Principal of antimicrobial therapy pharmacology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, well-sourced content. Let me compile the full detailed answer:
Principles of Antimicrobial Therapy - Pharmacology
Antimicrobial therapy is guided by six interlocking principles: identifying the pathogen, determining susceptibility, choosing the right drug for the right site, applying pharmacokinetic/pharmacodynamic (PK/PD) optimization, understanding resistance, and practicing stewardship.
I. Selection of Antimicrobial Agents
Selection of the most appropriate agent requires knowledge of:
- The identity of the microorganism
- The susceptibility of the organism to the agent
- The site of infection
- Patient factors (age, immune status, renal/hepatic function, allergy)
- The safety and efficacy of the antimicrobial
- The cost of therapy
Most patients require empiric therapy - immediate drug administration prior to bacterial identification and susceptibility testing. Therapy is subsequently adjusted once culture results return.
- Lippincott Illustrated Reviews: Pharmacology, p. 907
II. Identifying the Infecting Organism
Characterization of the pathogen is central to appropriate therapy. Methods include:
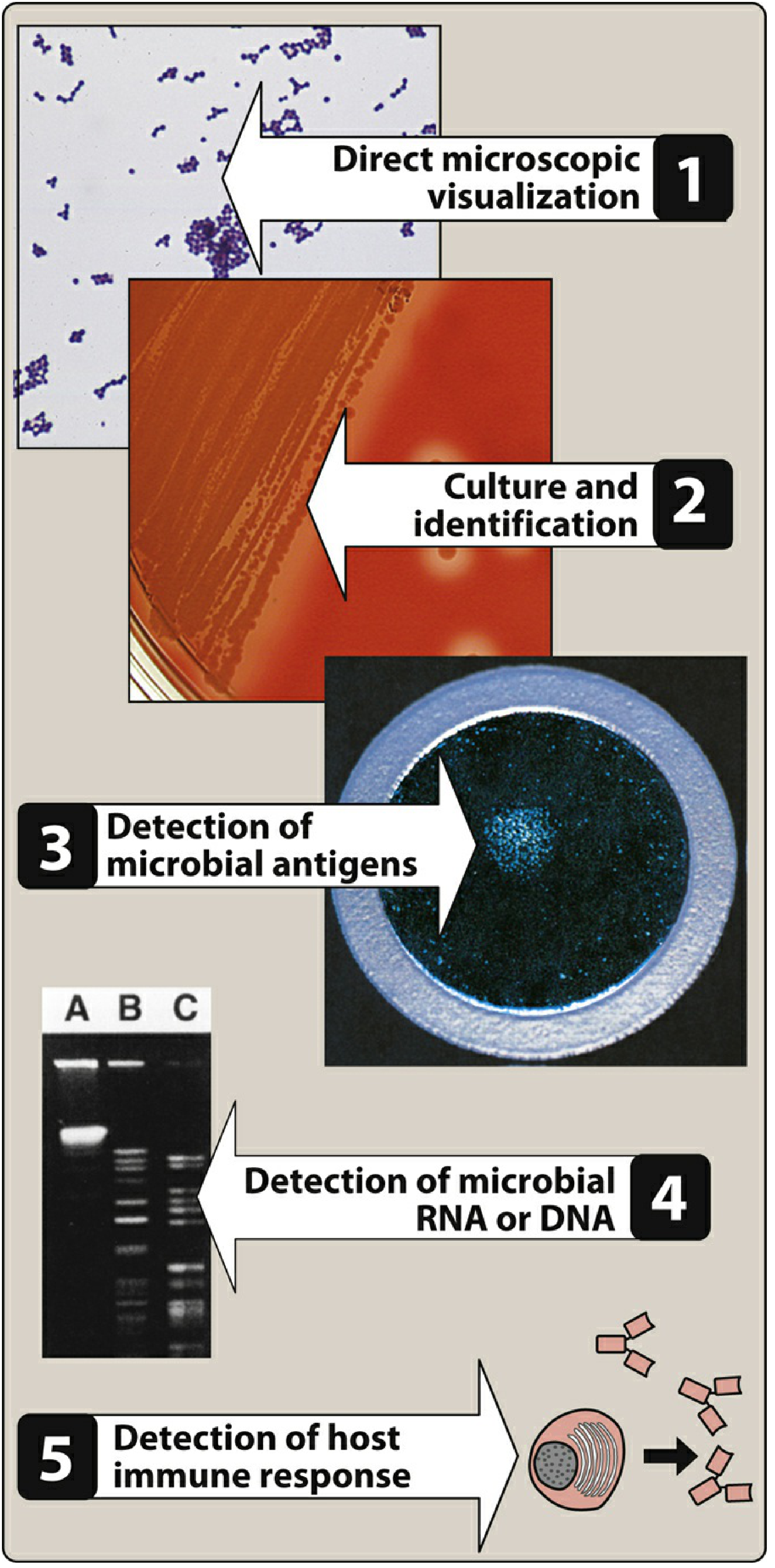
- Direct microscopic visualization (Gram stain) - rapid assessment for normally sterile body fluids (blood, CSF, pleural, synovial, urine)
- Culture and identification - definitive diagnosis; must be obtained before antibiotics are started
- Antigen detection
- Nucleic acid detection (PCR, MALDI-TOF MS) - highly accurate, rapid; allows detection of resistant genes (e.g., mecA gene for MRSA)
- Host immune response (serology)
Key clinical note: Culture specimens must be collected before initiating antibiotic therapy. A negative culture on an already-treated patient cannot differentiate absence of organism from antibiotic effect.
III. Empiric Antimicrobial Therapy
When culture results are unavailable, empiric therapy selection is guided by:
- Timing: Sepsis with hypotension requires antibiotics within 1 hour of diagnosis; neutropenic patients and meningitis require immediate treatment
- Site of infection: Identifies the most probable pathogen (e.g., urinary vs. pulmonary vs. CNS)
- Patient history: Age, prior infections, recent antibiotics, immune status, travel history, hospital vs. community acquisition
- Local antibiogram: Summary of local susceptibility patterns; used to guide empiric drug choices
Broad-spectrum therapy is appropriate initially when the organism is unknown or polymicrobial infection is likely. De-escalation to targeted therapy follows culture results.
IV. Antimicrobial Susceptibility Testing
Disk Diffusion (Kirby-Bauer)
Paper disks containing antibiotics are placed on agar. The drug diffuses outward, creating a zone of inhibition. Zone diameter is measured and compared to CLSI standards to classify the organism as susceptible (S), intermediate (I), or resistant (R).
Minimum Inhibitory Concentration (MIC)
The MIC is the lowest antimicrobial concentration that prevents visible bacterial growth after 24 hours. It provides a quantitative measure of in vitro susceptibility. Serial broth dilutions are inoculated with a standardized inoculum, and the lowest clear tube = MIC.
Minimum Bactericidal Concentration (MBC)
The MBC is the lowest concentration that kills ≥99.9% (3-log reduction) of the original inoculum. MBC is rarely determined in routine clinical practice due to labor intensity.
- Jawetz Melnick & Adelberg's Medical Microbiology 28E, p. 775
V. Bacteriostatic vs. Bactericidal Drugs
| Property | Bacteriostatic | Bactericidal |
|---|---|---|
| Definition | Arrests growth/replication at achievable levels | Kills ≥99.9% of organisms within 18-24 hours |
| MBC:MIC ratio | >4 | ≤4 |
| Examples | Tetracyclines, macrolides, sulfonamides, linezolid, clindamycin | Penicillins, cephalosporins, aminoglycosides, fluoroquinolones, vancomycin |
| When bactericidal preferred | Endocarditis, meningitis, immunocompromised hosts | - |
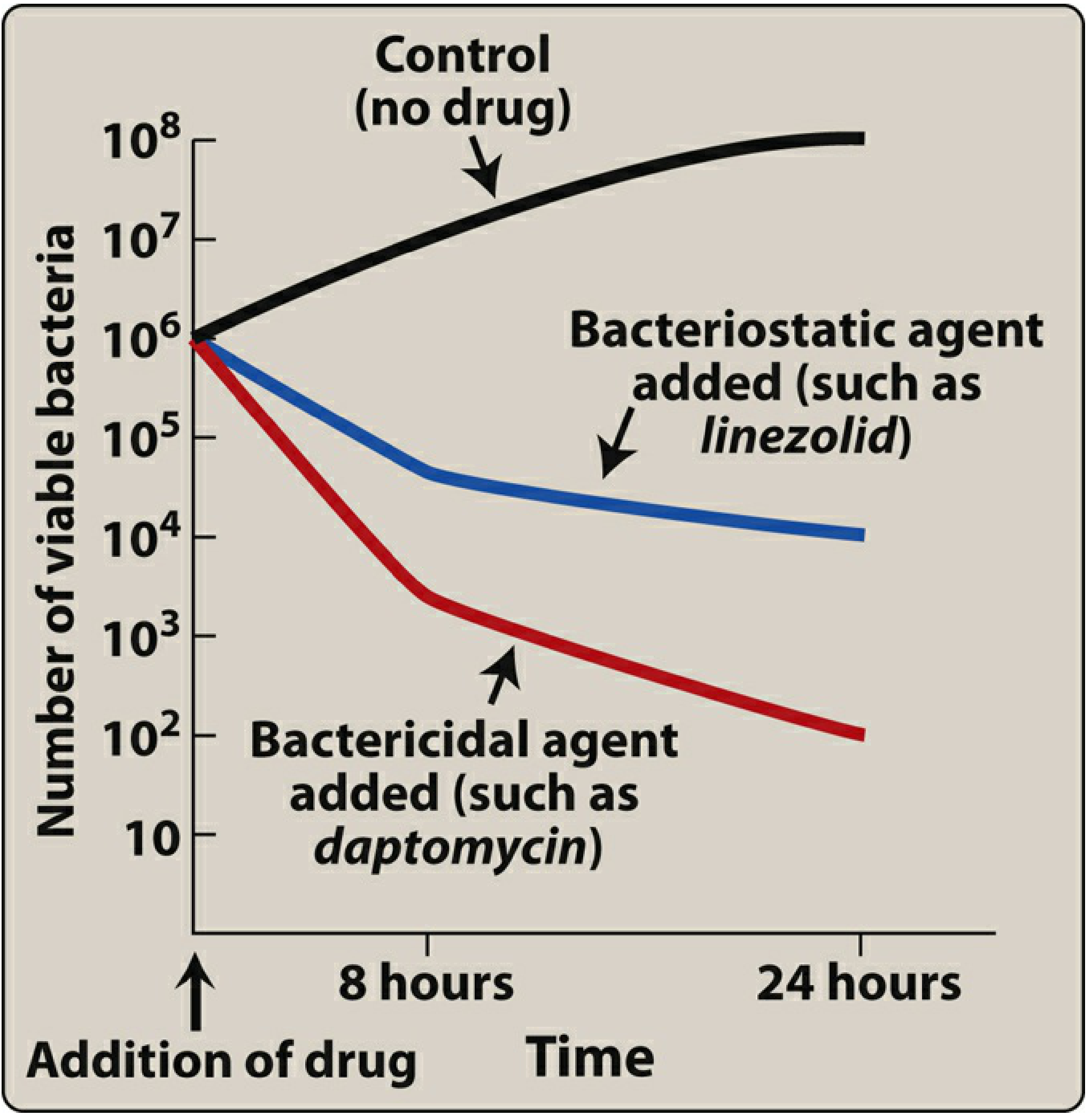
Note: This classification is context-dependent. Linezolid is bacteriostatic against S. aureus and enterococci but bactericidal against most S. pneumoniae. Recent evidence shows bacteriostatic and bactericidal agents have similar efficacy for many common infections.
- Lippincott Illustrated Reviews: Pharmacology, p. 914
VI. Pharmacokinetics and Pharmacodynamics (PK/PD)
Rational dosing is based on three key PK/PD parameters:
A. Concentration-Dependent Killing
- Killing rate increases as drug concentration rises above the MIC
- The higher the peak:MIC ratio, the greater the killing
- Best parameter: Peak:MIC ratio (Cmax/MIC)
- Examples: Aminoglycosides, fluoroquinolones, daptomycin, metronidazole
- Dosing strategy: Once-daily (high-dose) bolus to achieve high peak levels
B. Time-Dependent (Concentration-Independent) Killing
- Efficacy is determined by how long drug levels remain above the MIC
- Increasing concentration beyond the MIC does not increase killing
- Best parameter: %T>MIC (time drug concentration exceeds MIC)
- Penicillins: need T>MIC for ~50% of dosing interval
- Cephalosporins: ~60% T>MIC
- Examples: Beta-lactams (penicillins, cephalosporins), macrolides, clindamycin, linezolid
- Dosing strategy: Extended infusions (3-4 hours) or continuous infusions rather than bolus
C. AUC/MIC-Dependent Killing
- Efficacy best predicted by total drug exposure relative to MIC
- Best parameter: AUC24/MIC ratio
- Examples: Fluoroquinolones, vancomycin
D. Postantibiotic Effect (PAE)
-
Persistent suppression of bacterial growth after drug levels fall below the MIC
-
Long PAE drugs (aminoglycosides, fluoroquinolones) can be dosed once daily
-
Short/no PAE: beta-lactams (against gram-negative rods) - require more frequent dosing or continuous infusion
-
Lippincott Illustrated Reviews: Pharmacology, p. 921
VII. Effect of Site of Infection
Adequate drug levels must reach the site of infection. Key considerations:
| Site | Special Requirements |
|---|---|
| CNS (meningitis) | Drug must penetrate blood-brain barrier (BBB); bactericidal agents required; e.g., penicillin G, ceftriaxone, vancomycin. Lipophilic drugs cross BBB better |
| Endocarditis | Bactericidal drugs mandatory; prolonged IV therapy required |
| Abscesses | Poor drug penetration; surgical drainage often necessary |
| Bone | Good penetration by fluoroquinolones, clindamycin, rifampin |
| Urine (uncomplicated UTI) | Blood levels less important; urinary concentration critical |
| Prostate/kidney (febrile UTI) | Blood levels matter; need agents with tissue penetration |
Drug concentration in urine may be reduced by renal insufficiency or urinary obstruction, making eradication more difficult.
- Campbell-Walsh-Wein Urology, p. relevant section
VIII. Patient Factors
- Renal insufficiency: Dose adjustments needed for renally cleared drugs (aminoglycosides, vancomycin, carbapenems, beta-lactams). Impaired kidneys may also fail to concentrate drugs in the urine.
- Hepatic insufficiency: Adjust drugs metabolized hepatically (metronidazole, clindamycin, chloramphenicol)
- Pregnancy: Many antibiotics are contraindicated (tetracyclines, fluoroquinolones, aminoglycosides)
- Immune status: Immunocompromised patients often require bactericidal agents and broader empiric coverage
- Age: Neonates lack certain drug-metabolizing enzymes; elderly have reduced renal clearance
- Drug allergies: Cross-reactivity between penicillins and cephalosporins (~1-2% true cross-reactivity)
IX. Routes of Administration
- Oral: For uncomplicated infections and stable patients; bioavailability varies widely by drug
- IV: Required for severe infections, poor oral absorption, or specific tissue penetration needs
- IV to oral (step-down): Once clinical improvement occurs, switch to oral agents with good bioavailability (fluoroquinolones, linezolid, metronidazole have near 100% oral bioavailability)
- Topical: Mupirocin (skin infections), ophthalmic drops, inhaled (tobramycin for CF)
X. Mechanisms of Antimicrobial Resistance
Resistance is a major threat to modern antimicrobial therapy. Mechanisms include:
| Mechanism | Examples |
|---|---|
| Enzymatic inactivation | Beta-lactamases destroy penicillins/cephalosporins; aminoglycoside-modifying enzymes |
| Altered target site | PBP-2a (MRSA mecA gene) prevents beta-lactam binding; altered 30S ribosome (aminoglycoside resistance) |
| Decreased permeability | Loss of porin channels reduces drug entry (carbapenem resistance in gram-negatives) |
| Efflux pumps | Active drug expulsion; common in fluoroquinolone and tetracycline resistance |
| Bypass pathway | MRSA uses alternative PBP-2a; VRE uses alternative cell wall precursors (D-Ala-D-Lac) |
| Biofilm formation | Polymicrobial biofilms reduce drug access and host immunity |
Resistance spreads via:
- Chromosomal mutation (spontaneous)
- Horizontal gene transfer: conjugation (plasmids), transformation, transduction
Antibiotic use exerts selection pressure, enriching resistant populations. Broad-spectrum agents (especially cephalosporins and fluoroquinolones) carry the highest risk of collateral damage to normal flora, promoting selection of resistant organisms and C. difficile.
- Medical Microbiology 9e; Goldman-Cecil Medicine; Jawetz Microbiology
XI. Combination Antimicrobial Therapy
Indications for combination therapy:
- Synergy - two drugs together kill more than either alone (e.g., beta-lactam + aminoglycoside for serious gram-negative infection)
- Broad-spectrum empiric coverage when pathogen is unknown
- Prevention of resistance emergence (e.g., tuberculosis treatment: INH + RIF + PZA + EMB)
- Polymicrobial infections requiring coverage of multiple organisms
Risks of combination therapy:
- Increased toxicity
- Antagonism (possible with bacteriostatic + bactericidal combinations in some settings)
- Cost
- Disruption of normal flora
XII. Antibiotic Stewardship
Antimicrobial stewardship is the systematic effort to optimize antibiotic prescribing:
- Treat based on clinical indication, not just a positive culture (e.g., asymptomatic bacteriuria generally should not be treated)
- De-escalate from broad- to narrow-spectrum therapy once the pathogen is identified
- Use shortest effective duration
- Avoid antibiotics for viral infections
- Monitor local resistance patterns (antibiogram)
As stated in Campbell-Walsh-Wein: "The decision to initiate antibiotic therapy should not be based on treating a positive urine culture alone; rather clinical presentation in conjunction with urine testing should be considered, and we must assess the likelihood that the patient will benefit from or be harmed by antibiosis."
Inappropriate antibiotic use drives collateral damage - selection of multidrug-resistant organisms, C. difficile infection, disruption of microbiome, and adverse drug effects.
Summary Table: Key PK/PD Concepts
| Parameter | Drug Class | Strategy |
|---|---|---|
| Peak:MIC (Cmax/MIC) | Aminoglycosides, daptomycin | Once-daily high-dose bolus |
| %T>MIC | Beta-lactams, macrolides, clindamycin, linezolid | Frequent dosing or extended infusion |
| AUC24/MIC | Fluoroquinolones, vancomycin | Balanced dosing; TDM |
| Postantibiotic effect | Aminoglycosides, fluoroquinolones | Once-daily dosing feasible |
Sources: Lippincott Illustrated Reviews: Pharmacology, Chapter 28 (pp. 907-922); Jawetz, Melnick & Adelberg's Medical Microbiology 28E (pp. 774-776); Campbell-Walsh-Wein Urology; Medical Microbiology 9e
This is a shared conversation. Sign in to Orris to start your own chat.