Pprom at 29 weeks in previous lscs management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Searching PubMed
PPROM prior cesarean section management outcome
Reading File
Loading Image
I now have all the information needed to provide a comprehensive answer. Here is the full management guide for PPROM at 29 weeks in a patient with a previous LSCS (Lower Segment Caesarean Section):
PPROM at 29 Weeks with Previous LSCS — Management
At 29 weeks, PPROM falls in the early preterm (23–31 weeks) category. The presence of a previous LSCS adds specific considerations around mode of delivery, risk of scar dehiscence/uterine rupture, and interpretation of fetal monitoring.
Management Algorithm (Creasy & Resnik's Maternal-Fetal Medicine)
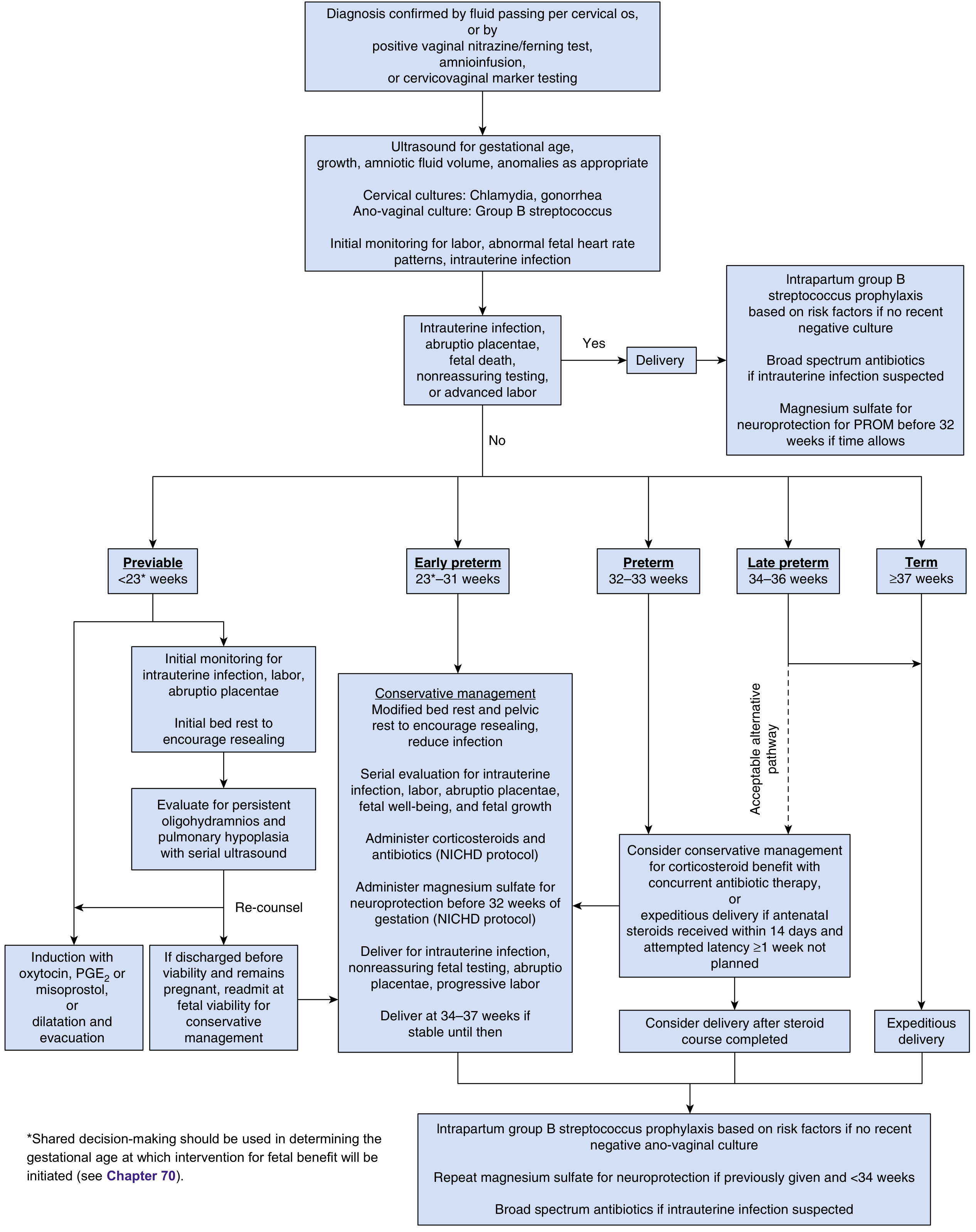
Step 1 — Confirm Diagnosis
- Fluid passing per cervical os on speculum examination
- Positive nitrazine/ferning test
- Cervicovaginal biochemical marker testing (IGFBP-1, PAMG-1)
- Avoid digital vaginal examination
Step 2 — Initial Assessment
After confirming rupture:
| Assessment | Detail |
|---|---|
| Gestational age | Confirm by dates + USS (avoid BPD alone if oligohydramnios — use HC) |
| Fetal presentation | Important in ex-LSCS (risk of cord prolapse, malpresentation) |
| Amniotic fluid volume | AFI / maximal vertical pocket — low volume predicts shorter latency |
| Fetal well-being | Continuous CTG monitoring initially |
| Signs of intrauterine infection | Maternal pyrexia, tachycardia, uterine tenderness, offensive discharge, fetal tachycardia, raised CRP/TLC |
| GBS carrier status | Culture results within 6 weeks, or empiric approach |
| Uterine scar assessment | USS lower uterine segment thickness; watch for scar tenderness |
Deliver immediately if: intrauterine infection (chorioamnionitis), abruption, non-reassuring fetal status, advanced labor, fetal transverse lie with advanced cervical dilation, or HIV with high viral load.
Step 3 — Expectant/Conservative Management (if no immediate delivery indication)
Since 29 weeks is remote from term, expectant management is the default to gain fetal maturity, unless there is an indication for immediate delivery.
A. Corticosteroids (most important intervention)
- Betamethasone 12 mg IM × 2 doses, 24 hours apart (or Dexamethasone 6 mg IM × 4 doses, 12 hours apart)
- Reduces RDS, IVH, NEC, and neonatal mortality
- Indicated for all preterm PROM <34 weeks
B. Antibiotics for Latency (NICHD Protocol — standard of care)
- IV Ampicillin 2 g every 6 hours + IV Erythromycin 250 mg every 6 hours × 48 hours
- Followed by oral Amoxicillin 250 mg every 8 hours + oral Erythromycin 333 mg every 8 hours × 5 days
- Avoid Amoxicillin-Clavulanate (co-amoxiclav) — associated with increased risk of neonatal necrotizing enterocolitis
- Alternatives if shortages: oral ampicillin, azithromycin, clarithromycin
- Prolongs pregnancy, reduces chorioamnionitis, reduces neonatal infectious morbidity
- Reduces frequencies of neonatal sepsis, IVH, RDS at <32 weeks' gestation
C. Magnesium Sulfate for Neuroprotection
- Indicated for PPROM before 32 weeks
- MgSO₄ 6 g IV bolus → 2 g/hour infusion × 12 hours (NICHD-MFMU protocol)
- Reduces cerebral palsy (4.2% vs 7.3%; P = .004), IVH, PVL, and developmental delay
- Administer even if delivery is not immediately planned
D. Tocolysis
- Not routinely recommended for prolonging latency in PPROM
- May be considered short-term (48 hours only) to facilitate steroid administration or maternal transfer before 34 weeks, in the absence of infection or abruption
- No prophylactic tocolysis before contractions; therapeutic tocolysis after contractions has no proven benefit
- Extra caution in previous LSCS: uterine scar makes aggressive tocolysis riskier
E. DVT Prophylaxis
- Bed rest increases DVT risk
- Leg exercises, compression stockings, sequential compression devices
- Weigh subcutaneous heparin against bleeding/anaesthesia risks
Step 4 — Fetal Surveillance During Conservative Management
- CTG at least daily (fetal heart rate abnormalities from cord compression occur in 32–76%)
- Biophysical profile (BPP) if NST equivocal — note: BPP may be confounded by oligohydramnios
- Serial USS for fetal growth, AFV, and lower uterine segment thickness
Step 5 — Timing of Delivery
- Planned delivery at 34–37 weeks if conservatively managed and stable
- Immediate delivery at any gestation for: chorioamnionitis, abruption, non-reassuring fetal testing, advanced labor
- In stable patients, plan to deliver by 34 weeks
Key Additional Considerations — Previous LSCS
These are specific to the scar uterus and significantly influence management:
1. Mode of Delivery
- Previous LSCS is not a contraindication to vaginal delivery in PPROM, but must be individualized
- At 29 weeks, the fetal size is small — vaginal birth after caesarean (VBAC) may be considered
- However, cervical ripening with prostaglandins (misoprostol, PGE₂) is CONTRAINDICATED in a scarred uterus due to high risk of uterine rupture
- If induction is needed, oxytocin is used cautiously with continuous CTG monitoring
- If labour fails to progress or there are signs of scar dehiscence → emergency LSCS
2. Uterine Rupture Risk
- Prior LSCS scars carry ~0.5–0.9% uterine rupture risk in labour (higher with prior classical/inverted-T incisions)
- Classical caesarean scar (vertical uterine incision): much higher rupture risk — elective repeat LSCS strongly preferred regardless of PPROM
- Continuous intrapartum CTG is mandatory — variable/late decelerations, sudden fetal bradycardia, loss of uterine contraction pattern, maternal haemorrhage = warning signs
- Lower threshold for proceeding to repeat LSCS if labour does not progress well
3. Placenta Praevia / Morbid Placentation
- In previous LSCS, rule out placenta praevia/accreta/increta/percreta by USS — these mandate delivery by LSCS
- If placenta praevia confirmed → elective repeat LSCS, not expectant vaginal management
4. Intrapartum GBS Prophylaxis
- Regardless of prior antibiotic therapy, intrapartum GBS prophylaxis is required if:
- GBS carrier known
- Carrier status unknown and delivering preterm
5. NICU Availability
- Conservative management must occur in a centre with Level III NICU and capacity for emergency LSCS
- If not available, arrange in-utero transfer
Summary Framework
| Phase | Key Actions |
|---|---|
| Diagnosis | Speculum exam, nitrazine/ferning, USS for GA + AFV |
| Immediate exclusions | Rule out infection, abruption, cord prolapse, malpresentation |
| Corticosteroids | Betamethasone × 2 doses |
| Antibiotics | Ampicillin + Erythromycin (NICHD protocol × 7 days) |
| Neuroprotection | MgSO₄ 6g IV → 2g/hr (<32 wks) |
| Tocolysis | Short-term only for steroid benefit, avoid if infection/abruption |
| Surveillance | Daily CTG, serial USS, signs of chorioamnionitis |
| Deliver | Signs of infection, abruption, non-reassurance, or by 34–37 wks |
| Previous LSCS | No prostaglandins; oxytocin with caution; low threshold for repeat LSCS; rule out morbid placentation |
References:
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, Chapter 39 — Management of Premature Rupture of the Membranes
- ACOG Practice Bulletin on Prelabor Rupture of Membranes
This is a shared conversation. Sign in to Orris to start your own chat.