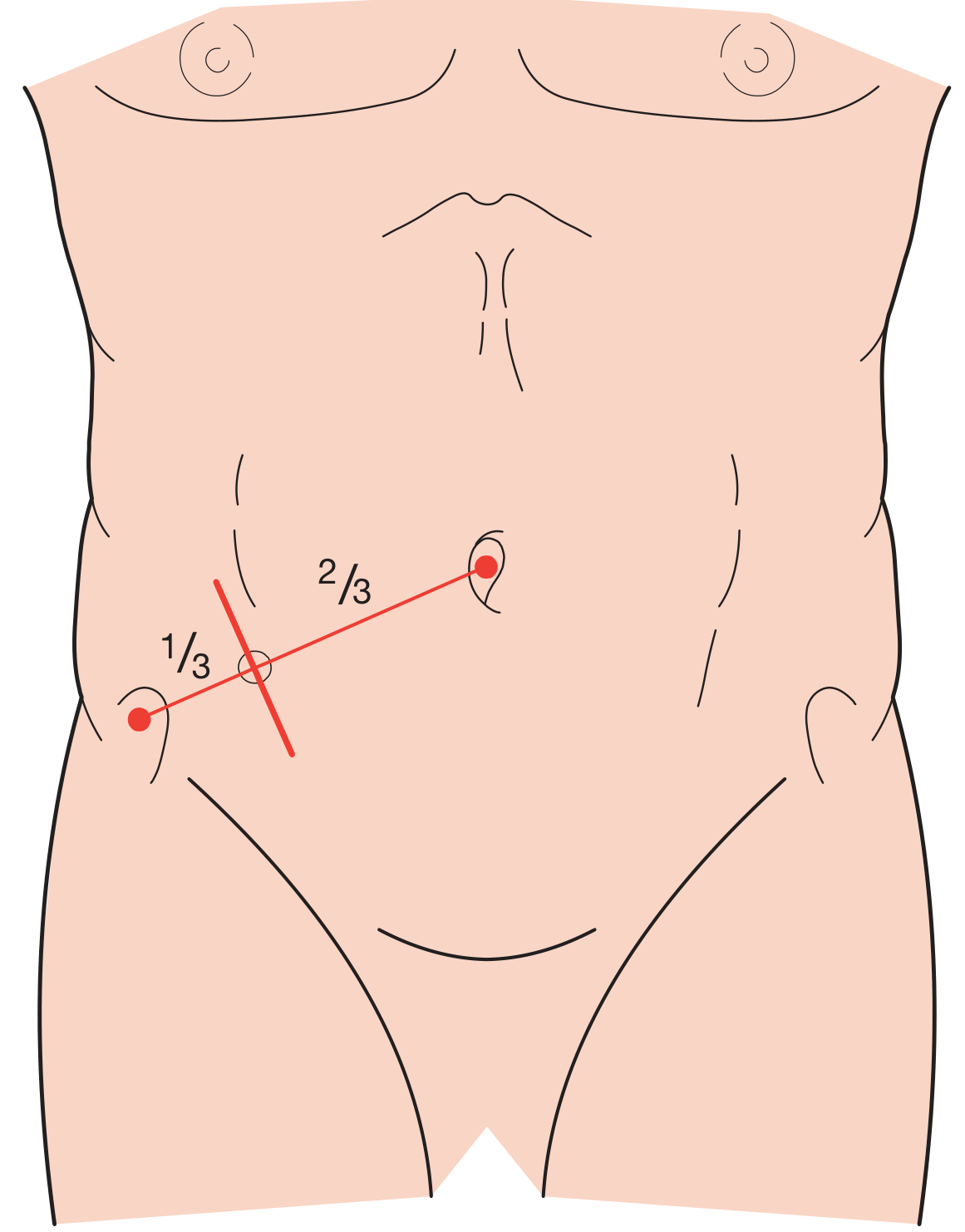
1. Gridiron Incision (McArthur-McBurney Incision) - Most Classic
Position: Made at right angles to a line joining the anterior superior iliac spine (ASIS) to the umbilicus, centred at McBurney's point (the junction of the lateral 1/3 and medial 2/3 of the ASIS-umbilicus line).
Technique: The muscles of the abdominal wall (external oblique, internal oblique, transversus abdominis) are split in the direction of their fibres rather than cut - this is a muscle-splitting approach, which is why it is called a "gridiron."
Extension: If more access is needed, it can be converted to a Rutherford-Morison incision by cutting the internal oblique and transversus in the line of the incision.
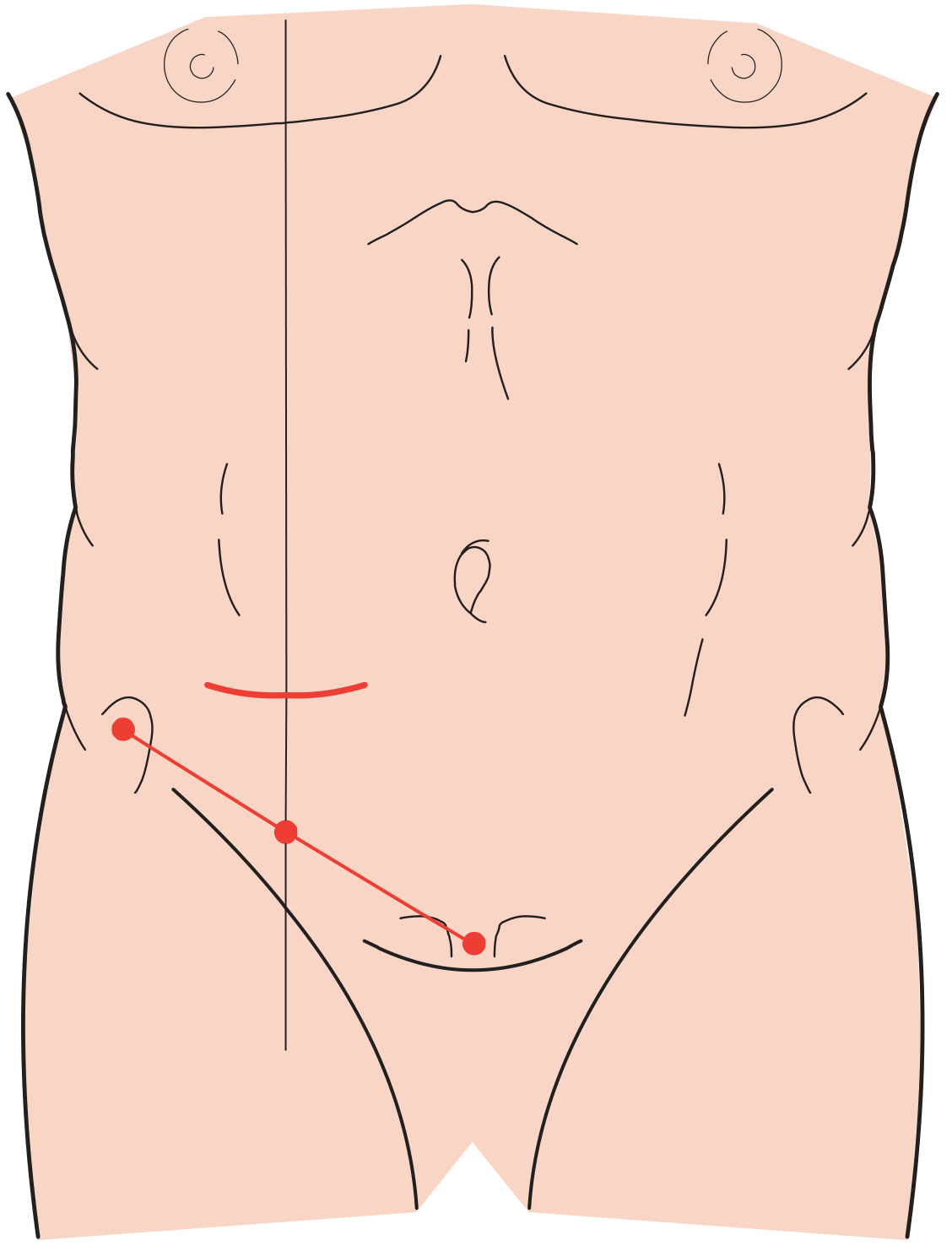
2. Lanz (Transverse/Skin Crease) Incision - Now More Popular
Position: A transverse (horizontal) skin crease incision placed approximately 2 cm below the umbilicus, centred on the midclavicular-midinguinal line.
Advantages: Better cosmesis, better exposure, easier to extend (medially, with retraction or division of the rectus abdominis).
Extension: Can be extended medially toward or through the rectus sheath for greater access.
3. Rocky-Davis Incision
A transverse incision over McBurney's point - essentially a transverse variant of McBurney's approach. Used for open appendectomy, particularly in North American practice (mentioned alongside McBurney's incision in Schwartz's Principles of Surgery).
4. Rutherford-Morison Incision
An oblique muscle-cutting incision with its lower end over McBurney's point, extending obliquely upwards and laterally. All layers are divided in the line of the incision. Used when the appendix is para- or retrocaecal and fixed, requiring greater lateral access.
5. Lower Midline (Laparotomy) Incision
Used when the diagnosis is in doubt, when intestinal obstruction co-exists, or for perforated appendicitis with a phlegmon. Preferred over a right lower paramedian incision because it is easier to extend, easier to close, and gives better access to the pelvis and peritoneal cavity.
6. Laparoscopic Approach (3 Ports)
Not an "incision" per se, but now the preferred approach when expertise and equipment are available:
- Periumbilical port (Hasson technique or optical trocar) for the camera
- Suprapubic port (5 mm)
- Left lower quadrant port (5 mm) - patient in Trendelenburg, left side down
Advantages include lower wound infection rate, faster recovery, and diagnostic benefit (allows inspection of the abdomen before committing to appendicectomy). Conversion to open should be considered for failure to progress.
Summary Table
| Incision | Direction | Location | Use |
|---|---|---|---|
| Gridiron (McArthur) | Oblique, perpendicular to ASIS-umbilicus line | McBurney's point | Standard open appendicectomy |
| Lanz | Transverse (skin crease) | 2 cm below umbilicus, on MCL-MIL | Standard open; better cosmesis |
| Rocky-Davis | Transverse | Over McBurney's point | Open appendicectomy (North America) |
| Rutherford-Morison | Oblique, muscle-cutting | McBurney's point upward laterally | Retrocaecal fixed appendix |
| Lower midline | Vertical midline | Below umbilicus | Uncertain diagnosis, perforation with phlegmon |
| Laparoscopic (3 ports) | - | Umbilical + suprapubic + LLQ | Preferred when expertise available |
Sources: - Bailey and Love's Short Practice of Surgery 28th Ed, pp. 1365-1366 - Schwartz's Principles of Surgery 11th Ed, p. 1363 - Maingot's Abdominal Operations
This is a shared conversation. Sign in to Orris to start your own chat.