Document distal end radius fracture examination
Reading File
Finding Sources
Finding Sources
Searching PubMed
"distal radius fracture" AND examination
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data from multiple authoritative textbooks. Here is the full structured documentation:
Distal End Radius Fracture - Clinical Examination
Overview
Fractures of the distal radius occur within 2-2.5 cm of the articular surface of the radius. They are among the most common fractures in adults, with the classic Colles' fracture being most frequent - especially in postmenopausal women with osteoporotic bone. Several distinct fracture patterns exist, each with characteristic examination findings.
Fracture Types at the Distal Radius
| Fracture | Displacement | Deformity |
|---|---|---|
| Colles' | Dorsal displacement & angulation | "Dinner fork" deformity |
| Smith's (reverse Colles') | Volar displacement & angulation | "Garden spade" deformity |
| Barton's | Volar or dorsal rim fracture-dislocation | Radiocarpal instability |
| Galeazzi | Distal radius + DRUJ dislocation | Radial shortening + DRUJ tenderness |
History
- Mechanism of injury
- Colles': fall on an outstretched hand (FOOSH) with wrist extended - the most common mechanism
- Smith's: fall on dorsum of the hand/wrist, or FOOSH with wrist flexed or in supination shifting to pronation
- Barton's (dorsal): dorsiflexion and pronation force; (volar): FOOSH in supination
- Age and sex: Colles' fracture is most common in postmenopausal women (osteoporotic bone)
- Dominant vs non-dominant hand
- Pre-injury functional status
- Complaints: pain, swelling, deformity at the wrist; palmar paresthesias (median nerve compression)
Inspection
- "Dinner fork deformity" (Colles'): the wrist viewed from the side has a step-like contour due to dorsal displacement and angulation of the distal fragment, resembling the profile of a dinner fork
- "Garden spade deformity" (Smith's): volar/palmar displacement of the distal fragment creates the reverse contour
- Radial deviation of the hand: the wrist deviates toward the radial side, making the distal ulna appear prominent
- Swelling and bruising around the wrist and distal forearm
- Check for open wounds or skin tenting (rare but requires urgent management)
Palpation
- Tenderness directly over the distal radial metaphysis (within 2-2.5 cm of the articular surface)
- Prominent distal ulna: the lower end of the ulna may be unusually prominent due to radial shortening and radial deviation of the hand
- Ulnar styloid tenderness: fracture of the ulnar styloid is common, avulsed by the interarticular disc (triangular fibrocartilage complex - TFCC); this represents disruption of the distal radioulnar joint (DRUJ) and is a frequent cause of long-term morbidity
- DRUJ tenderness: ballottement of the ulnar head; instability at the DRUJ suggests concomitant TFCC injury or Galeazzi pattern
- Scaphoid tenderness in the anatomical snuffbox: exclude a concurrent scaphoid fracture, especially in younger patients
Neurovascular Examination (Critical - Must be Done BEFORE and AFTER Reduction)
Median Nerve (most commonly injured)
- Sensation: assess light touch and two-point discrimination over the palmar aspect of thumb, index, middle, and radial half of ring finger
- Motor: thumb opposition (abductor pollicis brevis) - have the patient touch thumb to little finger against resistance
- Median nerve may be compromised by:
- Contusion
- Traction from displacement
- Transection from fracture fragments
- Nerve compression after closed reduction
- Overlying cast/splint pressure
- Acute carpal tunnel syndrome (ACTS)
- Patients may complain of palmar paresthesias from pressure on the median nerve
Radial and Ulnar Nerves
- Check dorsal hand sensation (radial nerve - first web space) and little finger sensation (ulnar nerve)
- Motor: finger abduction (ulnar nerve intrinsics)
Vascular Assessment
- Radial pulse: compare to contralateral side
- Capillary refill in all fingers
- Assess for hand pallor or blanching
Range of Motion
- Wrist flexion, extension, radial and ulnar deviation - all typically restricted and painful
- Forearm pronation and supination - especially restricted and painful if DRUJ is disrupted
- Finger and thumb motion should be assessed (swelling may limit MCP/PIP movement)
Radiographic Examination
Standard views are PA (posteroanterior) and lateral of the wrist.
PA View
- Distal metaphyseal fracture of the radius
- Radial shortening (the radius should be equal to or longer than the ulna - negative ulnar variance)
- Intraarticular extension into the radiocarpal or radioulnar joints
- Amount of intraarticular step-off
- Associated ulnar styloid fracture (suggests TFCC/DRUJ injury)
- Radial deviation of the distal fragment
Lateral View
- Dorsal angulation and displacement of the distal fragment (Colles')
- Loss of the normal volar tilt of the distal radial articular surface (normal = ~10-11° volar)
- The lateral view provides the best assessment of dorsal comminution
Radiographic Indicators of Instability (Higher-risk features)
- Dorsal angulation >20 degrees
- Intra-articular involvement
- Marked comminution
-
1 cm of radial shortening
- Associated ulnar styloid fracture at its base
Additional Imaging
- CT scan: indicated when significant intra-articular extension or comminution is suspected, or DRUJ instability cannot be fully assessed on plain film
- Ultrasound: handheld US has shown sensitivity of 100% and specificity >90% for diagnosing distal radius fractures in some studies (Rockwood & Green's)
Colles' Fracture X-ray
PA and lateral views of a Colles' fracture showing radial shortening, intraarticular extension, and the classic dorsal angulation:
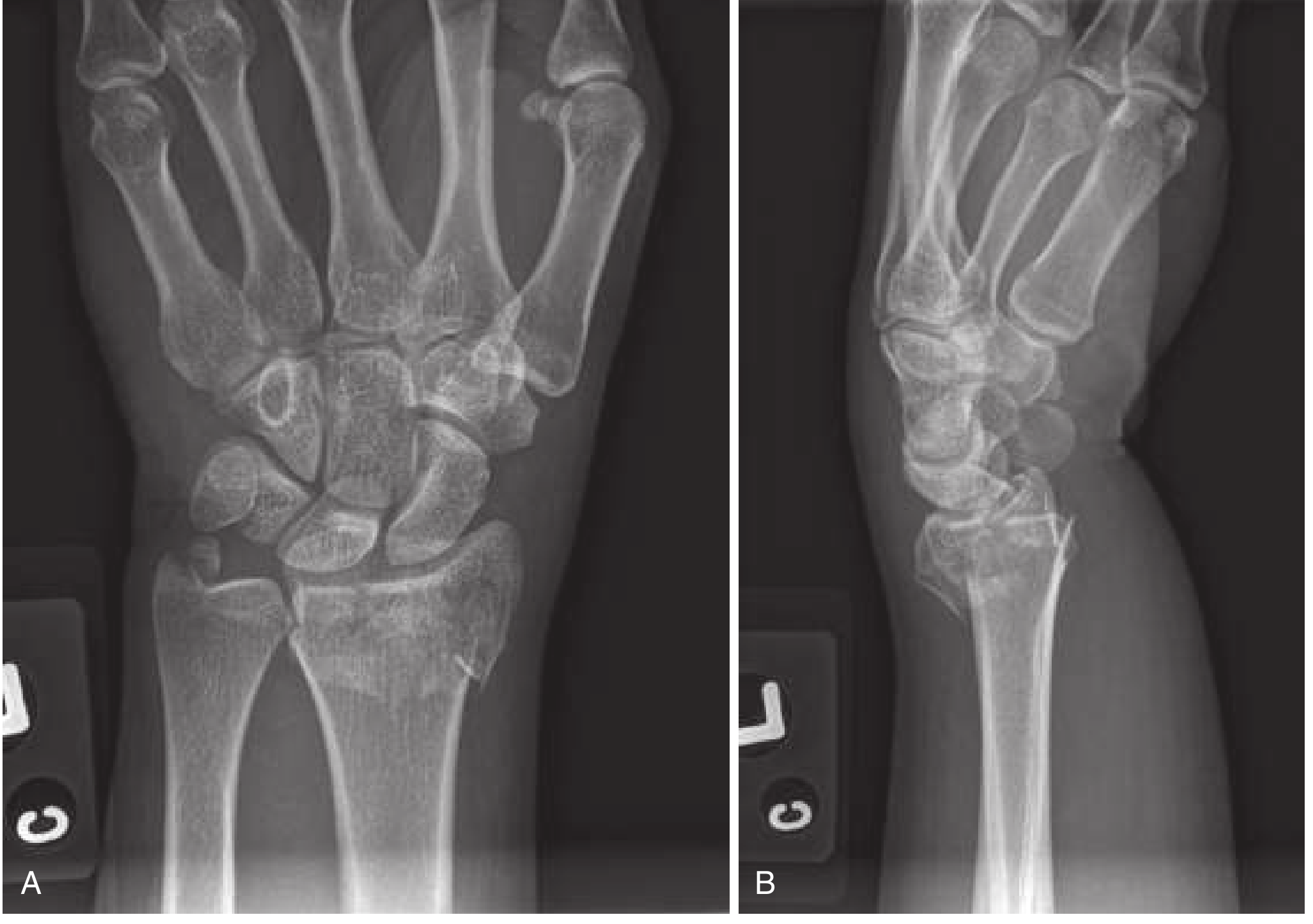
(Fig. 43.24 from Rosen's Emergency Medicine: A - PA view shows fracture and shortening of the radius, intraarticular extension, and associated ulnar styloid fracture; B - Lateral view shows typical dorsal displacement and angulation - the dinner fork deformity)
Associated Injuries to Examine For
| Structure | Assessment |
|---|---|
| Triangular fibrocartilage complex (TFCC) / DRUJ | Ulnar styloid fracture, DRUJ tenderness, forearm rotation pain |
| Median nerve | Thenar sensation, thumb opposition strength |
| Scaphoid | Anatomical snuffbox tenderness (concurrent scaphoid fracture) |
| Carpal ligaments | Scapholunate widening on PA X-ray (Terry Thomas sign) |
| Extensor pollicis longus tendon | At risk of late rupture (assess after healing) |
| Flexor pollicis longus tendon | At risk of late rupture after volar plate fixation |
Documentation Checklist
- Mechanism of injury and hand dominance
- Inspection: deformity type, radial deviation, swelling, skin integrity
- Palpation: fracture site tenderness, distal ulna prominence, ulnar styloid tenderness, DRUJ assessment
- Neurovascular exam (median, radial, ulnar nerve; radial pulse; capillary refill) - documented before and after reduction/splinting
- Range of motion (wrist and forearm)
- PA and lateral X-ray findings: displacement direction, angulation degree, radial shortening, intraarticular extension, ulnar styloid, comminution
- Stability assessment (based on radiographic criteria above)
- Diagnosis: fracture type (Colles', Smith's, Barton's, Galeazzi, intra/extra-articular)
Sources
- Rosen's Emergency Medicine: Concepts and Clinical Practice - Colles Fracture, p. 612
- Tintinalli's Emergency Medicine: A Comprehensive Study - COLLES' FRACTURE, p. 1847-1848; SMITH'S FRACTURE, p. 1848
- Pye's Surgical Handicraft, 22nd Ed. - Colles' fracture, p. 189
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed. - Colles' Fracture, p. 1321
- Campbell's Operative Orthopaedics, 15th Ed. 2026 - Distal Radius Fractures
- Rockwood and Green's Fractures in Adults, 10th Ed. 2025 - Ultrasonography in fracture assessment
This is a shared conversation. Sign in to Orris to start your own chat.