Maxillary and mandibular fractures in detail according to standard Ent textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive, textbook-quality response. Let me compile it:
Maxillary and Mandibular Fractures
Based on Cummings Otolaryngology Head and Neck Surgery, Scott-Brown's Otorhinolaryngology Head & Neck Surgery, and K.J. Lee's Essential Otolaryngology
PART I: MAXILLARY (MIDFACIAL) FRACTURES
Surgical Anatomy
The bone of the midfacial region is generally very thin and offers little resistance to anterior and lateral forces. The midfacial skeleton is divided into lateral (zygomatic) and central (maxillary, nasal, nasoorbito-ethmoid) fractures. The classical features of any midfacial fracture include:
- Circumorbital ecchymosis ("panda facies")
- Facial oedema and surgical emphysema
- Lengthening of the face
- Anterior open bite
- Infraorbital nerve sensory deficit (in higher fractures)
- Bruising at the junction of the hard and soft palate
Not all these signs need be present simultaneously.
(Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1)
Le Fort Classification
The Le Fort system, described over 100 years ago by René Le Fort, remains the cornerstone classification of maxillary fractures. Le Fort originally developed it by analyzing fracture patterns in cadavers traumatized by being dropped from a height. All three levels share two common features: fracture of the nasal septum and fracture of the pterygoid plates.
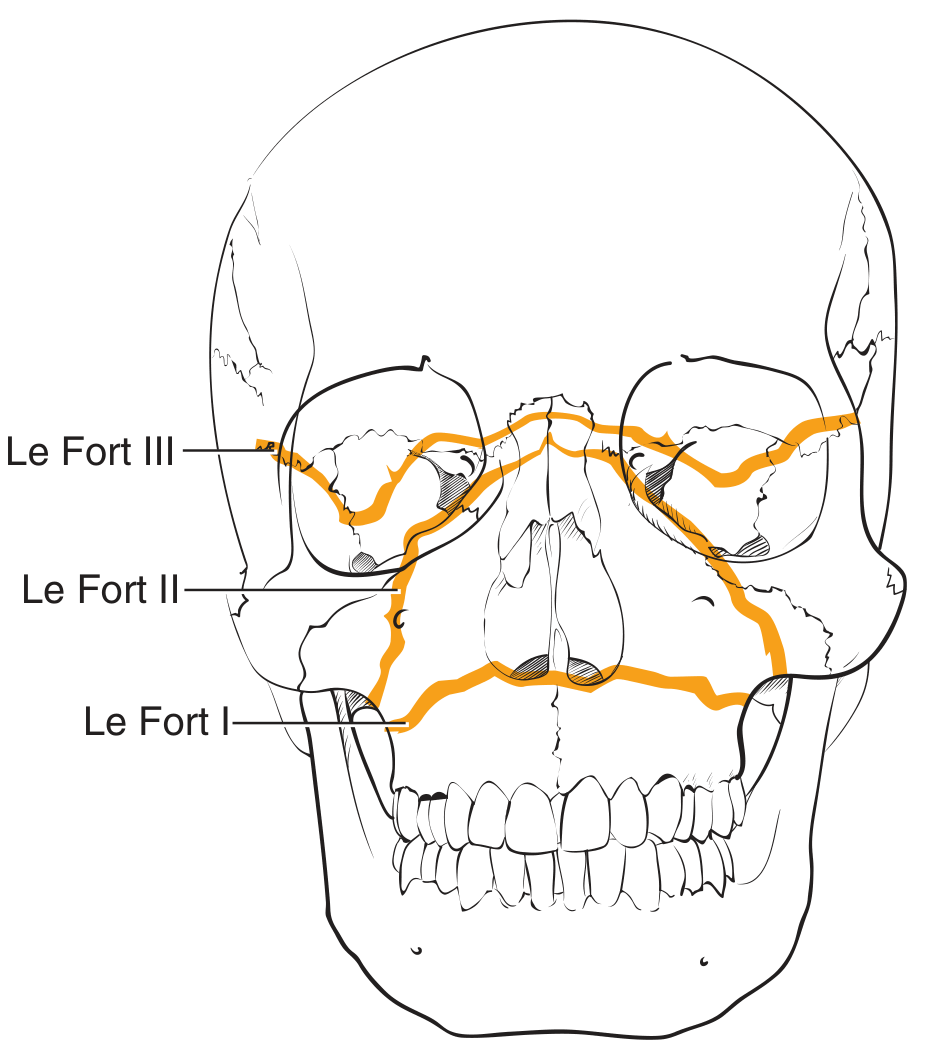
Le Fort fracture lines (Cummings Otolaryngology)
Le Fort I (Horizontal / Guérin's Fracture)
- Fracture line runs above the level of the maxillary dentition, above the floor of the nasal cavity
- Separates the alveolus and teeth from the remaining craniofacial skeleton
- Crosses through: nasal septum, maxillary sinuses, inferior parts of the medial and lateral pterygoid plates, and posterior maxillary walls
- The mobile segment contains the upper teeth and hard palate
- Results in a mobile hard palate on examination
Le Fort II (Pyramidal Fracture)
- A pyramid-shaped inferior facial segment is separated from the craniofacial skeleton
- Fracture starts at the zygomaticomaxillary buttress on one side, travels superomedially, fractures the inferior orbital rim and orbital floor, traverses the medial orbit, crosses the midline at the nasal root or through the nasal bones, then travels inferolaterally on the contralateral side
- Like Le Fort I, it fractures the nasal septum, posterior maxillary walls, and pterygoid plates
- May result in infraorbital nerve anaesthesia
- The entire central face (nose + maxilla) is mobile as one unit
Le Fort III (Craniofacial Separation / Craniofacial Dysjunction)
- True separation at the level of the skull base
- Separates the zygomas from the temporal and frontal bones
- Fracture crosses the lateral orbits and medial orbits, reaches the midline at the nasofrontal junction, violates the nasal septum and pterygoid plates
- The entire midface (including both zygomas) is separated from the skull
- Clinically: the entire face is mobile as one unit - "floating face"
- Dish-face deformity
Clinical note: Pure Le Fort III fractures are probably rare in practice. Most surgeons describe an injury by the most severe Le Fort level and then enumerate additional components. Many high-energy maxillary fractures are not pure Le Fort injuries and are also comminuted. (Cummings Otolaryngology)
Clinical Signs and Symptoms of Maxillary Fractures
| Feature | Details |
|---|---|
| Epistaxis | Due to disruption of mucosal lining |
| Circumorbital ecchymosis | "Panda eyes" - typical of Le Fort II/III |
| Facial oedema | Generalised swelling |
| Surgical emphysema | Air in soft tissue planes |
| Lengthening of the face | Downward displacement of midface |
| Anterior open bite | Posterior impaction of maxilla |
| Infraorbital anaesthesia | Injury to infraorbital nerve (Le Fort II/III) |
| Palatal bruising | At hard/soft palate junction |
Imaging
- Axial CT is excellent for demonstrating displacement of maxillary fractures and showing fractures through the pterygoid plates (helps define Le Fort type)
- Coronal CT is best for the horizontal components of Le Fort fractures
- 3D CT reconstruction is particularly helpful for complex midfacial and NOE fractures
- Plain radiographs may miss many details and are largely supplemented or replaced by CT in current practice
(Cummings Otolaryngology)
Management of Maxillary Fractures
Emergency Treatment
Midfacial fractures can easily compromise the airway due to:
- Torrential epistaxis
- Posterior impaction of the maxilla
Emergency measures:
- Bleeding arrested with anterior and posterior nasal packs or epistats
- If retroposition of the maxilla is a problem, it can be pulled forwards with the index and middle fingers placed behind the patient's soft palate
- Consider tracheostomy at the outset in patients with extensive trauma
Antibiotic Prophylaxis
Because maxillofacial injuries communicate with the nose, sinuses, and oral cavity, they are considered contaminated. Antibiotics covering oral organisms (penicillins, cephalosporins, or clindamycin) are initiated when the patient presents and are given for at least 24 hours post-surgery.
Reduction
- The maxilla is mobilized by a combination of digital pressure and traction on arch bars or interdental wires
- Position is confirmed with reference to bony buttresses and dental occlusion
- Rowe's maxillary disimpaction forceps can be invaluable if the maxilla is impacted
Fixation
Modern management uses internal fixation with 1.3 or 1.5 mm low-profile miniplates placed along the buttresses:
- Provides satisfactory stabilization with early mobilization
- Access via gingivobuccal incision (posterior limit no further than first permanent molar to preserve blood supply)
- Buccal fat pad avoided by angling scalpel at 45° to the gingival cuff
- Subperiosteal elevation with preservation of the infraorbital nerve allows reconstruction of paranasal and zygomatic buttresses
- In Le Fort II fractures: infraorbital rim needs separate reduction and fixation
- Internal fixation has replaced external fixation for the majority of maxillary fractures
(Scott-Brown's, Cummings Otolaryngology)
PART II: MANDIBULAR FRACTURES
Introduction and Surgical Anatomy
The mandible is a parabolic-shaped bone with complex articulations - the paired temporomandibular joints (TMJ) - and movements guided by dental occlusion. Satisfactory rehabilitation requires accurate reduction, adequate fixation, and mobilization.
The mandible fractures at points of anatomical weakness:
- Angle - weakened by unerupted wisdom teeth
- Parasymphysis - weakened by the long root of the lower canine
- Condylar neck - weakened by its slender anatomy
The mandible commonly fractures in more than one place - for example, at the parasymphysis (site of direct violence) and the condylar neck (site of indirect violence) simultaneously.

Lines of weakness in the mandible (Scott-Brown's Otorhinolaryngology)
Classification
Mandibular fractures are classified by:
-
Anatomic region (most commonly used):
- Condylar / subcondylar
- Coronoid
- Ramus
- Angle
- Body
- Parasymphysis
- Symphysis
- Alveolar
-
Severity:
- Simple (linear)
- Comminuted
- Avulsive (bone loss)
-
Dentition status:
- Dentulous
- Edentulous
- Atrophic edentulous
The traditional classification of "favorable" vs "unfavorable" fractures is no longer considered helpful in determining treatment and is of historical significance only. (Cummings Otolaryngology)
Signs and Symptoms
Fractures of the Body, Angle, and Symphysis
- Step deformity palpable externally or intraorally
- Asymmetry of the lower dental arch and derangement of occlusion
- Pain, paradoxical movement, and crepitus on distraction of fractured segments
- Haematomas in the buccal sulcus or floor of the mouth
- Blood-stained saliva
- Mobile teeth in the fracture line
- Anaesthesia of the lower lip and chin (mental nerve distribution)
- Trismus
Fractures of the Condylar Neck
- Tenderness over the TMJ
- Trismus
- Deviation of the jaw toward the injured side on opening (lateral pterygoid pull unopposed)
- Inability to move the mandible to the side opposite the fracture
- Anterior open bite (bilateral condylar neck fractures - symmetrical)
- Deviation to the fractured side at rest with anterior open bite (fracture-dislocation - "gagging" on molar teeth)
- Contralateral premature contact and ipsilateral open bite (unilateral fracture-dislocation)
Key principle: Always look for a second mandibular fracture, as contralateral fractures are common. Record the presence or absence of paraesthesia in the mental nerve distribution. (Bailey & Love's; Scott-Brown's)
Imaging
- Orthopantomogram (OPG/Panorex) is the most widely used and preferred initial investigation - provides an overview of the entire mandible
- Plain mandibular series (PA mandible, lateral obliques) supplement the OPG
- High-resolution helical CT (1-mm slices) has 100% sensitivity vs 86% for OPG alone (Lee, Cummings); particularly indicated for:
- Complex or comminuted fractures
- Condylar fractures (3D reconstruction recommended for condylar position)
- Post-operative assessment of reduction
- CT may miss posterior mandibular fractures, so both OPG + CT are used to maximize information
Biomechanics Relevant to Treatment
The mandible experiences both tension (superior/alveolar surface during bending) and compression (inferior border). This determines plate placement:
- Tension band plate placed along the superior surface (near the alveolus) resists the distracting forces
- Compression plate at the inferior border neutralizes compressive forces
- In simple fractures, monocortical 2 mm plates provide adequate fixation through load-sharing
- In anterior mandible: two plates are used
- Posteriorly: one plate is usually sufficient; 6 mm screws are standard
(Scott-Brown's, Cummings)
Management
General Principles
- Antibiotic prophylaxis (oral flora coverage) started at presentation
- Timing of surgery: once life-threatening injuries are stabilized; no significant benefit of delay beyond 2-3 weeks
- Dental occlusion is the primary functional goal - must be restored precisely
Intermaxillary Fixation (IMF) / Maxillomandibular Fixation (MMF)
IMF has a much smaller role in modern practice but remains relevant in:
- Undisplaced fractures with no neural deficits (conservative management)
- Unilateral condylar fractures
- As a temporary measure before ORIF
- Emergency room: tie wire placed around teeth either side of displaced fracture reduces pain and bleeding while awaiting ORIF
Methods of IMF:
- Eyelet wires - simple, for intact dental arch
- Leonard button - modification with metal disc, facilitates elastic traction
- Arch bars (Erich arch bar) - pliable metal bands wired to each jaw; allow elastic training bands; most widely used in the USA
- Ivy loops - stabilize a few teeth only; do not provide tension banding across the arch
- Intermaxillary bone pins/screws - rapid method using monocortical screws between canine and first premolar; advantage of speed, disadvantage of frequent tooth root penetration
Open Reduction and Internal Fixation (ORIF)
ORIF with miniplates is now the gold standard for the majority of displaced mandibular fractures.
Surgical approaches:
- Symphysis/parasymphysis/body: intraoral (gingivobuccal) incision; blunt dissection exposes lower border of mandible
- Angle fractures: intraoral or transbuccal approach
- Subcondylar fractures: retromandibular incision (most direct access to ramus and subcondylar region; risk of facial nerve)
- High condylar neck fractures: pre-auricular incision +/- retromandibular
- Endoscope-assisted repair: technically difficult, avoids large facial scars
Plate configuration:
- Simple fractures: monocortical 2 mm miniplates, 6 mm screws
- Anterior mandible: two plates (superior tension band + inferior)
- Posterior mandible: one plate usually sufficient
- Comminuted/infected/avulsive fractures: load-bearing osteosynthesis with rigid internal fixation and bicortical screws
Condylar Fractures (Special Consideration)
Condylar fractures remain the most controversial area in mandibular trauma management. Unlike other mandibular fractures, closed management (IMF) may be acceptable in:
- Intracapsular fractures
- Unilateral undisplaced condylar fractures
- Children (condylar remodeling capacity is greater)
ORIF is preferred for:
- Bilateral displaced condylar neck fractures
- High intracapsular fractures
- Significant loss of mandibular height/ramus shortening
- Dislocation of condyle into middle cranial fossa or external auditory canal
Functional adaptation, neuromuscular rehabilitation, and altered condylar mechanics may compensate for the deficiencies of IMF. This is the only subsite where these factors may justify non-operative management. (Scott-Brown's)
Complications
| Complication | Details |
|---|---|
| Malocclusion | Most common complication; requires replating if due to malposition |
| Non-union / fibrous union | Occurs when motion persists across fracture; bridged by fibrous tissue (pseudoarthrosis) |
| Infection / osteomyelitis | More common in compound fractures; treat with antibiotics ± removal of infected hardware |
| Nerve injury (inferior alveolar / mental) | Paraesthesia of lower lip/chin; may be temporary or permanent |
| TMJ ankylosis | Complication of condylar fractures, especially in children |
| Osteonecrosis | Particularly in atrophic edentulous mandibles |
| Trismus | Restricted mouth opening; may be due to haematoma, fibrosis, or plate irritation |
| Malunion | Healing in incorrect position |
Key Points Summary
Maxillary Fractures:
- May involve the orbits (Le Fort II/III)
- Always disrupt the dental occlusion
- Internal fixation has replaced external fixation for most fractures
- Most high-energy fractures are not pure Le Fort injuries and are also comminuted
- Haemorrhage arrested with anterior/posterior nasal packs or epistats
- Check visual acuity in all patients with middle-third injuries (retrobulbar haemorrhage)
Mandibular Fractures:
- Often multiple - always look for a second fracture
- IMF following closed reduction is no longer acceptable for the majority of mandibular injuries
- Most displaced fractures managed with ORIF using miniplates
- Condylar fractures remain the exception where non-operative management may be appropriate
- Mental nerve paraesthesia must be documented pre-operatively
Sources: Cummings Otolaryngology Head and Neck Surgery (9780323612173); Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1 (9781138094611); K.J. Lee's Essential Otolaryngology (9781260122237)
This is a shared conversation. Sign in to Orris to start your own chat.