Gastritis carcinoma, it's types, etiology, gross features, treatment management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I have gathered comprehensive information from multiple authoritative sources. Let me now compile the full, detailed response.
Gastric Carcinoma: Types, Etiology, Gross Features, and Treatment
Overview
Gastric carcinoma refers to malignant tumors of the stomach, of which 90% are adenocarcinomas. The remainder includes lymphomas (notably MALT), gastrointestinal stromal tumors (GISTs), neuroendocrine tumors, and rare variants. This review focuses primarily on gastric adenocarcinoma. Gastric cancer is the third most common cause of cancer mortality worldwide, with high-incidence regions including East Asia (China, Korea, Japan), South America (Chile), and Eastern Europe.
- Yamada's Textbook of Gastroenterology, 7th ed.
- Harrison's Principles of Internal Medicine, 22nd ed.
Classification / Types
1. Lauren Classification (1965 - Most Widely Used)
| Feature | Intestinal Type | Diffuse Type | Mixed Type |
|---|---|---|---|
| Differentiation | Well differentiated | Poorly differentiated | Both components |
| Cell arrangement | Glandular structures | Scattered signet ring cells | Mixed |
| Sex predominance | Male > Female | Equal | - |
| Age | Older patients | Younger patients | Intermediate |
| Precursor | Chronic gastritis, intestinal metaplasia | Not associated with gastritis | - |
| Spread | Hematogenous (liver mets) | Transmural/lymphatic (peritoneal mets, linitis plastica) | - |
| Prognosis | More favorable | Worse | Intermediate to poor |
| Epidemiology | Dominant in endemic areas | Not geographically linked | - |
The diffuse type consists of tiny clusters of small, uniform signet ring cells, spreads submucosally, and tends to infiltrate the entire gastric wall producing the classic "leather bottle" appearance (linitis plastica). It has a strong association with blood group A and germline CDH1 mutations (Hereditary Diffuse Gastric Cancer syndrome).
The modified Lauren classification incorporates tumor location (proximal nondiffuse, distal nondiffuse, or diffuse) and better predicts survival than histology alone -- distal nondiffuse having the best prognosis, diffuse type the worst.
- Sabiston Textbook of Surgery, Biological Basis of Modern Surgical Practice
2. WHO Classification (2019)
Five main subtypes:
- Tubular adenocarcinoma - Most common (45-64%); corresponds to Lauren intestinal type
- Papillary adenocarcinoma - Rare (2.7-9.9%); well-differentiated but higher liver metastasis rate and poor survival
- Poorly cohesive adenocarcinoma (including signet ring cell carcinoma) - 20-54% of cases; corresponds to Lauren diffuse type; lower sensitivity to chemoradiotherapy
- Mucinous adenocarcinoma - Rare (2.1-8.1%); glandular structures with interstitial mucin or nests of signet ring cells surrounded by mucin
- Mixed-pattern adenocarcinoma - 6-22%; contains both glandular and signet ring cell components; poorer prognosis than single-component tumors
Additional rare subtypes include: adenocarcinoma with lymphoid stroma (EBV-positive, good prognosis), hepatoid adenocarcinoma, micropapillary adenocarcinoma, and gastric adenocarcinoma of fundic gland type (very good prognosis).
- Yamada's Textbook of Gastroenterology, 7th ed.
3. TCGA Molecular Classification (2014)
Four subtypes based on transcriptomic/proteomic profiling:
| Subtype | Characteristics |
|---|---|
| EBV-positive | EBV infection; associated with lymphoid stroma variant; good prognosis |
| MSI (Microsatellite Instability) | High mutation burden; responds to immunotherapy (PD-1 inhibitors) |
| Genomically Stable (GS) | Enriched for diffuse type; CDH1 mutations |
| Chromosomal Instability (CIN) | Most common; TP53 mutations; HER2 amplification common |
This classification has therapeutic significance -- MSI-high tumors respond well to checkpoint inhibitors, and CIN tumors with HER2 amplification respond to trastuzumab.
- Sabiston Textbook of Surgery
Etiology and Risk Factors
Environmental / Acquired Factors
-
H. pylori infection: The most important modifiable risk factor. ~50% of all humans are infected, but only a small subset develop cancer. High-risk strains drive intestinal metaplasia via the Correa cascade (normal mucosa → chronic gastritis → atrophic gastritis → intestinal metaplasia → dysplasia → carcinoma). H. pylori eradication significantly reduces gastric cancer risk, supported by RCT evidence.
-
Diet: High intake of nitrates from dried, smoked, and salted foods. Refrigeration (since 1920s) has correlated with decreased incidence in Western countries.
-
EBV (Epstein-Barr Virus): Associated with a distinct subtype (~10% of all gastric cancers); characterized by dense lymphoid stroma and good prognosis.
-
Chronic inflammation / atrophic gastritis: Especially autoimmune gastritis causing achlorhydria.
-
Obesity and acid reflux: Promotes adenocarcinoma of the gastroesophageal junction (GEJ) -- incidence of proximal/GEJ cancers has been rising in Western high-HDI countries even as distal cancers decline.
-
Gastric microbiome: Gastric cancer patients show higher overall bacterial load; the spectrum beyond H. pylori may contribute.
-
Harrison's Principles of Internal Medicine, 22nd ed.
Genetic / Hereditary Factors
| Syndrome/Gene | Risk |
|---|---|
| CDH1 mutation (HDGC) | Markedly increased risk for diffuse/signet ring cell type; also lobular breast cancer |
| Lynch syndrome | MSI-high gastric cancer; responds to immunotherapy |
| FAP (APC gene) | Fundic/body polyps, GAPPS variant; upper GI surveillance required |
| GAPPS | >100 polyps carpeting gastric fundus/body; can progress to cancer |
| Peutz-Jeghers / Juvenile Polyposis | EGD surveillance from teenage years |
| TP53 / KRAS | Common somatic mutations across multiple cancer types |
| HER2 (ERBB2) | Amplification/overexpression predicts response to trastuzumab |
Prophylactic total gastrectomy is recommended for medically fit carriers of germline CDH1 mutations, typically between ages 20-30.
- Sabiston Textbook of Surgery, Harrison's Principles of Internal Medicine
Gross Features: Borrmann Classification (1926)
This system classifies advanced gastric adenocarcinoma by macroscopic/endoscopic appearance:
| Type | Gross Description | Notes |
|---|---|---|
| Type I | Polypoid / fungating | Localized; best prognosis |
| Type II | Ulcerative with elevated, distinct, well-defined borders | Localized |
| Type III | Ulcerative with indistinct, infiltrating borders | Infiltrative |
| Type IV | Diffusely infiltrating (linitis plastica) | Entire gastric wall involved by infiltrating signet ring cells; "leather bottle" stomach; worst prognosis |
Types I and II are localized; Types III and IV are infiltrative. The Borrmann type is a valuable predictor of survival in advanced gastric cancer, particularly for stage III patients undergoing curative resection.
Linitis plastica (Type IV) is the classic gross appearance of the diffuse type -- the stomach becomes rigid, thickened, and shrunken due to transmural infiltration by poorly cohesive tumor cells mixed with a desmoplastic stromal reaction.
- Yamada's Textbook of Gastroenterology, Sabiston Textbook of Surgery
Histology of intestinal-type gastric adenocarcinoma (H&E):
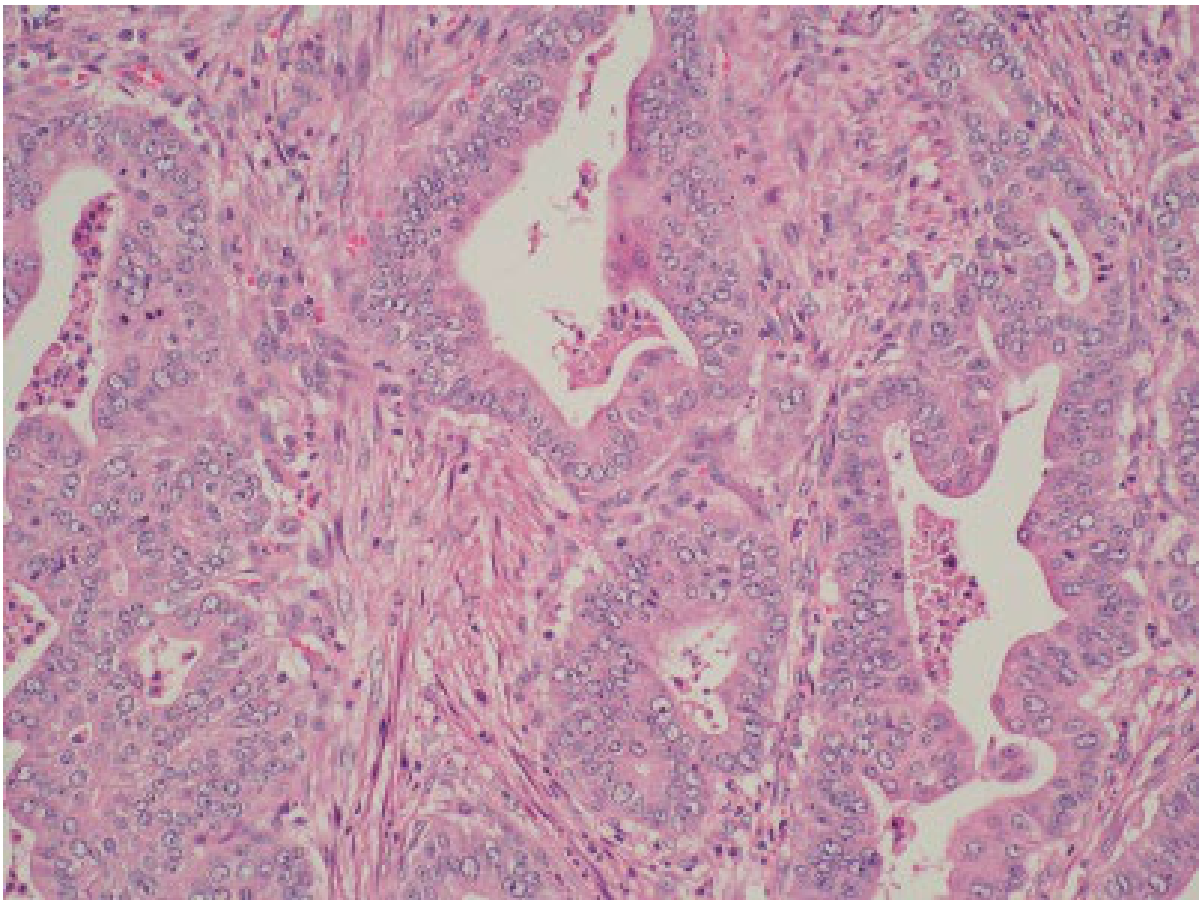
Intestinal type gastric adenocarcinoma: glandular-like structures within a fibrous desmoplastic stroma. (Courtesy Prof. Graeme Murray, Aberdeen University -- from Yamada's Textbook of Gastroenterology)
Early gastric cancer (EGC) on endoscopy:
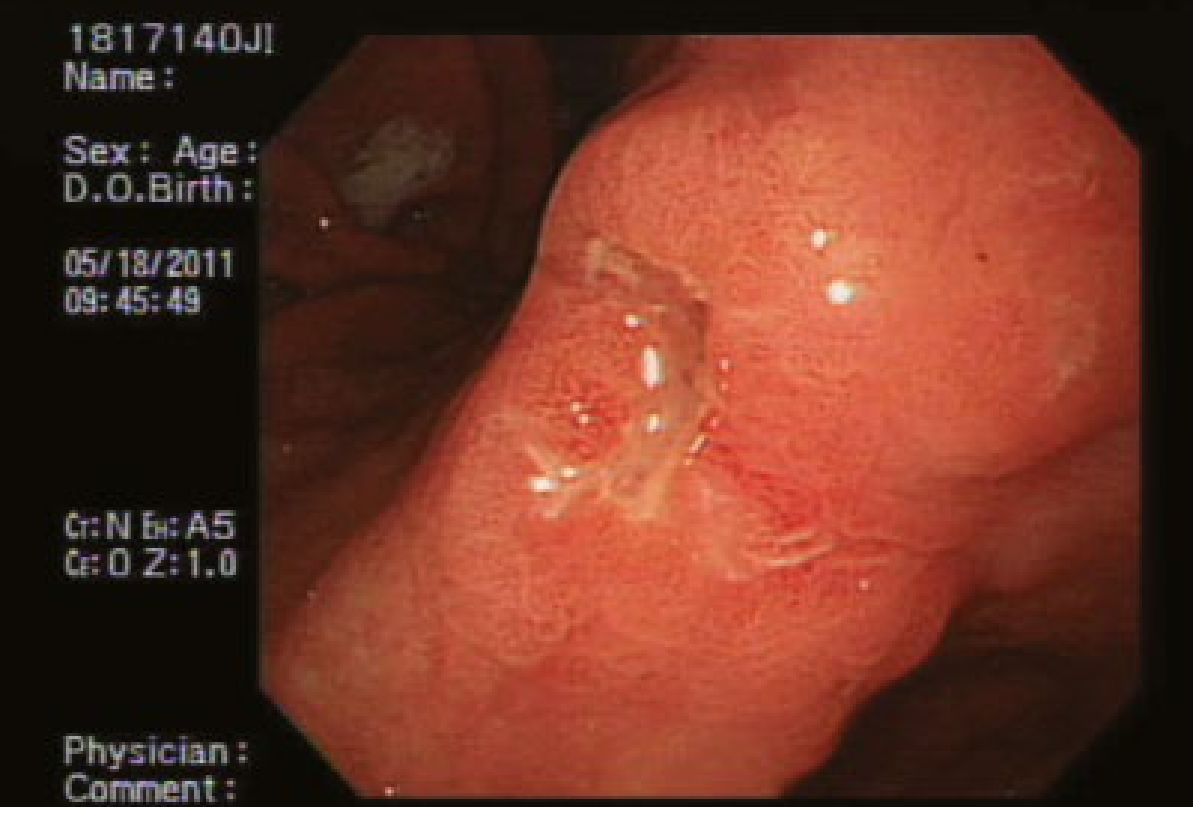
Endoscopic view of early gastric cancer: uneven elevated mucosal patch over the angularis with some healing ulcers. (From Yamada's Textbook of Gastroenterology)
Early vs Advanced Gastric Cancer
- Early gastric cancer (EGC): Confined to mucosa or submucosa regardless of lymph node status; associated with high cure rates.
- Advanced gastric cancer: Invades muscularis propria or beyond. In Western countries, ~75% of patients present with perigastric lymph node spread or distant metastases at diagnosis.
Japanese classification of EGC (based on endoscopic morphology):
- Type I: Protruding
- Type IIa: Superficially elevated
- Type IIb: Flat
- Type IIc: Superficially depressed
- Type III: Excavated
Treatment Management
A. Early Gastric Cancer (EGC)
Endoscopic Resection (preferred for select EGC):
- Endoscopic mucosal resection (EMR): For non-ulcerated lesions confined to mucosa
- Endoscopic submucosal dissection (ESD): Preferred for larger or ulcerated EGC; allows en bloc resection
- Japanese expanded ESD criteria: (1) Mucosal intestinal-type of any size without ulceration; (2) Mucosal intestinal-type <3 cm with ulceration; (3) Submucosal intestinal-type <3 cm with submucosal invasion <500 μm
- En bloc resection rates >90%; local recurrence <3%
- Risk of perforation ~2-6% (managed conservatively with clips)
Surgical Resection: Standard for EGC not meeting endoscopic criteria or with lymph node involvement.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
B. Resectable / Locally Advanced Gastric Cancer - Surgery
- Subtotal gastrectomy: For distal tumors
- Total gastrectomy: For proximal tumors or diffuse-type disease
- Lymphadenectomy extent (JGCA definitions):
- D1: Perigastric nodes only
- D1+: D1 + selected regional nodes
- D2: Extended nodal dissection (recommended by NCCN for experienced centers)
- NCCN recommends modified D2 (without routine distal pancreatectomy or splenectomy) to reduce morbidity while maintaining survival benefit
- Minimum 16 lymph nodes recommended for pathologic analysis; >30 is desirable
A Cochrane meta-analysis found improved disease-specific survival with D2 vs D1, but higher perioperative morbidity -- largely related to concurrent pancreatectomy/splenectomy in older trials.
- Sabiston Textbook of Surgery
C. Perioperative Chemotherapy (Standard of Care for Resectable Disease)
MAGIC Trial: Perioperative ECF (epirubicin + cisplatin + 5-fluorouracil) significantly improved 5-year survival (36% vs 23%) compared to surgery alone.
FLOT4-A10 Trial: FLOT (docetaxel + oxaliplatin + fluorouracil/leucovorin) perioperatively significantly improved OS and PFS vs ECF/ECX -- FLOT is now the preferred perioperative regimen for resectable gastric and GEJ adenocarcinoma.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
D. Adjuvant Chemoradiation
The Intergroup Trial 0116 randomized 603 patients: surgery + adjuvant 5-FU/leucovorin/radiation vs surgery alone. The chemoradiation group had significantly better OS (median 36 vs 27 months) and relapse-free survival. This established adjuvant chemoradiation as a standard of care in the USA.
E. Targeted Therapy and Immunotherapy
| Target | Agent | Indication |
|---|---|---|
| HER2 (ERBB2) | Trastuzumab | HER2-overexpressing advanced/metastatic gastric cancer (first-line with chemotherapy) |
| PD-1 | Nivolumab | PD-L1+ advanced gastric/GEJ cancer - improved OS in combination with chemotherapy (CheckMate 649) |
| VEGFR2 | Ramucirumab | Second-line metastatic gastric cancer |
| MSI-H | Pembrolizumab | MSI-high / dMMR tumors; immunotherapy preferred over cytotoxic chemo (Lynch syndrome-associated) |
- Current Surgical Therapy, 14th ed., Sabiston Textbook of Surgery
F. Intraperitoneal (IP) Chemotherapy
- HIPEC (Hyperthermic Intraperitoneal Chemotherapy): Used for patients with peritoneal metastases or high-risk of microscopic peritoneal residual after resection. Meta-analysis shows significantly reduced risk of death (OR 0.60) vs surgery alone. Most benefit in stage III-IV with serosal invasion or lymph node metastases.
G. Palliative Treatment (Advanced / Unresectable Disease)
-
Debulking surgery
-
Bypass procedures for gastric outlet obstruction
-
Endoscopic laser therapy or alcohol injection for tumor debulking
-
Endoscopic stenting
-
Systemic chemotherapy (FLOT, FOLFOX, XP/XELOX regimens)
-
Best supportive care
-
Yamada's Textbook of Gastroenterology
H. Prevention
- H. pylori eradication in high-risk individuals (first-degree relatives of gastric cancer patients, prior early-stage gastric cancer) - reduces subsequent cancer incidence
- Prophylactic gastrectomy for CDH1 germline mutation carriers
- Surveillance endoscopy with Cambridge/Bethesda protocol biopsies for those declining prophylactic gastrectomy (HDGC)
- Dietary modification: reduce smoked, salted, nitrate-rich foods; increase fresh fruits and vegetables
Summary at a Glance
| Aspect | Key Points |
|---|---|
| Most common type | Adenocarcinoma (90%) |
| Lauren classification | Intestinal (glandular, better prognosis) vs Diffuse (signet ring, linitis plastica, worse prognosis) |
| Borrmann gross types | I Polypoid, II Ulcerative clean borders, III Ulcerative infiltrating, IV Linitis plastica |
| Main etiology | H. pylori, diet (nitrates), EBV, CDH1 mutation, Lynch syndrome |
| Treatment backbone | Perioperative FLOT + surgery + D2 lymphadenectomy |
| Targeted therapy | Trastuzumab (HER2+), Nivolumab/Pembrolizumab (PD-L1+/MSI-H) |
| EGC endoscopic Rx | ESD (preferred) or EMR |
Sources: Sabiston Textbook of Surgery (Biological Basis of Modern Surgical Practice) | Yamada's Textbook of Gastroenterology, 7th ed. | Harrison's Principles of Internal Medicine, 22nd ed. | Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Current Surgical Therapy, 14th ed.
This is a shared conversation. Sign in to Orris to start your own chat.