Give me most common ICU images with explanations high yield
Reading File
Finding Sources
Finding Sources
Searching Images
ICU chest X-ray pneumothorax endotracheal tube central line
Reading File
Searching Images
ARDS bilateral infiltrates chest X-ray ICU diffuse opacities
Searching Images
tension pneumothorax tracheal deviation mediastinal shift X-ray
Searching Images
pulmonary edema cardiogenic Kerley B lines bat wing perihilar haziness chest X-ray
Searching Images
malpositioned endotracheal tube right mainstem bronchus intubation
Searching Images
central venous catheter pleural effusion misplaced line chest X-ray
Searching Images
pleural effusion blunting costophrenic angle chest X-ray ICU
Searching Images
pneumonia lobar consolidation air bronchogram chest X-ray
I now have excellent images and information to compile a comprehensive, high-yield ICU radiology guide. Let me put it all together.
🫁 High-Yield ICU Chest X-Ray Findings
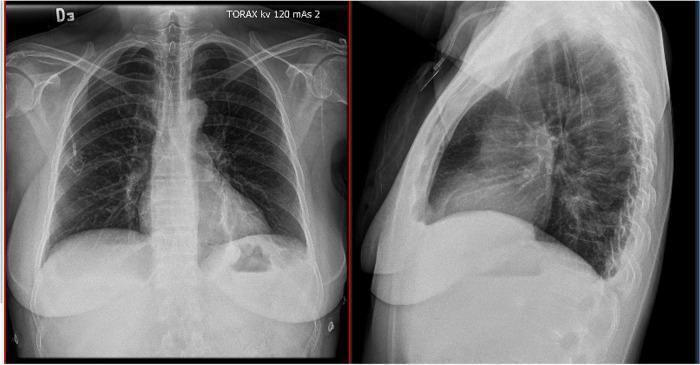
1. Normal ICU Chest X-Ray — Devices in Situ
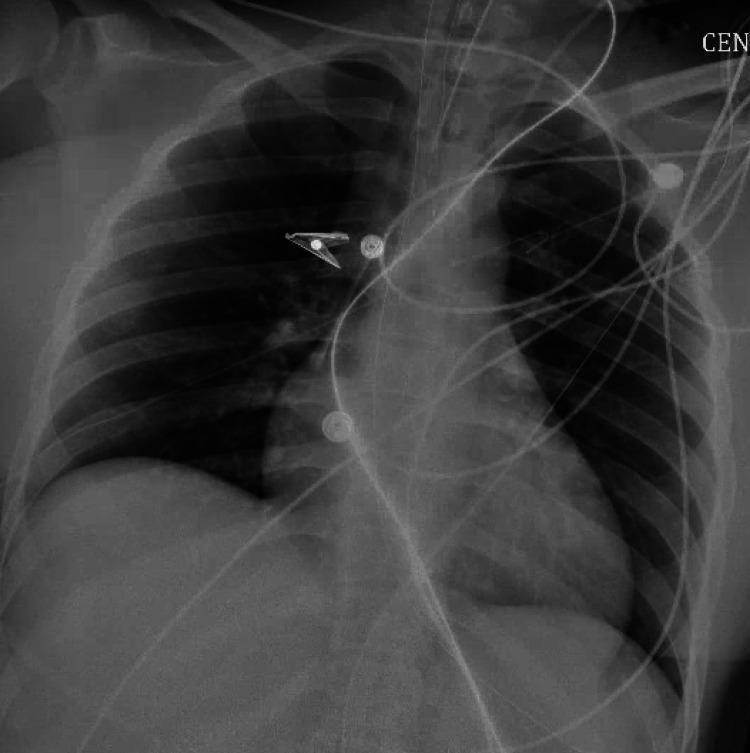
What to look for on every ICU CXR (systematic approach — ABCDE):
- Airway: ETT tip should be 3–5 cm above the carina (ideally at level of the aortic arch); check for tracheal deviation
- Breathing: Lung fields — symmetric aeration, no pneumothorax, no consolidation, no effusion
- Cardiac: Cardiothoracic ratio < 0.5 on PA (< 0.55 acceptable on AP portable)
- Diaphragm: Costophrenic angles sharp; right hemidiaphragm slightly higher than left
- Everything else: NGT, central line, chest tubes, pacemaker leads — confirm positions
Common devices visible:
| Device | Correct Position |
|---|---|
| ETT | 3–5 cm above carina (~T4 level, aortic arch) |
| Central venous catheter | Tip at SVC-RA junction (right tracheobronchial angle) |
| NGT/OGT | Tip below diaphragm, in stomach |
| Chest tube | Apex for pneumothorax; base for effusion |
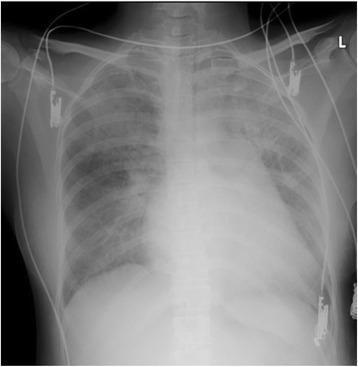
2. Endotracheal Tube Malposition — Right Mainstem Intubation
Classic picture: ETT tip beyond carina → in right mainstem bronchus → left lung white-out (atelectasis) + right lung hyperinflation
Key teaching points:
- Most common because the right mainstem bronchus is shorter and less angulated than the left
- Immediate fix: pull ETT back until tip sits above carina
- Mediastinal shift toward the collapsed (left) side — distinguishes this from tension pneumothorax, where shift is away from the pathology
- On exam: absent breath sounds on the left; ventilator shows increasing peak pressures
Danger: Barotrauma to the right lung; severe hypoxemia from V/Q mismatch
3. Tension Pneumothorax
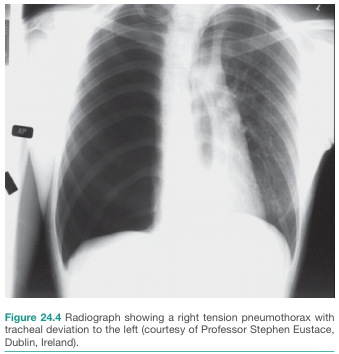
Classic picture:
- Tracheal + mediastinal shift AWAY from the affected side
- Hyperlucent hemithorax with absent lung markings
- Depressed ipsilateral hemidiaphragm
- ± Cardiac silhouette displaced

Key teaching points:
- This is a clinical diagnosis — do NOT wait for CXR if patient is unstable
- Immediate treatment: needle decompression (2nd intercostal space, midclavicular line) → definitive chest tube
- In ventilated patients: sudden ↑ peak airway pressures + hypotension + hypoxia = tension PTX until proven otherwise
- Deep sulcus sign on supine AP CXR (air collects anteriorly, costophrenic angle appears abnormally deep and lucent)
- Post-decompression complication: re-expansion pulmonary edema (bilateral infiltrates developing after rapid lung re-expansion — shown in Panel B above)
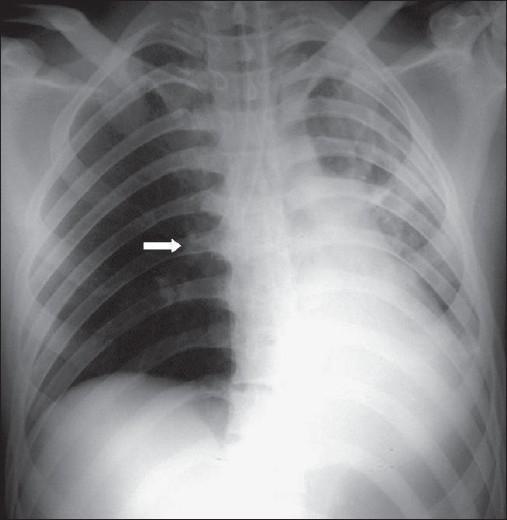
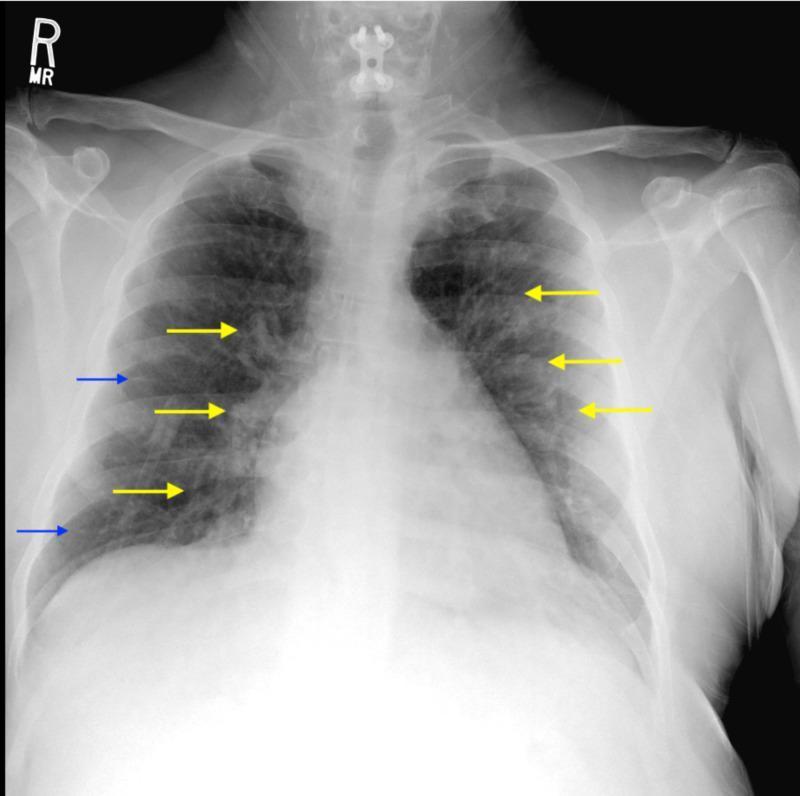
4. Simple Pneumothorax (Barotrauma)

Classic picture:
- Thin visceral pleural line (white line) visible, with absent lung markings peripheral to it
- No mediastinal shift (unlike tension PTX)
Key teaching points:
- Highest risk: mechanically ventilated patients (barotrauma from high tidal volumes/pressures)
- Associations: ARDS, bullous emphysema, post-procedural (central line placement)
- Small PTX in a non-ventilated, stable patient → observation; in ventilated patients → chest tube mandatory (will progress to tension)
- Subcutaneous emphysema (air in soft tissues — streaky lucency in neck/chest wall) is a tip-off to underlying barotrauma
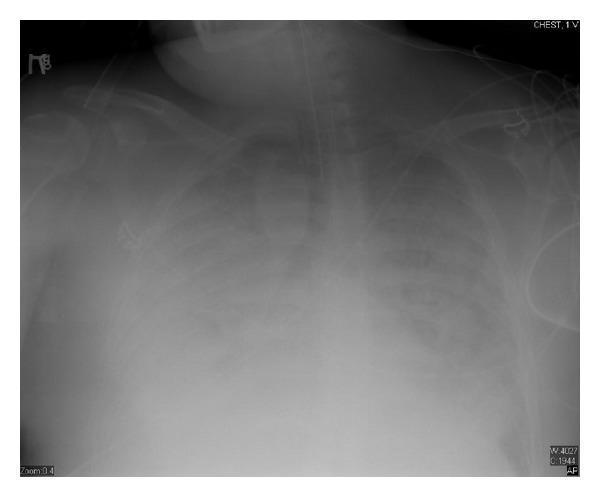
5. ARDS — Acute Respiratory Distress Syndrome
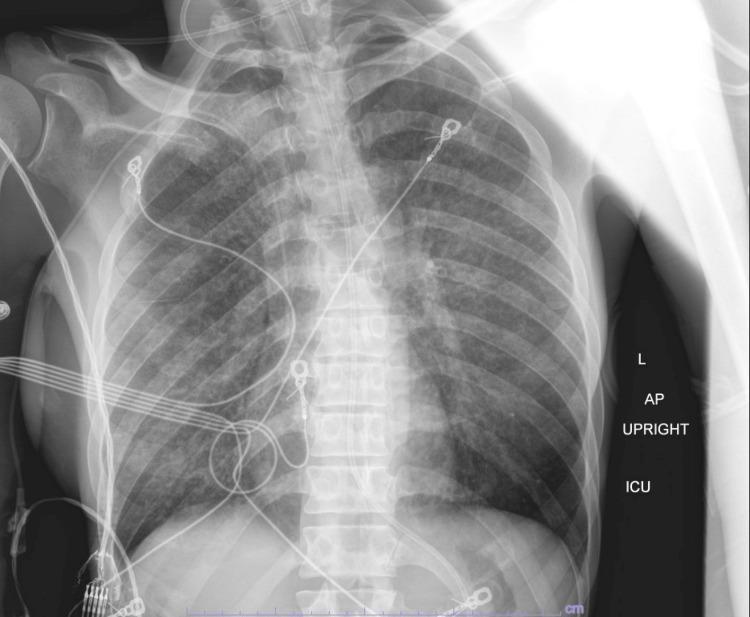
Classic picture:
- Bilateral diffuse alveolar infiltrates (both lung fields, not respecting lobar/segmental boundaries)
- Rapid onset (within 1 week of precipitating event)
- No cardiac enlargement, no Kerley B lines (non-cardiogenic)
Berlin Definition (2012):
| Severity | PaO₂/FiO₂ (P/F Ratio) |
|---|---|
| Mild | 201–300 mmHg |
| Moderate | 101–200 mmHg |
| Severe | ≤ 100 mmHg |
Key teaching points:
- Diffuse bilateral opacities NOT fully explained by effusions, atelectasis, or nodules
- PCWP < 18 mmHg OR no evidence of CHF (to exclude cardiogenic pulmonary edema)
- Management: lung-protective ventilation (tidal volume 6 mL/kg IBW, plateau pressure ≤ 30 cmH₂O), prone positioning for severe ARDS (P/F ≤ 150)
6. Cardiogenic Pulmonary Edema — "Bat-Wing" / Perihilar Pattern
Classic picture (5 Cs):
- Cardiomegaly (CTR > 0.5)
- Cephalization of pulmonary vessels (upper lobe vessel prominence > lower lobe)
- Clouding — perihilar "bat-wing" opacity, interstitial haziness
- Costophrenic blunting — small bilateral pleural effusions
- Kerley B lines — short horizontal lines at peripheral lung bases (thickened interlobular septa from interstitial fluid)
ARDS vs Cardiogenic edema — key differentiator:
| Feature | ARDS | Cardiogenic Edema |
|---|---|---|
| Heart size | Normal | Enlarged |
| Distribution | Peripheral > perihilar | Perihilar "bat-wing" |
| Kerley B lines | Absent | Present |
| Pleural effusions | Rare | Common |
| Onset | After precipitant | With cardiac decompensation |
| BNP/NT-proBNP | Normal/low | Elevated |
7. Pleural Effusion
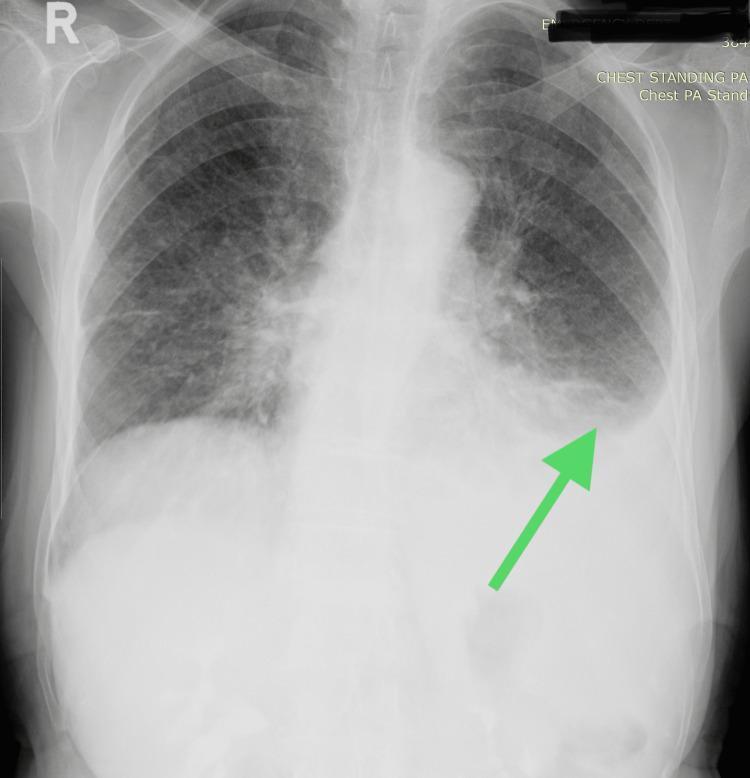
Classic picture:
- Blunting of costophrenic angle (needs ~200 mL to blunt on PA; ~50 mL on lateral)
- Meniscus sign — curved upper border tracking up the lateral chest wall
- Silhouette of diaphragm lost on the affected side

Key teaching points:
- Supine ICU films: effusions appear as homogeneous opacification of the entire hemithorax (fluid layers posteriorly)
- Large effusion → mediastinal shift away (distinguish from collapse, where shift is toward)
- Common ICU causes: CHF, sepsis (para-pneumonic), post-op, hypoalbuminemia
- Ultrasound is far more sensitive and guides drainage
8. Lobar Consolidation / Pneumonia

Classic picture:
- Dense, lobar/segmental opacity with maintained lung volume
- Air bronchogram sign — tubular air-filled bronchi visible within the opacified lung (patent airways surrounded by fluid-filled alveoli)
- Borders defined by fissures (distinguishes lobar from ARDS)

Silhouette sign (localizing consolidation):
| Structure Obscured | Location of Consolidation |
|---|---|
| Right heart border | Right middle lobe |
| Right hemidiaphragm | Right lower lobe |
| Left heart border | Lingula |
| Left hemidiaphragm | Left lower lobe |
| Aortic knuckle | Left upper lobe |
Consolidation vs Atelectasis:
| Feature | Consolidation | Atelectasis |
|---|---|---|
| Volume | Preserved or ↑ | Decreased |
| Mediastinal shift | None or away | Toward lesion |
| Air bronchogram | Present | Absent (usually) |
| Fissure displacement | None | Toward lesion |
9. Central Line Malposition & Complications
What to check on post-CVC insertion CXR:
- Tip position: Should be at SVC-RA junction (right tracheobronchial angle, ~T4–T6)
- No pneumothorax (occurs in ~1–3% of subclavian/IJ insertions)
- No mediastinal widening (hematoma from arterial injury)
- No new pleural effusion (hemothorax, infusion into pleural space)
Red flags:
- Tip too lateral → arterial placement (subclavian artery) — requires urgent removal
- Tip turned up the contralateral neck → guidewire malposition into opposite jugular
- New large pleural opacity after CVC placement → hemothorax or infusion extravasation
Quick Summary Table
| Finding | Key Radiographic Sign | Immediate Action |
|---|---|---|
| Right mainstem intubation | Left white-out + right hyperinflation | Pull ETT back 2–3 cm |
| Tension PTX | Contralateral mediastinal shift + hyperlucent lung | Needle decompression NOW |
| Simple PTX (ventilated) | Visceral pleural line, no shift | Chest tube |
| ARDS | Bilateral diffuse infiltrates, normal heart size | Lung-protective ventilation |
| Cardiogenic edema | Bat-wing + cardiomegaly + Kerley B | Diuresis, treat cardiac cause |
| Lobar pneumonia | Lobar opacity + air bronchogram | Antibiotics per clinical context |
| Pleural effusion | Costophrenic blunting, meniscus sign | Consider drainage if large/symptomatic |
| CVC malposition | Tip outside SVC, new opacity | Reposition or remove |
Clinical pearl: Every ICU CXR should be read systematically. Check all lines and tubes first (is anything malpositioned?), then read the lung fields, then the heart and mediastinum. A missed right mainstem intubation or unrecognized tension pneumothorax can be fatal.
This is a shared conversation. Sign in to Orris to start your own chat.