Management of hepato-renal syndrome as per latest peer reviewed guidelines
Reading File
Finding Sources
Searching PubMed
"hepatorenal syndrome" AND management
Searching the Web
hepatorenal syndrome management guidelines 2024 2025 EASL AASLD
Reading File
Reading File
Reading Article
PMID: 37978969
Reading Article
PMID: 41853888
Reading File
Reading File
Reading Article
PMID: 41114681
Loading Image
Reading File
I now have more than enough information to provide a thorough, well-sourced answer. Let me compile everything.
Hepatorenal Syndrome (HRS): Management per Latest Guidelines
Overview and Updated Nomenclature
The terminology for HRS was updated by the International Club of Ascites (ICA) and is now reflected in AASLD (2021) and AGA (2024) guidance:
- HRS-AKI (formerly Type 1 HRS): rapid, progressive renal impairment - defined by a rise in serum creatinine (SCr) ≥0.3 mg/dL within 48 h OR ≥50% rise from baseline within 7 days, in the absence of other AKI causes. Median survival without treatment is ~2 weeks.
- HRS-CKD (formerly Type 2 HRS): moderate, stable renal impairment (SCr 1.25-2.5 mg/dL), typically presenting with refractory ascites. Median survival 4-6 months.
HRS occurs in ~10-30% of hospitalized cirrhotics with AKI, with annual incidence of ~8% in cirrhotic patients with ascites.
Pathophysiology (Basis of Treatment)
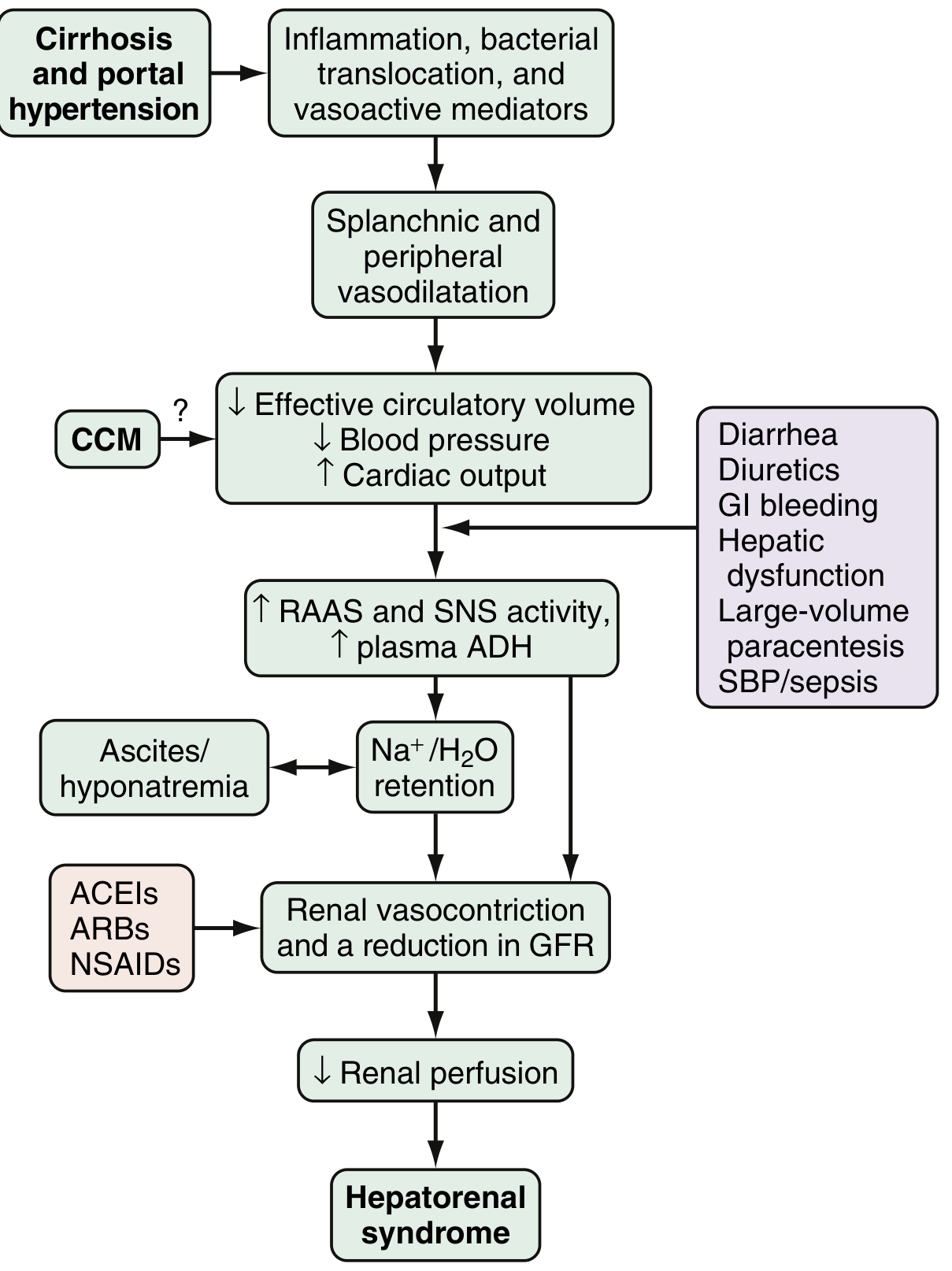
Fig. 94.2 - Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Three core mechanisms drive HRS:
- Splanchnic/systemic vasodilation (mediated by NO, CO, glucagon, prostacyclin) reduces effective circulatory volume
- Compensatory renal vasoconstriction via RAAS, SNS activation, and ADH release
- Cirrhotic cardiomyopathy (CCM) further impairs cardiac output and renal perfusion
Precipitants include: SBP/sepsis (30% risk), severe alcoholic hepatitis (25%), serial large-volume paracentesis without albumin (10%), GI bleeding, diuretics.
Diagnostic Criteria (ICA/AASLD)
Before labeling HRS, exclude other AKI causes:
- Stop all diuretics and nephrotoxins (ACEIs, ARBs, NSAIDs)
- Give albumin 1 g/kg/day IV for 48 hours (max 100 g/day) - if no improvement, HRS is confirmed
- No improvement with fluid challenge
- No intrinsic renal disease (absence of proteinuria >500 mg/day, hematuria >50 RBCs/HPF, abnormal renal ultrasound)
- Exclude hypovolemic shock, septic shock, nephrotoxic drugs
AKI staging (ICA criteria):
- Stage 1: SCr rise ≥0.3 mg/dL or 1.5-2× baseline
- Stage 2: SCr rise >2-3× baseline
- Stage 3: SCr >3× baseline or ≥4.0 mg/dL with acute rise ≥0.3 mg/dL, or initiation of RRT
Prevention (High Priority)
- Avoid intravascular volume depletion: careful diuretic titration, lactulose avoidance in excess, albumin with large-volume paracentesis (6-8 g/L removed per AGA 2025)
- Avoid nephrotoxins: NSAIDs, ACEIs, ARBs, aminoglycosides
- SBP: IV albumin 1.5 g/kg at diagnosis + 1 g/kg on day 3 reduces HRS risk by ~70%
- Norfloxacin 400 mg/day for primary SBP prophylaxis in high-risk patients (Child-Pugh C, low ascitic protein <1.5 g/dL with renal/liver dysfunction)
- Treat infections promptly (SBP, bacteremia)
Treatment of HRS-AKI
Step 1: Immediate Supportive Measures
- Discontinue ALL nephrotoxins (diuretics, NSAIDs, ACEIs, ARBs)
- Treat underlying precipitants (antibiotics for infection)
- IV albumin bolus: 1 g/kg/day for 48 hours (max 100 g/day); continue at 20-60 g/day to maintain CVP 10-15 cmH₂O
Step 2: Vasopressor Therapy (Combined with Albumin)
The goal is splanchnic vasoconstriction to improve effective circulating volume and renal perfusion. Duration: generally up to 2 weeks.
First-Line: Terlipressin + Albumin (AASLD, EASL, AGA 2024 - all concordant)
Terlipressin received FDA approval (as TERLIVAZ) in 2022 for HRS-AKI. It is now the vasoactive drug of choice per AGA Clinical Practice Update 2024 (Garcia-Tsao et al., PMID 37978969):
| Regimen | Details |
|---|---|
| Bolus dosing | 1 mg IV every 4-6 hours; increase to 2 mg IV every 4-6 hours if SCr does not fall ≥25% by day 3 |
| Continuous infusion | 2 mg/day IV; may increase to 12 mg/day - preferred per recent meta-analysis (PMID 41853888) |
| Duration | Until HRS reversal (full response = SCr return to within 0.3 mg/dL of baseline) or max 14 days |
| Monitoring | Can be administered via peripheral IV line; does NOT require ICU monitoring per AGA 2024 |
Continuous vs. bolus terlipressin: A 2026 meta-analysis of 6 RCTs (PMID 41853888) found continuous infusion had fewer adverse events (RR 0.59), less cardiovascular side effects, and comparable HRS reversal rates. Optimal dose: 4-5 mg/day.
Contraindications/cautions: Ischemic cardiovascular disease, respiratory failure (risk of pulmonary edema), ACLF Grade 3 (very poor outcomes).
Second-Line: Norepinephrine + Albumin (ICU only)
- Dose: 0.1-0.7 mcg/kg/min IV infusion, titrated to increase MAP ≥10 mmHg
- Requires ICU monitoring; comparable efficacy to terlipressin in some studies but less convenient
Third-Line: Midodrine + Octreotide + Albumin
Now explicitly downgraded to third-line by AGA 2024 (Best Practice Advice #9-10):
- Midodrine (oral α-agonist): 5-15 mg orally three times daily
- Octreotide (somatostatin analogue): 100-200 mcg SC/IV three times daily OR 25 mcg/hr IV infusion
- Inferior to terlipressin; may be used in outpatient settings or where terlipressin is unavailable
Step 3: Renal Replacement Therapy (RRT)
- Initiated when vasopressor therapy fails to reverse HRS-AKI
- Used as a bridge to liver transplantation (LT), not a standalone treatment
- Does not improve survival in the absence of LT
Step 4: Transjugular Intrahepatic Portosystemic Shunt (TIPS)
- Not first-line for HRS-AKI (given rapid course)
- Most useful for HRS-CKD and refractory ascites
- Reduces portal pressure, improves renal blood flow
- Contraindicated in: Child-Pugh >13, hepatic encephalopathy, bilirubin >5 mg/dL, HCC
- Meta-analysis (PMID 37141993) confirms TIPS prevents further decompensation and improves survival in portal hypertension
Step 5: Liver Transplantation (Definitive Treatment)
- The only definitive therapy for HRS - renal function typically recovers after LT as the kidney itself is histologically normal
- HRS reversal with vasopressors before LT improves post-transplant outcomes and reduces need for peritransplant RRT
- All HRS patients should be evaluated for LT urgently (all HRS-AKI patients warrant MELD exception points)
- Combined liver-kidney transplantation (CLKT) considered if: HRS-AKI on RRT >4 weeks, or HRS-CKD with GFR <25 mL/min for >3 months
Management Summary Table
| Intervention | Indication | Dosing | Evidence Level |
|---|---|---|---|
| Stop nephrotoxins/diuretics | All HRS | Immediate | Strong |
| IV albumin (loading) | All HRS-AKI | 1 g/kg/day × 48h (max 100g/day) | Strong |
| Terlipressin + albumin | HRS-AKI first-line | 1-2 mg IV q4-6h (bolus) or 2-12 mg/day (infusion) | Strong (FDA approved) |
| Norepinephrine + albumin | HRS-AKI, ICU patients | 0.1-0.7 mcg/kg/min, titrate MAP +10 mmHg | Moderate |
| Midodrine + octreotide + albumin | HRS-AKI, third-line | Midodrine 5-15 mg TID; octreotide 100-200 mcg TID | Moderate (downgraded 2024) |
| TIPS | HRS-CKD, refractory ascites | Per hepatology assessment | Moderate |
| Liver transplantation | All HRS | Urgent evaluation | Strong (definitive) |
| Albumin with SBP | Prevention | 1.5 g/kg day 1, 1 g/kg day 3 | Strong |
| Albumin with LVP | Prevention | 6-8 g/L removed | Strong |
Special Considerations
ACLF (Acute-on-Chronic Liver Failure): Terlipressin efficacy is reduced in ACLF Grade 3 (multi-organ failure). These patients have very high short-term mortality and decisions about escalation vs. goals-of-care discussions are important.
Frailty: Higher frailty scores are independently associated with worse outcomes in HRS hospitalizations; frailty assessment should inform clinical decision-making.
Response assessment:
- Full response: SCr returns to within 0.3 mg/dL of baseline
- Partial response: ≥1 AKI stage reduction but not back to baseline
- No response: no AKI stage regression - consider second-line therapy, RRT, or palliative planning
Key Guideline Sources
- AGA Clinical Practice Update 2024: Vasoactive Drugs & Albumin in Cirrhosis (Garcia-Tsao et al., Gastroenterology 2024) - PMID 37978969
- AGA Clinical Practice Update 2025: Ascites, Volume Overload & Hyponatremia (Orman et al., Gastroenterology 2025) - PMID 41114681
- AASLD Practice Guidance 2021: Diagnosis, Evaluation & Management of Ascites/SBP/HRS (Hepatology 74:1014-1048)
- EASL Clinical Practice Guidelines on Decompensated Cirrhosis (J Hepatol 2018; updated 2023)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Chapter 94
- Harrison's Principles of Internal Medicine 22E (2025)
What is Low protein in Ascites
Finding Sources
Finding Sources
Searching the Web
low protein ascites SBP prophylaxis norfloxacin guidelines cirrhosis
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a comprehensive answer.
Low Protein in Ascites
Definition
Low protein ascites is defined as an ascitic fluid total protein concentration of <1.5 g/dL (some sources use <1.0 g/dL as the threshold for highest infection risk). It is characteristic of cirrhotic ascites and carries important diagnostic and clinical implications.
Why is Protein Low in Cirrhotic Ascites?
The mechanism is structural. In cirrhosis, fibrous tissue is deposited in the hepatic sinusoids - a process called "capillarization of the sinusoid." Normal hepatic sinusoids are uniquely "leaky" to large molecules. After capillarization, the sinusoids become less permeable to macromolecules (including albumin), so the liver lymph - and hence the ascitic fluid formed from it - has an abnormally low protein content.
In contrast, in post-hepatic causes (heart failure, Budd-Chiari syndrome), the sinusoids remain normal and still leak protein-rich lymph - so those ascites have a high protein content, despite also having a high SAAG.
"In cirrhosis, there is deposition of fibrous tissue in the sinusoids (capillarization of the sinusoid), which renders the sinusoids less leaky to macromolecules and this leads to an abnormally low protein content of liver lymph."
- Yamada's Textbook of Gastroenterology, 7th ed.
Diagnostic Significance: SAAG + Ascitic Protein Together
The SAAG (Serum-Ascites Albumin Gradient) alone cannot distinguish cirrhosis from cardiac or Budd-Chiari ascites - all three give SAAG ≥1.1 g/dL. Ascitic protein is the discriminating test:
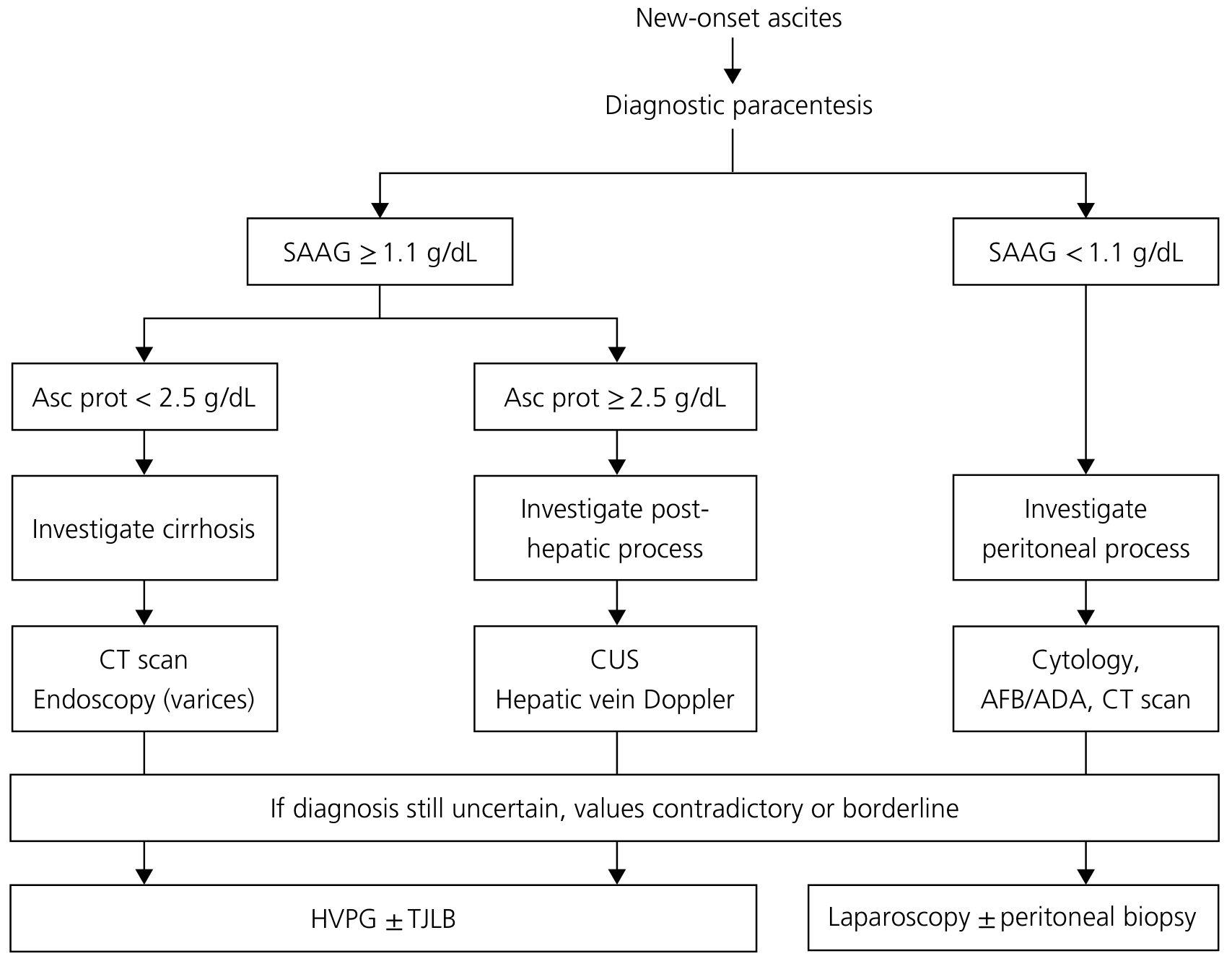
Fig. 98.1 - Yamada's Textbook of Gastroenterology, 7th ed.
| Cause | SAAG | Ascitic Protein |
|---|---|---|
| Cirrhosis | ≥1.1 g/dL (HIGH) | <2.5 g/dL (LOW) |
| Cardiac ascites / Budd-Chiari / Constrictive pericarditis | ≥1.1 g/dL (HIGH) | ≥2.5 g/dL (HIGH) |
| Peritoneal malignancy / TB / Peritonitis | <1.1 g/dL (LOW) | >2.5 g/dL (HIGH) |
| Nephrotic syndrome / Protein-calorie malnutrition | <1.1 g/dL (LOW) | LOW |
This distinction is clinically important - constrictive pericarditis is one of the few curable causes of ascites, and missing it (by only checking SAAG) is a major error. In alcoholic patients especially, ascites can be from alcoholic cardiomyopathy OR cirrhosis, with very different management implications.
Clinical Importance: SBP Risk
Ascitic fluid protein is directly related to its opsonic activity - the ability to fight bacterial infection. Cirrhotic patients with ascitic protein <1.0-1.5 g/dL have markedly poor defenses against bacterial infection and are at high risk of spontaneous bacterial peritonitis (SBP).
- Protein <1.0 g/dL: highest risk of SBP
- Protein <1.5 g/dL: threshold used for primary SBP prophylaxis
Ascitic protein also helps differentiate SBP from secondary (surgical) peritonitis - protein >1.0 g/dL in an infected tap raises suspicion for secondary peritonitis.
Clinical Application: Primary SBP Prophylaxis Criteria
Patients with low-protein ascites AND any of the following criteria qualify for long-term primary prophylaxis with norfloxacin 400 mg/day:
| Criterion | Threshold |
|---|---|
| Ascitic fluid protein | <1.5 g/dL |
| PLUS Child-Pugh score | ≥9 with bilirubin ≥3 mg/dL |
| OR serum creatinine | ≥1.2 mg/dL |
| OR serum sodium | <130 mEq/L |
Outcome data: A landmark RCT showed that norfloxacin in this population reduced:
- 1-year SBP probability: 61% → 7%
- HRS development: 41% → 28%
- 3-month mortality: 38% → 6%
(Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Chapter 93)
Alternative agents (where norfloxacin is unavailable): trimethoprim-sulfamethoxazole (1 DS tablet daily), rifaximin (proposed but evidence less established).
Other Non-Cirrhotic Causes of Low Protein Ascites
Beyond cirrhosis, protein-poor ascites can occur from decreased capillary oncotic pressure:
- Nephrotic syndrome - massive proteinuria depletes serum albumin; ascites responds to salt restriction + diuretics
- Protein-calorie malnutrition / Kwashiorkor - severe hypoalbuminemia
- Protein-losing enteropathy - GI protein loss
In all these, SAAG will be <1.1 g/dL (no portal hypertension) and protein will be low (because serum albumin is low globally, limiting protein gradient into the ascites).
Summary
| Feature | Details |
|---|---|
| Definition | Ascitic fluid total protein <1.5 g/dL (risk threshold) or <1.0 g/dL (highest risk) |
| Main cause | Cirrhosis (sinusoidal capillarization reduces protein permeability) |
| Diagnostic role | Differentiates cirrhotic from cardiac/Budd-Chiari ascites (both high SAAG) |
| Infection risk | Low opsonic activity → high SBP risk |
| Prophylaxis | Norfloxacin 400 mg/day if protein <1.5 g/dL + advanced liver/kidney dysfunction |
| Non-cirrhotic causes | Nephrotic syndrome, kwashiorkor, protein-losing enteropathy |
- Yamada's Textbook of Gastroenterology, 7th ed., Chapter 98
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Chapter 93
Serum albumin- 2.7, ascitic albumin- 1.0and ascitic protein is 2.0. Define it
This is a straightforward calculation I can answer directly.
Given values:
- Serum albumin = 2.7 g/dL
- Ascitic albumin = 1.0 g/dL
- Ascitic total protein = 2.0 g/dL
Step 1: Calculate SAAG
SAAG = Serum albumin − Ascitic albumin
SAAG = 2.7 − 1.0 = 1.7 g/dL
Step 2: Interpret SAAG
SAAG ≥ 1.1 g/dL → Portal hypertension is present
(Accuracy ~97% for sinusoidal hypertension as the cause of ascites)
Step 3: Interpret Ascitic Total Protein
Ascitic protein = 2.0 g/dL
- This is <2.5 g/dL → points toward intrahepatic (cirrhotic) cause
- This is ≥1.5 g/dL → does NOT meet the threshold for primary SBP prophylaxis (which requires protein <1.5 g/dL)
- This is >1.0 g/dL → slightly above the highest-risk SBP threshold, but still relatively low opsonic activity
Step 4: Final Interpretation
| Parameter | Value | Interpretation |
|---|---|---|
| SAAG | 1.7 g/dL (≥1.1) | Portal hypertension present |
| Ascitic protein | 2.0 g/dL (<2.5) | Low-protein ascites |
| Combined pattern | High SAAG + Low protein | Cirrhotic ascites |
Conclusion
This fluid profile is consistent with cirrhotic ascites:
- High SAAG (1.7) confirms portal hypertension as the driving mechanism
- Low ascitic protein (2.0 g/dL) confirms intrahepatic (sinusoidal) origin - the capillarized cirrhotic sinusoids leak poorly, producing protein-poor fluid
- This pattern distinguishes it from cardiac/Budd-Chiari ascites (which would show high SAAG + high protein ≥2.5 g/dL) and from peritoneal malignancy/TB (which would show low SAAG + high protein)
Regarding SBP prophylaxis: At protein 2.0 g/dL, the patient does NOT meet the <1.5 g/dL threshold for primary norfloxacin prophylaxis based on protein alone - but clinical risk factors (Child-Pugh score, bilirubin, creatinine, sodium) should still be assessed independently to determine prophylaxis eligibility.
Note: If serum globulins are >5 g/dL, apply the SAAG correction factor: uncorrected SAAG × (0.16 × [serum globulin + 2.5]) to avoid a falsely elevated gradient.
Why lasilactone not given in HRS with DCLD
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have all the information needed. Here is the complete, well-reasoned answer.
Why Lasilactone is NOT Given in HRS with DCLD
Lasilactone = Furosemide (loop diuretic) + Spironolactone (aldosterone antagonist)
While Lasilactone is the standard treatment for cirrhotic ascites, it is contraindicated in HRS for multiple, compounding reasons - each one making kidney injury worse.
Understanding the Context First
In DCLD (Decompensated Chronic Liver Disease) with HRS, the kidneys are already in a state of intense renal vasoconstriction and critically reduced renal perfusion. The effective circulating volume is already severely depleted due to splanchnic vasodilation. Any further reduction in circulatory volume is catastrophic.
Reasons Lasilactone is Stopped in HRS
1. Furosemide - Worsens Prerenal State and Renal Hypoperfusion
| Mechanism | Why it Harms |
|---|---|
| Blocks Na-K-2Cl transporter in thick ascending limb | Natriuresis and diuresis → further reduction in already-depleted intravascular volume |
| Activates RAAS and SNS | Compensatory response worsens renal vasoconstriction |
| Inhibits Na-K-Cl transporter | Triggers release of arginine vasopressin → hyponatremia |
| May cause hypokalemia | Electrolyte imbalance worsens hepatic encephalopathy |
In HRS, the kidney is not failing due to excess fluid - it is failing due to functional vasoconstriction with no intrinsic pathology. Forcing more diuresis is like stepping on the accelerator when the fuel line is already blocked.
2. Spironolactone - Causes Life-Threatening Hyperkalemia
| Mechanism | Why it Harms |
|---|---|
| Blocks aldosterone receptors in collecting duct | Prevents K⁺ excretion in the distal nephron |
| In HRS, GFR is already severely reduced | Very little urine is formed → K⁺ builds up in blood |
| Oliguria/anuria in advanced HRS | No urinary K⁺ loss possible at all |
| Result: Severe hyperkalemia (K⁺ >5.5-6.0 mEq/L) | Risk of fatal cardiac arrhythmia |
The guideline threshold is clear:
"Anti-mineralocorticoids should be stopped in cases of hyperkalemia (>5.5 mEq/L)" "Diuretic treatment should be withheld in cases of... AKI"
- Sleisenger & Fordtran's GI & Liver Disease, Chapter 93
3. Both Together - Accelerate AKI Progression
Combined furosemide + spironolactone in HRS:
- Reduces intravascular volume further → worsens renal hypoperfusion
- Reduces GFR further → converts HRS-AKI Stage 1 to Stage 3
- Removes the possibility of HRS reversal with vasopressors (because volume depletion masks response assessment)
- Prevents accurate diagnosis - the 48-hour albumin challenge (1 g/kg IV) used to diagnose HRS requires diuretics to be stopped first, to exclude volume-responsive AKI
4. Diagnostic Protocol Requires Diuretic Withdrawal
The ICA/AASLD diagnostic criteria for HRS-AKI mandates:
- Stop all diuretics
- Give IV albumin 1 g/kg/day × 48 hours
- If creatinine does not improve → confirm HRS
If Lasilactone is continued, you cannot properly diagnose HRS OR assess response to terlipressin therapy.
What to Do Instead
| Stopped | Replaced With |
|---|---|
| Furosemide + Spironolactone (Lasilactone) | IV Albumin 1 g/kg/day (volume expansion) |
| — | Terlipressin 1-2 mg IV q4-6h (splanchnic vasoconstrictor - first line) |
| — | Norepinephrine 0.1-0.7 mcg/kg/min (ICU, second line) |
| — | Treat precipitant (antibiotics for SBP/infection) |
| — | Evaluate urgently for liver transplantation |
Simple Summary
Lasilactone reduces volume → HRS is already a low-volume state. Spironolactone blocks K⁺ excretion → HRS kidneys cannot excrete K⁺ → fatal hyperkalemia. Together, they worsen the very mechanism causing HRS and prevent its treatment.
The goal in HRS is the opposite of diuresis - it is to restore effective circulating volume (albumin) and reduce renal vasoconstriction (terlipressin), not to remove more fluid.
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Chapters 93 & 94
- Harrison's Principles of Internal Medicine 22E (2025)
- AGA Clinical Practice Update 2024, PMID 37978969
This is a shared conversation. Sign in to Orris to start your own chat.