Ocular sonography in emergency room
Reading File
Finding Sources
Finding Sources
Searching PubMed
ocular ultrasound emergency department point-of-care
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive content from three major emergency medicine textbooks plus real sonographic images. Let me compose the full answer.
Ocular Sonography in the Emergency Room
Bedside ocular ultrasound (point-of-care ultrasound, POCUS) has become a standard skill for emergency physicians since the first published series by Blaivas et al. in 2000. It is fast, non-invasive, radiation-free, and can be performed at the bedside without moving a trauma patient or waiting for radiology.
Indications
Ocular POCUS is appropriate in any patient presenting with:
- Altered vision or sudden vision loss
- Ocular or periorbital pain
- Eye trauma (blunt or penetrating)
- Suspected intraocular foreign body (FB)
- Head injury or altered mental status
- Headache (to assess raised intracranial pressure)
- Periorbital edema or hematoma obscuring fundoscopy
Conditions reliably diagnosed include: globe rupture, intraocular FB, vitreous hemorrhage, retinal detachment, lens dislocation, and elevated intracranial pressure (via optic nerve sheath diameter).
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 1484
Equipment
A linear array transducer (7.5-10 MHz or higher) is preferred. The high frequency provides superior resolution of the superficial globe structures. A curvilinear probe can be used but gives inferior detail. The machine should be set to the ocular/ophthalmic preset (which limits thermal index and mechanical index to safer values - recommended exposure limits are half those of fetal imaging).
Technique: The No-Pressure Method
This is the single most important safety point - excessive pressure on a potentially ruptured globe can cause vitreous extrusion.
- Patient recumbent or semi-reclined to prevent gel runoff
- Instruct patient: eyes closed, relaxed, gazing straight ahead
- Place a large piece of clear Tegaderm over the closed eyelid as a barrier
- Apply a copious amount of gel over the dressing - enough to fill the orbital sulcus so the probe floats in gel without touching the eyelid
- Rest the scanning hand on the patient's forehead, bridge of nose, or maxilla for stabilization
- Touch probe to gel without applying any pressure (no-pressure technique)
- Scan in transverse then longitudinal planes; adjust gain and depth
- Identify: anterior chamber, iris, lens, vitreous, retina, optic nerve sheath
- Roberts and Hedges', p. 1485
- Rosen's Emergency Medicine, 9e
Sonographic Findings by Diagnosis
1. Retinal Detachment
Sensitivity 97-100%, specificity 83-92% when performed by emergency physicians.
Appears as a hyperechoic, undulating membrane in the posterior-to-lateral globe, protruding into the vitreous. It remains tethered at the ora serrata anteriorly and the optic disc posteriorly. Critically, unlike choroidal detachment, retinal detachment moves with eye movements - dynamic scanning (asking the patient to look side to side) helps confirm this.

The panel below shows (A) normal eye with lens visible, (B) retinal detachment (large arrow = lens, small arrow = detachment), and (C) ruptured globe:
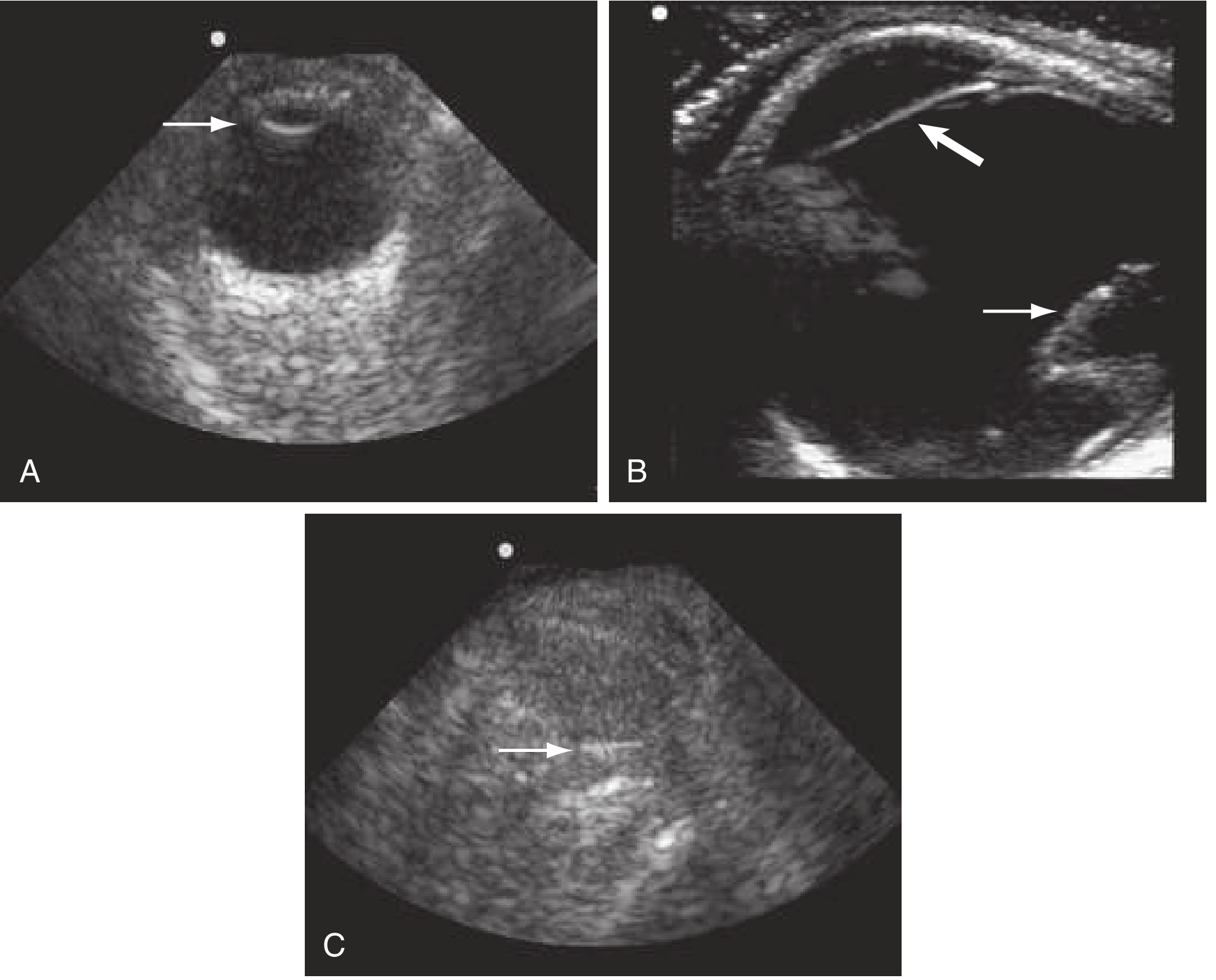
- Tintinalli's Emergency Medicine, p. 1600
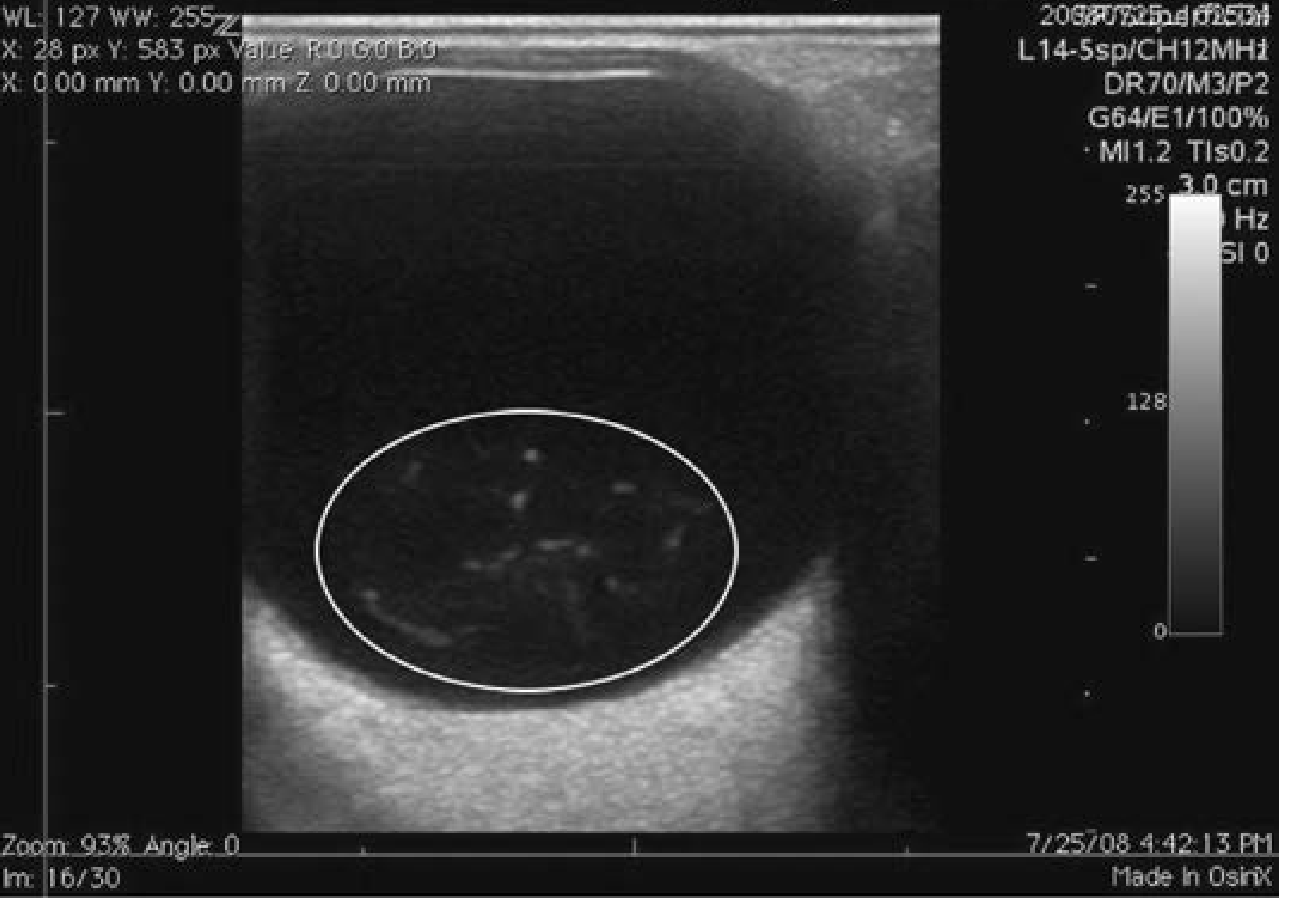
2. Vitreous Hemorrhage
Appears as echogenic material in the posterior chamber. Appearance depends on age and severity:
- Acute/mild: small dots or low-amplitude mobile opacities (increase gain to detect)
- Organized: thick mobile membranes, multiple large echoes filling the vitreous
- Due to gravity, opacities may layer inferiorly
3. Globe Rupture
Look for:
- Loss of normal spherical globe shape / globe deformity
- "Flat tire" sign (flattening of the anterior globe contour)
- Vitreous collapse
- Intraocular air
If globe rupture is suspected clinically, perform the no-pressure technique with extreme caution. If the exam obviously confirms open globe, stop - the risk of vitreous extrusion outweighs further imaging benefit. CT of orbits is the gold standard in that scenario.
4. Intraocular Foreign Body
Metallic FBs are especially visible - bright echogenic focus with posterior shadowing or reverberation (comet-tail) artifact in the echolucent vitreous. Wood is more difficult to detect. A track of hemorrhage may mark the path of FB penetration. Dynamic scanning helps localize size and position.
5. Lens Dislocation
The lens appears as a biconvex echogenic structure in the anterior globe. Dislocation is confirmed when it is found displaced posteriorly or floating in the vitreous. High-resolution US has 94% correlation with CT in detecting lens dislocation and other traumatic ocular injuries.
- Rosen's Emergency Medicine, p. 415
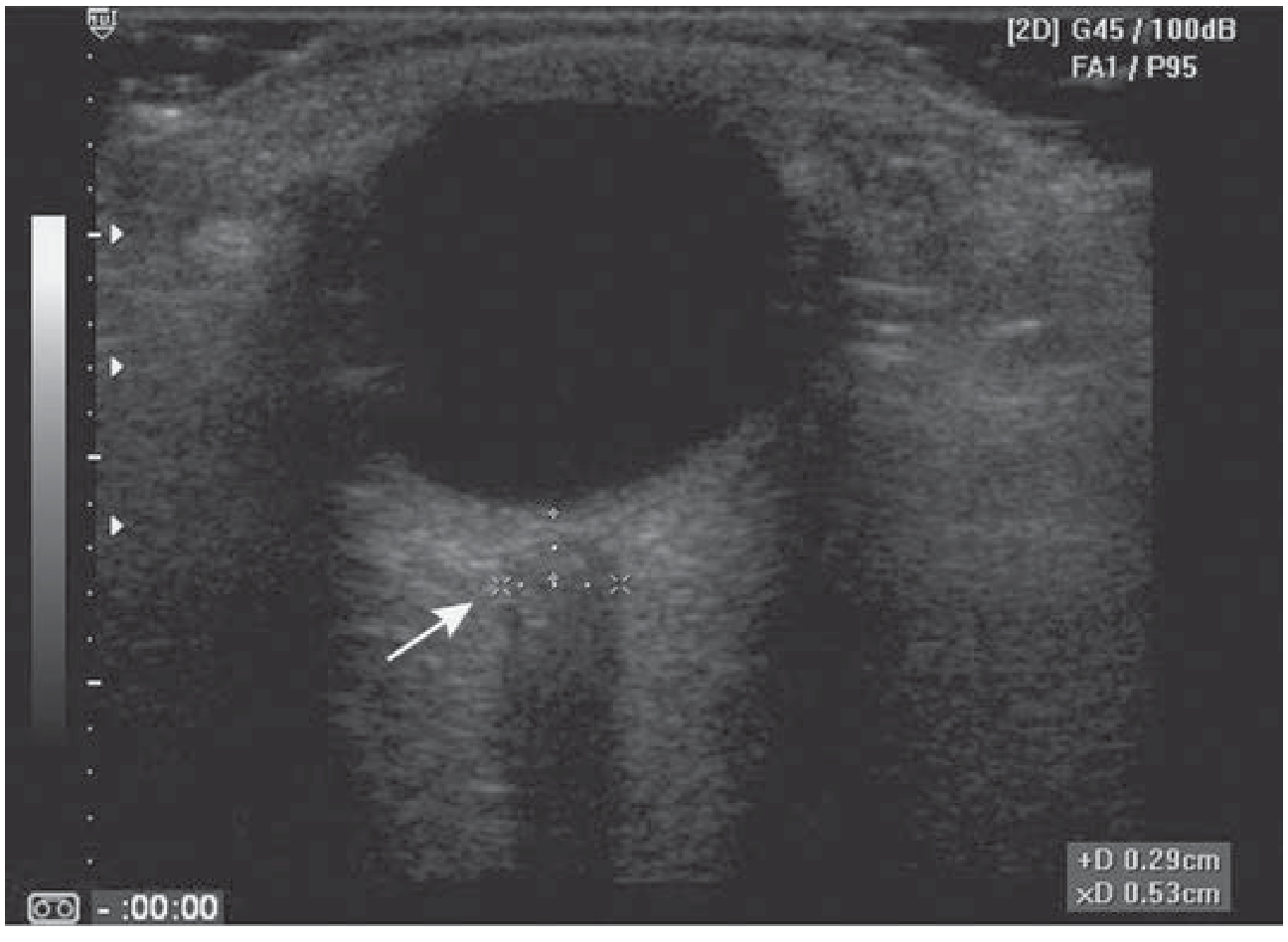
6. Optic Nerve Sheath Diameter (ONSD) - Elevated ICP Screening
This is one of the most powerful non-trauma applications of ocular POCUS. The optic nerve sheath communicates with the subarachnoid space and expands when CSF pressure rises.
Technique:
- Ask the patient to deviate the examined eye ~10 degrees laterally (aligns the nerve with the beam)
- Measure the sheath width 3 mm posterior to the retina (best contrast and reproducibility at this point)
- Average at least 2-3 measurements per eye
Normal values:
| Population | Upper limit of normal ONSD |
|---|---|
| Adults | 5.0 mm |
| Children | 4.5 mm |
| Infants | 4.0 mm |
Diagnostic thresholds: A cutoff of 5.7-6.0 mm for ICP > 20 mmHg gives sensitivity 87-95% and specificity 79-100%. A diameter > 5 mm is considered widened and suspicious for raised ICP.
The differential for an enlarged ONSD includes: elevated ICP, anterior orbital mass, optic neuritis, trauma, and cavernous sinus mass.
- Tintinalli's Emergency Medicine, p. 1601
- Rosen's Emergency Medicine - ONSD > 5 mm guideline to delay LP in suspected meningitis
Contraindications and Cautions
There are no absolute contraindications, but important cautions include:
| Situation | Caution |
|---|---|
| Suspected open globe | Use no-pressure technique; if exam confirms rupture, stop scanning |
| Orbital emphysema | Air artifact will obscure globe contents |
| Air bubbles in vitreous | May mimic intraocular FB |
| Examination duration | Limit time, especially with spectral/color Doppler (thermal risk) |
Relative contraindication: If physical exam obviously confirms open globe, do not scan - risk of vitreous extrusion even with minimal compression.
Summary Table of Sonographic Findings
| Condition | Sonographic Appearance | Key Feature |
|---|---|---|
| Retinal detachment | Hyperechoic undulating membrane, posterior globe | Moves with eye movements |
| Choroidal detachment | Hyperechoic membrane, more peripheral | Does NOT move with eye movements |
| Vitreous hemorrhage | Echogenic dots/membranes in vitreous | Mobile, gravity-dependent layering |
| Globe rupture | Deformed globe, "flat tire" sign | No pressure exam; consider CT |
| Intraocular FB | Bright echogenic focus + shadowing/comet tail | Metallic best seen; wood difficult |
| Lens dislocation | Biconvex structure displaced into vitreous | Displaced from normal anterior position |
| Elevated ICP (ONSD) | Optic sheath width > 5 mm at 3 mm depth | >5.7-6 mm = ICP likely > 20 mmHg |
Key Clinical Pearls
- Always use the no-pressure (flotation) technique - never apply direct probe pressure to the globe
- Scan in at least two planes (transverse and longitudinal) and through the full arc of the globe
- Increase gain to detect early/acute vitreous hemorrhage (can be nearly anechoic initially)
- Dynamic scanning (asking patient to move their eye) differentiates retinal from choroidal detachment
- ONSD measurement is a bedside surrogate for ICP - use it to triage patients with head injury, altered mental status, or suspected meningitis before LP
- Orbital emphysema and air bubbles are sources of false-positive FB findings
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine | Tintinalli's Emergency Medicine: A Comprehensive Study | Rosen's Emergency Medicine: Concepts and Clinical Practice
Recent literature: A 2024 review in Emerg Med Clin North Am (Pierre et al., PMID 39326993) provides an up-to-date overview of ocular US in the ED. A 2025 review in Adv Emerg Nurs J (Gonzalez et al., PMID 39641540) specifically addresses point-of-care US for ocular emergencies from a nursing/advanced practice perspective.
This is a shared conversation. Sign in to Orris to start your own chat.