Endoscopic ultrasound
Reading File
Finding Sources
Searching the Web
endoscopic ultrasound EUS indications technique clinical applications 2024
Searching PubMed
"endoscopic ultrasound"[MeSH Terms] AND "clinical applications"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have rich content from multiple textbooks and several images. Let me compile a comprehensive answer.
Endoscopic Ultrasound (EUS)
What is EUS?
Endoscopic ultrasound combines traditional mucosal endoscopy with a separate ultrasound probe mounted on the echoendoscope tip. Because the pancreas, bile duct, and mediastinal structures lie within a few millimeters of the GI lumen, placing the transducer intraluminally allows use of higher ultrasound frequencies (7.5-20 MHz) than transcutaneous scanning - yielding far superior resolution at the cost of reduced penetration depth. This makes EUS uniquely able to characterize the five-layer wall structure of the GI tract and adjacent organs in real time.
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 182
- Clinical Gastrointestinal Endoscopy Expert Consult, 3e
Instrument Types
| Type | Ultrasound Arrangement | Optics | Primary Use |
|---|---|---|---|
| Radial echoendoscope | Radially arranged (360° scan) | Forward-viewing | Diagnostic staging (esophagus, stomach) |
| Linear echoendoscope | Linearly arranged (alongside needle path) | Side-viewing | Guided biopsy (FNA/FNB), therapeutic procedures |
The linear scope has a working channel like an ERCP scope, allowing real-time needle visualization during EUS-FNA. The radial scope gives a more intuitive anatomical cross-section but cannot guide needles in real time.
- Bailey and Love's, p. 182
GI Wall Layers on EUS
EUS resolves the GI wall into five distinct layers:
| Layer | Appearance | Tissue Correlate |
|---|---|---|
| 1 | Hyperechoic | Interface/superficial mucosa |
| 2 | Hypoechoic | Deep mucosa (muscularis mucosae) |
| 3 | Hyperechoic | Submucosa |
| 4 | Hypoechoic | Muscularis propria |
| 5 | Hyperechoic | Serosa/adventitia |
Identifying which layer a lesion arises from directs both the diagnosis (e.g., lipoma from layer 3, GIST from layer 4) and the T-stage.
Indications
Diagnostic
- Staging of esophageal/gastric/rectal malignancy (T and N staging)
- Staging of hepatobiliary malignancy (pancreatic cancer, cholangiocarcinoma)
- Subepithelial lesions (SELs) - characterizing intramural masses (lipoma, GIST, carcinoid, varices, cysts)
- Diagnosis of choledochal microlithiasis / biliary sludge
- Evaluation of chronic pancreatitis - parenchymal and ductal criteria
- Idiopathic recurrent acute pancreatitis (IRAP) - 7-point checklist including bile duct stones, pancreatic masses, pancreas divisum, SOD, CP, AIP
- Suspected pancreatic masses - EUS detects small masses missed by CT
Therapeutic / Interventional
-
EUS-FNA/FNB - tissue acquisition from pancreatic masses, lymph nodes, submucosal lesions, left adrenal, portal adenopathy
-
Transgastric drainage of pancreatic pseudocysts and abscesses (EUS cystgastrostomy)
-
Coeliac plexus neurolysis/block for pain management in pancreatic cancer
-
Biliary interventions - EUS-guided biliary drainage (increasingly performed)
-
EUS-guided gastroenterostomy for gastric outlet obstruction
-
Bailey and Love's, Table 9.6, p. 182
EUS in Tumor Staging
Esophageal Cancer
EUS is the most accurate pre-operative staging modality for esophageal cancer:
- T staging accuracy: 87-92% (vs. CT: 51-74%)
- N staging sensitivity: 92-95%, specificity 50-54%
- EUS is superior to CT for primary tumor and regional nodal status
- EUS-FNA improves N-staging accuracy to >90% for celiac axis nodes
- CT or MRI should be performed before EUS to exclude distant metastases
- Post-chemoradiotherapy: a ≥50% reduction in tumor cross-sectional area correlates with treatment response, though EUS cannot reliably distinguish residual cancer from inflammation/fibrosis
EUS image - esophageal tumour with adventitial invasion:
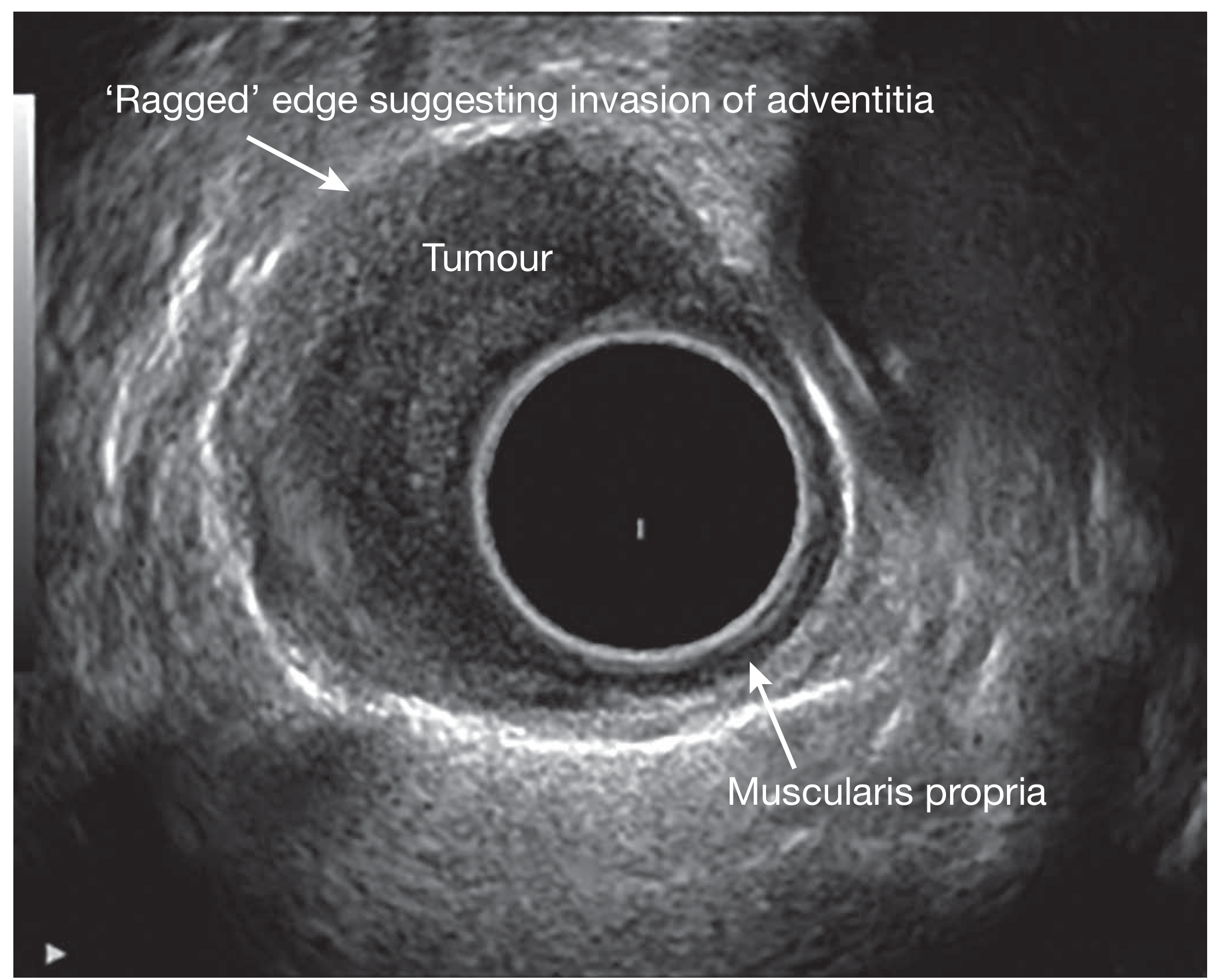
EUS image of an oesophageal tumour. The 'ragged' edge at the top indicates invasion into the adventitia (T3/T4 disease). The intact muscularis propria layer is visible at the bottom. - Bailey and Love's, Fig. 9.20
- Yamada's Textbook of Gastroenterology, 7e, p. 976
EUS-FNA (Fine Needle Aspiration)
EUS-FNA is performed using the linear echoendoscope with real-time needle visualization. A needle (typically 22G or 25G; 19G for core biopsy) is passed through the working channel and directed into the target lesion under continuous ultrasound guidance.
EUS-FNA image - pancreatic head mass:
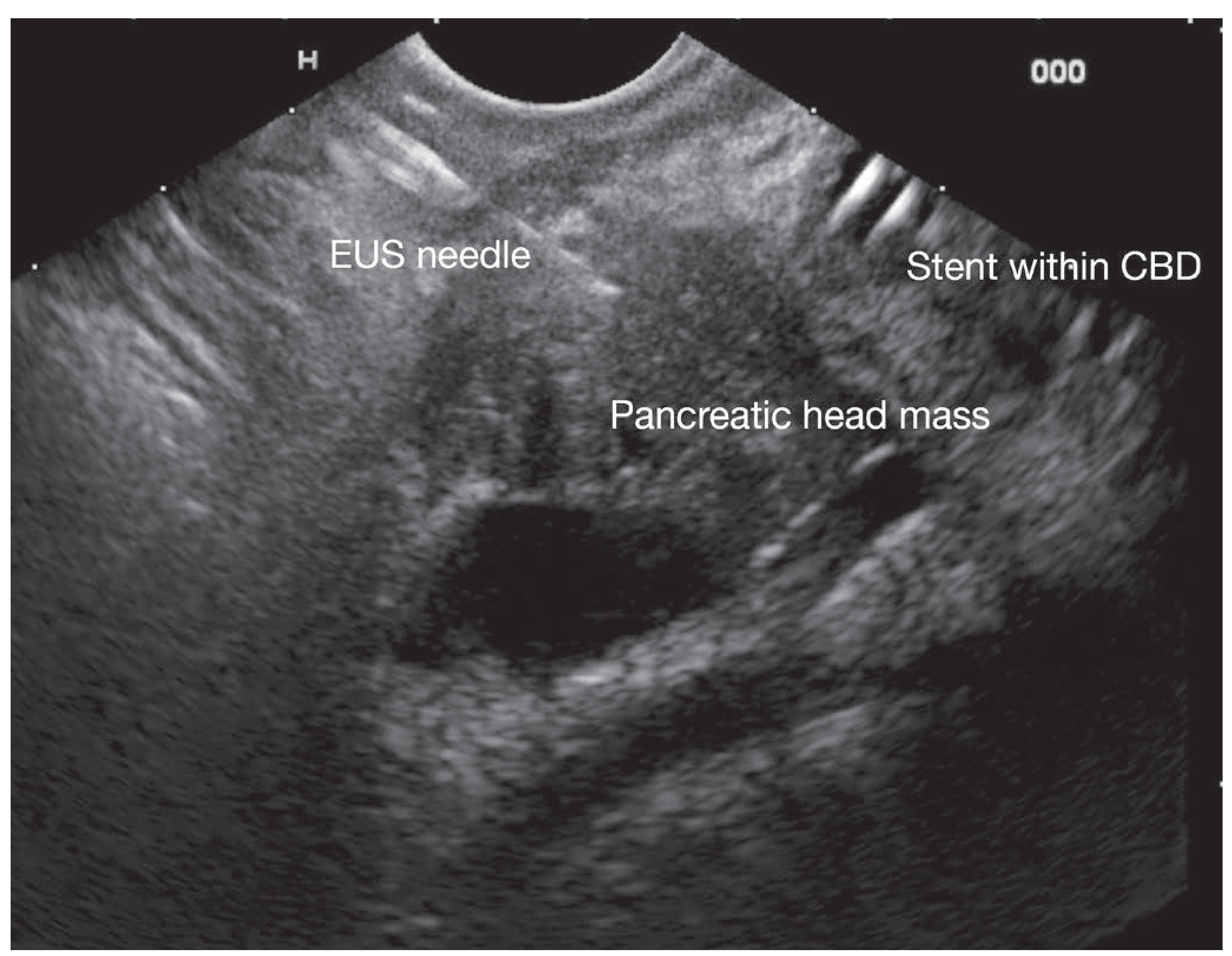
EUS-guided FNA of a pancreatic head mass. The EUS needle is clearly visible entering the mass. A biliary stent is also visible within the CBD (common bile duct). - Bailey and Love's, Fig. 9.21
Key EUS-FNA targets:
- Pancreatic masses and cysts
- Paraesophageal and coeliac lymph nodes
- Submucosal GI lesions
- Portal lymphadenopathy
- Left adrenal gland and left hepatic masses
- Mediastinal lesions
Newer fine-needle biopsy (FNB) needles (e.g., fork-tip, Franseen design) provide tissue cores with preserved architecture, improving histological diagnosis and enabling immunohistochemistry - particularly useful for autoimmune pancreatitis (IgG4 staining, obliterative phlebitis).
EUS in Chronic Pancreatitis
EUS is exquisitely sensitive for early chronic pancreatitis (CP) due to proximity to the pancreas, allowing high-frequency scanning. EUS criteria are divided into:
Parenchymal criteria:
- Inhomogeneity
- Hyperechoic foci
- Hyperechoic strands
- Lobularity
- Pseudocysts
Ductal criteria:
- Ductal dilation (≥3 mm head; ≥2 mm body; ≥1 mm tail)
- Hyperechoic main duct margins
- Irregular main duct margins
- Visible side branches
A quantitative score using 9 criteria is most reliable when clearly normal (≤2 criteria) or clearly abnormal (≥5 criteria) - predictive value 85% at these thresholds. Intermediate scores (3-4 criteria) are diagnostically uncertain and may represent early disease.
EUS image - chronic pancreatitis with intraductal stone:
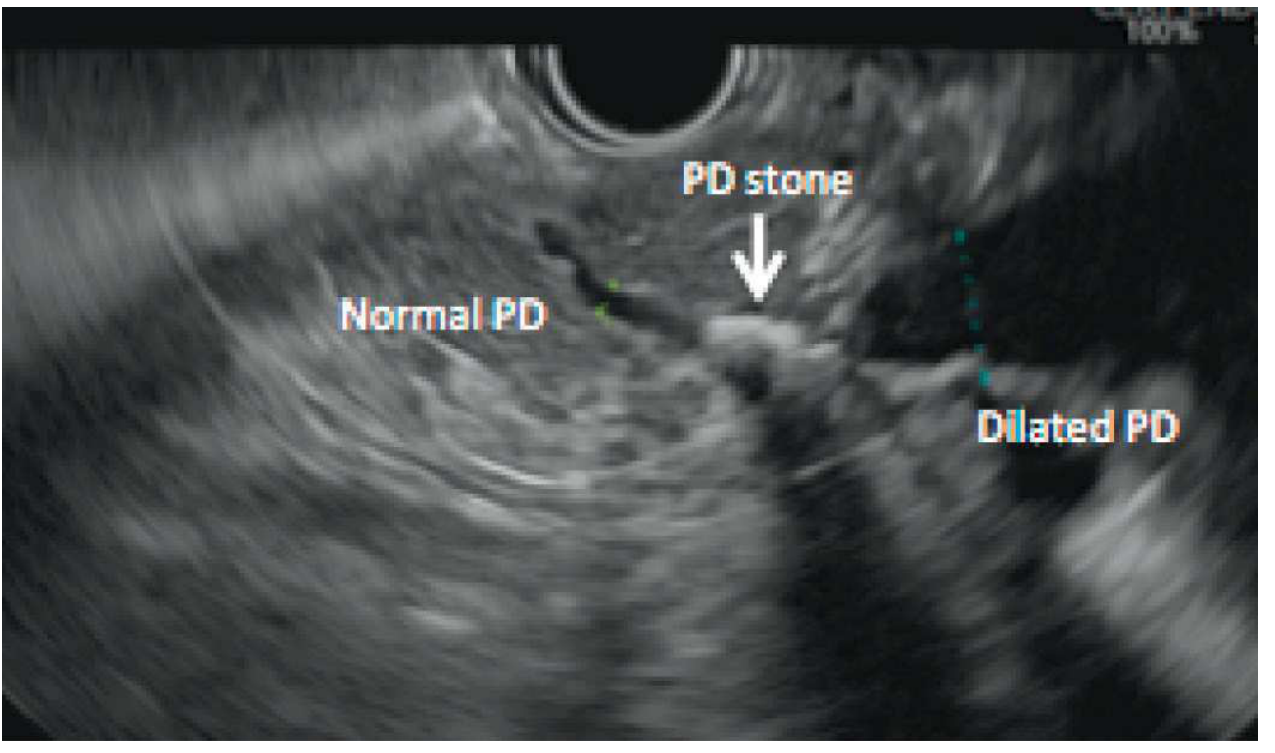
EUS showing a calcified intraductal stone in the pancreatic head (PD stone, arrow) with upstream normal duct and downstream dilation. - Clinical GI Endoscopy, Fig. 59.4
EUS in Subepithelial Lesions (SELs)
Key EUS features assessed for any intramural mass:
| Feature | What to Assess |
|---|---|
| Location | Organ + position |
| Size | 3 dimensions |
| Background echogenicity | Hypo/hyper/anechoic |
| Focal echogenicity | Foci present/absent |
| Shape/margins | Round, oval; smooth vs. irregular |
| Margin definition | Well- vs. poorly-defined |
| Wall layer of origin | Mucosa / submucosa / muscularis propria |
| Invasion | T-stage |
Characteristic appearances:
-
Lipomas: Brightly hyperechoic, uniform, well-demarcated, layer 3 (submucosal), easily deformed by transducer
-
Varices: Anechoic, vermiform, nearly always in groups
-
GISTs: Hypoechoic, layer 4 (muscularis propria) origin, malignant risk ↑ with size >3 cm, irregular margins, echogenic foci
-
EUS sensitivity/specificity for distinguishing lesion types: 64-92% / 80-100%
-
Clinical GI Endoscopy Expert Consult, 3e, p. [block5]
EUS vs. Other Modalities
| Modality | Advantage of EUS |
|---|---|
| CT scan | Better T-staging, detects small pancreatic masses, more sensitive for biliary sludge/stones |
| MRCP | Superior for biliary sludge/stones, luminal visualization, tissue acquisition; combined yield ~50% in IRAP (complementary) |
| Transcutaneous US | Far higher resolution due to intraluminal positioning and higher frequencies |
| ERCP | Non-invasive alternative for diagnosis (ERCP reserved for treatment) |
Training Requirements and Complications
EUS requires dedicated training in both scope manipulation and image interpretation. The wide, relatively inflexible echoendoscope typically requires sedation - many units use propofol-based anaesthesia for complex therapeutic procedures.
Complications:
-
Diagnostic EUS: Oversedation, esophageal perforation (rare)
-
Therapeutic EUS (FNA/drainage): Haemorrhage, perforation, pancreatitis (rare, <1% for pancreatic FNA), infection
-
All patients undergoing therapeutic EUS require a normal coagulation screen beforehand
-
Bailey and Love's Short Practice of Surgery, 28th ed., p. 182
Summary
EUS is a versatile tool occupying a unique niche - it provides high-resolution, real-time imaging of structures adjacent to the GI lumen combined with the ability to obtain tissue under direct ultrasound guidance. Its main clinical roles are:
- Cancer staging (GI, pancreatic, hepatobiliary)
- Pancreatic disease (masses, chronic pancreatitis, cysts)
- Tissue acquisition (FNA/FNB)
- Biliary stone detection (especially microlithiasis)
- Therapeutic drainage (pseudocysts, biliary)
- Pain palliation (coeliac plexus block)
This is a shared conversation. Sign in to Orris to start your own chat.