Neurological complication of cocaine and ketamine
cocaine neurological complications stroke seizure
ketamine neurotoxicity neurological effects
Neurological Complications of Cocaine and Ketamine
COCAINE
Mechanism of CNS Toxicity
1. Cerebrovascular Complications (most common neurological manifestation)
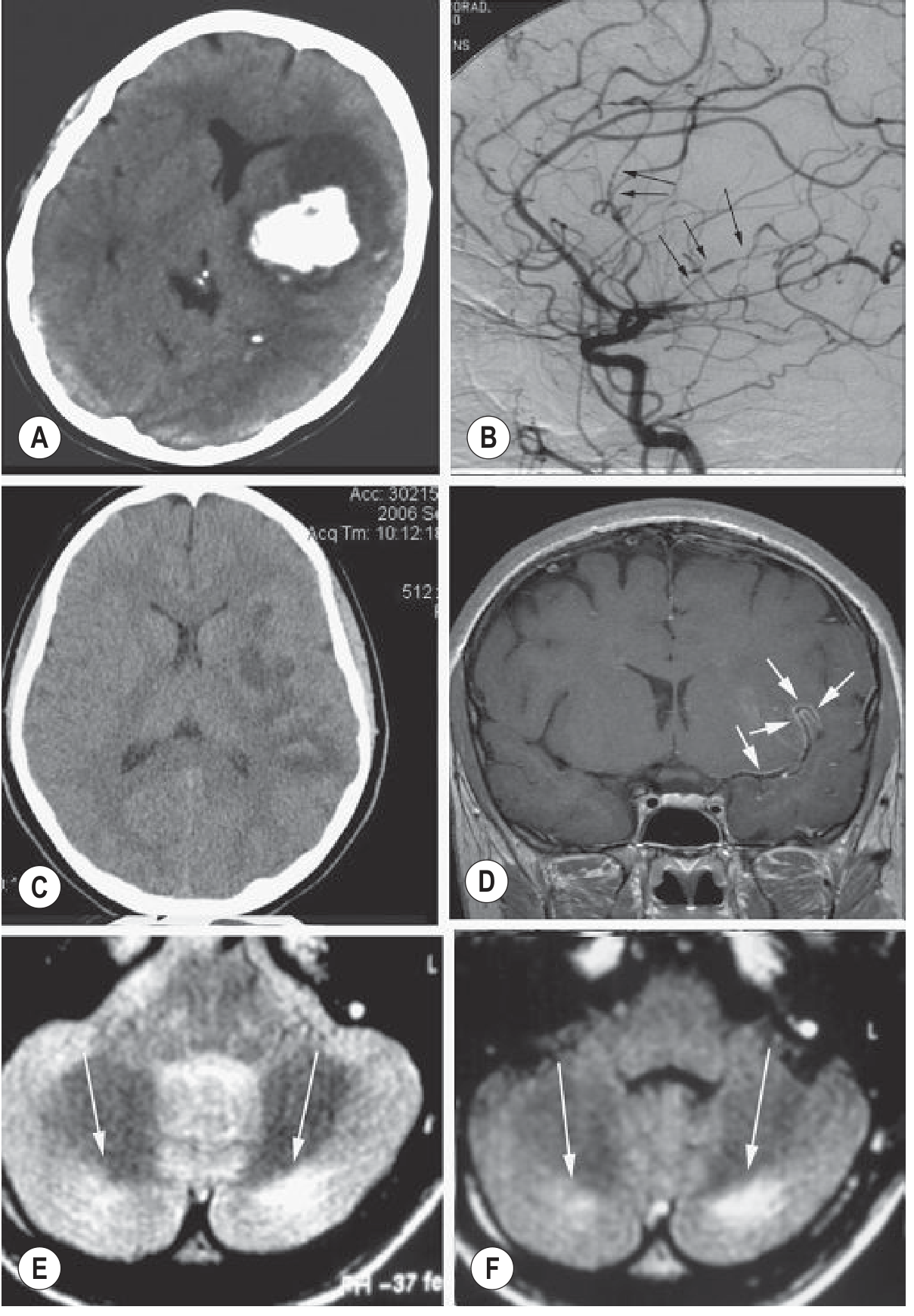
- Subarachnoid hemorrhage (SAH) and intracerebral hemorrhage (ICH) are both seen
- ~50% of patients have an underlying vascular lesion (AVM or aneurysm) that ruptures due to cocaine-induced surges in blood pressure and heart rate
- When no vascular malformation is found, hemorrhage is most commonly in the basal ganglia and thalamus
- Risk of hemorrhage increases substantially with concurrent alcohol abuse
- A 2024 systematic review and meta-analysis (PMID: 38072159) specifically examined aneurysmal SAH with cocaine consumption
- Vasospasm / vasoconstriction - focal constrictions visible on angiography ("pearl and string" sign)
- Vasculitis - caused by cocaine itself or its adulterants (contrast enhancement of vessel walls on MRI)
- Thrombosis - cocaine increases platelet response to arachidonic acid, raises thromboxane levels, enhancing platelet aggregation leading to thrombotic infarcts
- Emboli - from cardiac arrhythmias (cocaine-induced dysrhythmias can produce cardioembolic events)
- Subcortical white matter
- Middle cerebral artery territory
- Mesencephalic infarcts are more frequent when cocaine is combined with amphetamines
- Bilateral cerebellar infarction has also been reported
2. Seizures
- Single generalized tonic-clonic seizures (most common)
- Status epilepticus in overdose
- Can occur with any route of use (intranasal, smoked, intravenous)
- Particularly dangerous because they may herald a stroke or can be the presenting feature of ICH
3. Levamisole-associated Multifocal Inflammatory Leukoencephalopathy
4. Chronic Brain Atrophy
- Chronic cocaine users develop cerebral atrophy, particularly affecting the frontal lobe (most severely) followed by the temporal lobe
- The mechanism is believed to be chronic ischemia from repeated endothelial damage causing premature atherosclerosis
- Subcortical white matter changes from microvascular pathology accumulate over time
5. Movement Disorders
- "Crack dancing" - stereotyped repetitive movements
- Choreiform movements have been reported, related to dopaminergic excess in the basal ganglia
- These are typically reversible with cessation of use
6. Headache
7. CNS Infections
KETAMINE
Mechanism of CNS Effects
1. Acute Dissociative Syndrome ("K-hole")
- Dose-dependent effects ranging from mild disorientation and illusions to full dissociation
- At recreational doses: euphoria, altered sensory perception, depersonalization, "out of body" experience
- Higher doses: catatonia, complete dissociation, unresponsiveness with preserved airway reflexes
- Duration: ~1 hour after insufflation (snorting), up to 4-8 hours after oral ingestion
- Route of street use: predominantly insufflation, but also IM injection and oral routes - Rosen's Emergency Medicine
2. Psychosis and Psychiatric Complications
- Ketamine blocks NMDA receptors and reproduces both positive symptoms (hallucinations, delusions) and negative symptoms (blunted affect, social withdrawal) of schizophrenia - making it the pharmacological model of schizophrenia in research
- Chronic users, even at low doses, can experience persistent psychiatric symptoms similar to schizophrenia
- The NMDA hypofunction hypothesis: impaired NMDA receptors on GABAergic interneurons in prefrontal cortex lead to downstream hyperdopaminergia, explaining the psychosis
- Emergence reactions/delirium on recovery from anesthetic doses
3. Cognitive Impairment
- Chronic recreational use is associated with memory impairment (especially episodic and working memory)
- Persistent cognitive deficits have been documented in long-term ketamine abusers
- NMDA receptors are critical for long-term potentiation (LTP) - the cellular substrate of memory - explaining why their chronic blockade impairs cognition
4. Seizures
- Ketamine can increase seizure activity in a dose-dependent manner
- However, at sub-anesthetic doses it may actually raise the seizure threshold
- Seizures are more commonly a feature of high-dose toxicity, especially when street preparations are adulterated with stimulants
5. Increased Intracranial Pressure
- Ketamine increases cerebral blood flow (unique among anesthetics) - a concern in patients with TBI or raised ICP
- This effect is mediated via cerebral vasodilation
- This side effect can be minimized by concurrent benzodiazepine use
6. Neurological Signs with Overdose/High-Dose Intoxication
- Ataxia
- Nystagmus (horizontal, vertical; vertical and horizontal nystagmus are hallmarks of dissociative intoxication)
- Muscle rigidity and increased deep tendon reflexes
- Bizarre posturing, grimacing
- Hyperthermia (mild to severe)
- Rhabdomyolysis (from muscle hyperactivity or seizures) - can lead to myoglobinuric renal failure
- Rarely: intracerebral hemorrhage from severe hypertension (more commonly seen with PCP)
7. Neurotoxicity (chronic/high-dose)
- A 2025 review (PMID: 40015548) specifically addresses the molecular mechanisms of programmed cell death in ketamine-induced neuronal damage
- Mechanisms include: mitochondrial dysfunction, oxidative stress, apoptosis pathways
- Particularly concerning in the developing brain (neonatal/pediatric exposure) - Harriet Lane Handbook
- The metabolite hydroxynorketamine (HNK) has emerged as the mediator of antidepressant effects via AMPA receptor activation, but the neurotoxic pathways involve direct NMDA blockade-mediated apoptosis in neurons - Goldman-Cecil Medicine
8. Urological Complications (indirect neurological relevance)
- Chronic ketamine use causes a distinct uropathy (ketamine cystitis) - urinary frequency, nocturia, and in severe cases, upper urinary tract destruction
- This is not directly a neurological complication, but the associated chronic pain can have central sensitization consequences
Summary Comparison Table
| Feature | Cocaine | Ketamine |
|---|---|---|
| Primary mechanism | Monoamine reuptake blockade + sympathomimetic | NMDA receptor antagonism |
| Stroke (hemorrhagic) | Very common - basal ganglia/thalamus | Rare (mainly with severe HTN) |
| Stroke (ischemic) | Common - MCA territory, subcortical WM | Not a primary complication |
| Seizures | Common, threshold-lowering | Possible, dose-dependent |
| Psychosis | Paranoid psychosis (acute) | Schizophrenia-like (positive + negative symptoms) |
| Cognitive effects | Chronic atrophy, executive dysfunction | Memory impairment, chronic cognitive deficits |
| Vasculitis/Leukoencephalopathy | Yes (levamisole-associated) | No |
| ICP effects | Indirect (via hemorrhage) | Direct (increases cerebral blood flow) |
| Neurotoxicity (chronic) | Cerebral atrophy, microvascular WM changes | Neuronal apoptosis (NMDA-mediated) |
| Hallmark imaging | "Pearl and string" angiography; ICH on CT | No specific lesion pattern |
Any chronic neurological disorder.eho has left cocaine and ketamine use 1 month ago
cocaine cessation persistent neurological cognitive sequelae
cocaine abstinence cognitive impairment brain
ketamine chronic abuse cognitive psychiatric residual effects
ketamine use disorder cognitive neurotoxicity long term
PMID: 35502632
PMID: 40926573
PMID: 37148676
Chronic Neurological Disorders Persisting After Stopping Cocaine and Ketamine (1 Month into Abstinence)
COCAINE - Chronic/Persistent Neurological Disorders
1. Post-Stroke Neurological Deficits (most significant)
- Hemiparesis / hemiplegia - from MCA territory ischemic stroke (most common distribution)
- Aphasia - dominant hemisphere involvement
- Cerebellar ataxia - from posterior circulation infarcts (bilateral cerebellar infarction reported with cocaine)
- Hemianopia - from occipital or PCA territory involvement
- Basal ganglia / thalamic syndromes - from the typical sites of cocaine-related ICH (involuntary movements, sensory disturbances, thalamic pain)
A 2024 meta-analysis (PMID: 38072159) confirmed cocaine's strong association with aneurysmal SAH - patients surviving SAH carry permanent neurological and neuropsychological sequelae.
2. Chronic Cerebral Atrophy and Neurodegenerative Changes
- Frontal lobe atrophy is the most characteristic finding in chronic cocaine users - the frontal lobe is most severely affected, followed by the temporal lobe
- Mechanism: repeated endothelial damage → premature atherosclerosis → chronic ischemia → neuronal loss - Grainger & Allison's Diagnostic Radiology
- At 1 month abstinence, structural atrophy does NOT reverse - this is a fixed lesion
- Neurometabolic signature on MR spectroscopy: lower N-acetylaspartate (NAA, a marker of neuronal integrity), lower creatine, and higher myo-inositol (glial activation marker) in the medial prefrontal cortex - a profile that parallels Alzheimer's disease and mild cognitive impairment - 2023 meta-analysis, PMID: 37148676
3. Chronic Cognitive Impairment
| Domain Affected | Manifestation |
|---|---|
| Executive function | Poor planning, impulsivity, decision-making deficits |
| Working memory | Difficulty holding information in mind |
| Attention / concentration | Easily distracted, poor sustained attention |
| Processing speed | Slowed mental processing |
| Verbal learning | Difficulty learning new material |
- Frontally mediated functions are most impaired, consistent with the frontal atrophy pattern
- Dopaminergic dysfunction in prefrontal-striatal circuits persists well beyond acute withdrawal
4. Persistent Dopamine System Dysregulation - Anhedonia and Depression
- Chronic cocaine use depletes dopamine at nerve terminals through receptor downregulation and DAT upregulation
- At 1 month, dopaminergic recovery is incomplete - patients typically experience anhedonia (inability to feel pleasure), dysphoria, and depression that can persist for weeks to months
- This is not simply "feeling sad" - it represents a neurobiological state of dopamine D2 receptor hypofunction in the reward circuitry - Tintinalli's Emergency Medicine
- This "protracted withdrawal" phase carries significant relapse risk
5. White Matter Changes (Subcortical Leukoencephalopathy)
- Chronic microvascular ischemia produces diffuse subcortical and periventricular white matter hyperintensities on T2/FLAIR MRI
- These reflect small vessel disease accelerated by repeated vasospasm and endothelial injury
- Not reversible at 1 month abstinence
- Contribute to the cognitive slowing and executive dysfunction described above
6. Levamisole-Induced Leukoencephalopathy (if cocaine was adulterated)
- A subset of patients exposed to levamisole-adulterated cocaine develop multifocal inflammatory white matter lesions
- These can persist and even progress even after stopping cocaine - an immune-mediated process that may require immunosuppressive treatment
- MRI shows pseudo-tumoral inflammatory WM lesions
7. Seizure Disorder (Epilepsy)
- A single seizure during cocaine use is usually provoked and does not mandate long-term anticonvulsant treatment
- However, if the patient has underlying structural brain damage (prior stroke, WM changes), they are at increased risk for unprovoked recurrent seizures (i.e., epilepsy)
- At 1 month, provoked seizures from cocaine are no longer occurring, but if seizures continue, structural epilepsy must be considered
8. Movement Disorders (residual)
- Choreiform movements related to dopaminergic hypersensitivity usually resolve with abstinence but may take several weeks
- In patients with basal ganglia hemorrhage, permanent movement abnormalities (dystonia, choreic movements) may persist
KETAMINE - Chronic/Persistent Neurological Disorders
1. Persistent Psychosis / Schizophrenia-Like Disorder
- Chronic low-dose ketamine users can experience persistent psychiatric symptoms similar to schizophrenia - including both positive (delusions, hallucinations) and negative symptoms (blunted affect, avolition, social withdrawal) - Rosen's Emergency Medicine
- Mechanism: chronic NMDA receptor blockade on GABAergic interneurons → disinhibition of dopamine release → persistent dopaminergic dysregulation even after cessation
- At 1 month, these symptoms may still be active or worsening as neuroadaptation occurs
- Distinguishing drug-induced persistent psychotic disorder from primary schizophrenia is a key clinical challenge at this stage
2. Cognitive Impairment
| Domain | Finding |
|---|---|
| Memory (episodic + working memory) | Most consistently impaired |
| Executive function | Impaired planning, cognitive flexibility |
| Attention | Sustained attention deficits |
| Processing speed | Slowed cognition |
- A 2025 review in the American Journal of Psychiatry (PMID: 40926573) confirmed that frequent high-dose users (>1 g/day) show memory and executive function impairments that persist after cessation
- These deficits are worse in those who used daily at high recreational doses compared to infrequent users
3. Olney Lesions and Structural Neurotoxicity
- NMDA receptor antagonists produce Olney lesions - vacuolization and neuronal injury in specific brain regions, particularly the posterior cingulate and retrosplenial cortices, in animal models
- [PMID: 35502632] (2022 review): daily high-dose ketamine use in substance use disorder populations was associated with clear neurotoxic effects; Olney lesions and tau hyperphosphorylation are concerns with chronic high-dose exposure
- At 1 month post-cessation, if neuronal damage occurred, it is unlikely to reverse significantly
4. Persistent Dissociative Episodes / Flashbacks
- Some chronic users experience spontaneous dissociative episodes without the drug - similar to "flashbacks" described with hallucinogens
- Perceptual distortions, depersonalization, and derealization can recur in the weeks following cessation
- These typically diminish over weeks to months but can persist in heavy users
5. Cerebellar and Balance Dysfunction
- Chronic exposure to NMDA antagonists impairs cerebellar-dependent motor learning
- Ataxia, gait instability, and balance problems may persist beyond acute intoxication
Combined Use: Special Considerations
- Cardiovascular synergy - cocaine's vasoconstrictive/hypertensive effects plus ketamine's catecholamine release (tachycardia, HTN) creates extreme hemodynamic stress, increasing stroke risk
- Dopamine + NMDA system dual disruption - cocaine depletes dopamine while ketamine disrupts NMDA-mediated glutamate signaling; this produces a complex, compounded neurochemical deficit state that is harder to recover from than either alone
- Additive cognitive impairment - frontal executive dysfunction from both agents converges
- Psychosis risk - cocaine-induced paranoid psychosis on the background of ketamine-induced NMDA hypofunction is a powerful recipe for persistent psychotic symptoms
- Depression severity - dopamine depletion (cocaine) compounded by glutamatergic dysregulation (ketamine) produces refractory post-withdrawal depression
Timeline of Recovery at 1 Month
| Sequela | Status at 1 Month | Trajectory |
|---|---|---|
| Post-stroke deficits | Active - in rehabilitation phase | Partial recovery possible (stroke recovery) |
| Cerebral atrophy | Fixed structural change | Does not reverse |
| WM microangiopathic changes | Fixed | Stable or slowly progressive |
| Cognitive impairment | Partially improving | Continues to improve for 6-12 months |
| Anhedonia / depression | Still prominent | Gradually resolves over months |
| Psychosis (ketamine-related) | May still be active | Weeks to months to resolve; may persist |
| Dissociative episodes | May still be occurring | Diminish over weeks |
| Seizure risk | Low (no drug present) | Depends on structural lesions |
| Dopamine receptor recovery | Incomplete (D2 upregulation ongoing) | 3-12 months for receptor normalization |
Clinical Bottom Line
- Cognitive impairment - neuropsychological testing recommended
- Persistent psychosis or mood disorder - psychiatric evaluation
- Structural brain lesions - MRI brain with FLAIR to evaluate for WM changes, prior infarcts, atrophy
- Epilepsy - EEG if there is any history of seizures
- Depression/anhedonia - closely monitored; antidepressant therapy may be warranted
explain the pharmacology and cocaine dependence syndrome as well as intoxication symptoms and withdrwal effects also explain the managmenet
cocaine use disorder treatment pharmacotherapy behavioral
PMID: 36401591
PMID: 34823736
Cocaine: Pharmacology, Dependence Syndrome, Intoxication, Withdrawal, and Management
PART 1 - PHARMACOLOGY
Sources and Formulations
- Cocaine hydrochloride (HCl) - water-soluble salt; a white crystalline powder inhaled intranasally ("snorted") or dissolved and injected IV
- Cocaine freebase / "crack" - heat-stable alkaloid that can be smoked; named for the cracking sound it makes when heated
| Route | Formula | Onset | Peak Effect | Duration |
|---|---|---|---|---|
| Inhalation (smoked) | Crack | 8-12 seconds | 2-5 min | 10-20 min |
| Intranasal (snorted) | HCl | 2-5 min | 5-10 min | 30 min |
| Intravenous | HCl | Seconds | 10-20 min | 60-90 min |
| Oral | HCl | 30-60 min | 60-90 min | Unknown |
- Half-life: ~90 minutes
- Metabolism: Plasma and hepatic cholinesterases → ecgonine methyl ester + benzoylecgonine (urine target in drug screens, detectable up to 7 days)
- Cocaethylene: When cocaine + ethanol are used together, cocaethylene forms - it has the same cocaine-like effects, explaining why alcohol prolongs and potentiates cocaine's actions rather than counteracting them - Rosen's Emergency Medicine
Mechanisms of Action (dual)
1. Monoamine Reuptake Blockade (primary CNS mechanism)
- Dopamine excess → euphoria, reward, increased salience of stimuli, locomotor activation
- Norepinephrine excess → vasoconstriction (alpha-1), tachycardia, hypertension, mydriasis, diaphoresis (sympathomimetic toxidrome)
- Serotonin excess → mood elevation, but also potential serotonergic excess with large doses
- In addition to blocking reuptake, cocaine has a weaker amphetamine-like action of releasing endogenous monoamines - Adams & Victor's Principles of Neurology
2. Sodium Channel Blockade (local anesthetic mechanism)
- Slows neuronal conduction (basis of topical anesthesia in ENT surgery)
- In the heart, prolongs the QRS (>100 ms = sign of significant Na-channel toxicity)
- Can also block K⁺ channels → QT prolongation
- Combined adrenergic stimulation + Na-channel blockade → ventricular tachyarrhythmias
The Reward Pathway (why cocaine is so addictive)
PART 2 - COCAINE DEPENDENCE SYNDROME
Dependence vs. Addiction
| Term | Definition |
|---|---|
| Dependence | Neuroadaptation producing withdrawal when drug is stopped; defined by a withdrawal syndrome |
| Addiction | Compulsive, relapsing use despite negative consequences; loss of control; cue-triggered craving |
DSM-5: Cocaine Use Disorder Criteria (11 criteria, 3+ = moderate/severe)
- Taking cocaine in larger amounts or over longer time than intended
- Persistent desire or unsuccessful efforts to cut down
- Spending a great deal of time obtaining, using, or recovering
- Craving - strong urge to use cocaine
- Failure to fulfill major role obligations (work, school, home)
- Continued use despite persistent social or interpersonal problems
- Giving up important activities because of cocaine use
- Recurrent use in physically hazardous situations
- Continued use despite knowledge of physical/psychological harm
- Tolerance - need for more to achieve effect, or diminished effect with same dose
- Withdrawal - characteristic syndrome upon stopping
Neurobiological Basis of Dependence
- Downregulation of D2 receptors - the brain reduces dopamine receptor density to compensate for the chronic dopamine flood
- DAT upregulation - more transporter molecules expressed to remove dopamine faster
- Reduced dopamine synthesis - presynaptic compensatory reduction
- Result: When cocaine is stopped, the now-dopamine-depleted brain with upregulated transporters and downregulated receptors cannot maintain normal dopamine tone → dysphoria, anhedonia, craving
PART 3 - INTOXICATION SYMPTOMS
Mild-Moderate Intoxication (desired and early toxic effects)
- Euphoria, sense of well-being, heightened confidence
- Increased energy and alertness
- Loquacity (talkativeness), sociability
- Reduced appetite, reduced need for sleep
- Heightened sensory perception
- Mild paranoia or anxiety (very common even at moderate doses)
- Tachycardia
- Hypertension
- Mydriasis (dilated pupils)
- Diaphoresis (sweating)
- Hyperthermia
- Increased motor tone
Severe Intoxication / Overdose
| System | Manifestation |
|---|---|
| CNS | Agitation, psychosis, paranoid delusions, hallucinations (tactile "cocaine bugs" / formication, visual, auditory) |
| Seizures | Generalized tonic-clonic; status epilepticus in severe cases |
| Cardiovascular | Severe hypertension, tachyarrhythmias (SVT, VT), chest pain (cocaine-induced coronary vasospasm + thrombosis) |
| Neurological | Tremor, myoclonus, hyperreflexia |
| Thermal | Life-threatening hyperthermia |
| Cerebrovascular | Ischemic stroke, hemorrhagic stroke, SAH |
| Metabolic | Rhabdomyolysis → acute renal failure, DIC, liver dysfunction |
| End-stage | Coma → death |
"Symptoms of severe intoxication (overdose) may lead to coma and death and require emergency treatment in an intensive care unit." - Adams & Victor's Principles of Neurology
Cocaine-Induced Paranoid Psychosis
PART 4 - WITHDRAWAL SYNDROME
Phases of Cocaine Withdrawal
- Immediately after stopping or after a binge ("crash")
- Profound dysphoria, depression, anxiety
- Extreme fatigue and hypersomnia (prolonged sleep)
- Increased appetite (rebound)
- Intense craving during the crash, then craving subsides temporarily
- Little psychomotor agitation
- Anhedonia - inability to feel pleasure from normally rewarding activities
- Persistent dysphoria and depression
- Insomnia (paradoxically, despite the initial hypersomnia)
- Restlessness, irritability
- Intense craving - especially triggered by cues (places, people, sounds associated with drug use)
- Anorexia
- Hyperprolactinemia (due to dopamine depletion - dopamine normally inhibits prolactin)
- Signs of dopaminergic hypersensitivity
- Low-level dysphoria and anhedonia persist
- Episodic craving triggered by cues and stress
- Risk of relapse is highest during this period
- Gradually subsides over months
"Abstinence from cocaine following a period of chronic abuse is regularly attended by insomnia, restlessness, anorexia, depression, hyperprolactinemia, and signs of dopaminergic hypersensitivity - a symptom complex that constitutes an identifiable withdrawal syndrome." - Adams & Victor's Principles of Neurology
Key Features Distinguishing Cocaine Withdrawal
- No life-threatening autonomic instability (unlike alcohol/benzodiazepine withdrawal)
- No physical seizures from withdrawal itself (seizures during cocaine use are from intoxication, not withdrawal)
- The dominant danger is depression and suicidality during the crash phase
- Cue-triggered craving is the primary driver of relapse for months-years
PART 5 - MANAGEMENT
A. Acute Intoxication Management
1. Agitation / CNS Excitation
- Benzodiazepines (first-line): Lorazepam or diazepam IV - treat agitation, lower BP, prevent/treat seizures simultaneously. Preferred over antipsychotics initially
- Antipsychotics: Haloperidol for cocaine-induced psychosis/paranoia - Adams & Victor; use with caution as they lower seizure threshold
2. Seizures
- Benzodiazepines (first-line): More effective than standard anticonvulsants for cocaine-related seizures - Adams & Victor's Principles of Neurology
- Phenytoin/fosphenytoin are less effective (cocaine seizures are not Na-channel mediated in the same way)
- Treat reversible causes (hyperthermia, hypoglycemia)
3. Hypertension
- Benzodiazepines often sufficient for mild-moderate hypertension (by reducing sympathetic drive)
- Phentolamine (alpha-blocker) for refractory hypertension
- Nitroprusside or nitroglycerin for hypertensive emergency
- AVOID beta-blockers (propranolol, metoprolol) - blocking beta receptors while alpha receptors remain stimulated causes paradoxical hypertension and coronary vasospasm
4. Hyperthermia
- Active cooling (ice packs, cooling blankets, cool IV fluids) - a medical emergency
- Benzodiazepines to stop muscle hyperactivity
- Dantrolene if severe (muscle relaxant)
5. Cardiac Arrhythmias / QRS Widening
- Sodium bicarbonate for QRS prolongation from Na-channel blockade (as with TCA overdose)
- Lidocaine is relatively contraindicated (also a Na-channel blocker)
6. Cocaine-Associated Chest Pain / ACS
- Benzodiazepines + aspirin + nitroglycerin + calcium channel blockers (CCBs)
- Avoid beta-blockers
7. Rhabdomyolysis
- Aggressive IV fluid resuscitation
- Monitor renal function, CK, urine output
B. Management of Cocaine Withdrawal
Supportive / Non-pharmacological
- Safe, low-stimulation environment
- Hydration, nutrition
- Close monitoring for suicidality (depression can be severe)
- Psychoeducation
Pharmacological (targeted at dopaminergic recovery)
| Drug | Mechanism | Evidence |
|---|---|---|
| Topiramate | Glutamate modulation, GABA enhancement | Mixed evidence for cocaine withdrawal (PMID: 36401591) |
| Bupropion | Dopamine/NE reuptake inhibitor; "substitution" strategy | Some benefit; also treats depression |
| Amantadine | Dopamine releaser / NMDA antagonist | Modestly reduces craving in some studies |
| Bromocriptine | D2 agonist - replaces depleted dopamine tone | Used for acute crash dysphoria; short-term |
| Antidepressants (desipramine, imipramine) | Restore dopaminergic/noradrenergic tone | Early studies showed promise; not firmly established |
| Mirtazapine | NaSSA; addresses insomnia and dysphoria | Potential efficacy in withdrawal (PMID: 36401591) |
| Naltrexone | Opioid antagonist; reduces reward | Mixed evidence; some benefit in withdrawal phase |
Important: Currently there is NO FDA-approved pharmacotherapy specifically for cocaine use disorder. Treatments remain off-label and evidence is inconsistent. - PMID 36401591 (Addiction, 2023)
C. Long-term Management of Cocaine Use Disorder
Psychosocial Treatments (most evidence-based)
- Cognitive Behavioral Therapy (CBT) - identifies triggers, builds coping strategies; well-validated
- Contingency Management (CM) - voucher-based incentives for drug-free urine screens; strongest behavioral evidence for cocaine dependence
- 12-Step facilitation (e.g., Narcotics Anonymous)
- Motivational Interviewing (MI)
- Community Reinforcement Approach (CRA)
Emerging Pharmacotherapy
- GLP-1 receptor agonists (semaglutide, liraglutide) - emerging evidence that GLP-1 analogues reduce reward-seeking and addiction behaviors across multiple substances including cocaine, via effects on dopamine circuitry - PMID 40508146 (2025) and PMID 34532853
- Cocaine vaccine (TA-CD) - immunotherapy generating anti-cocaine antibodies to prevent cocaine reaching the brain; in clinical trials
- Disulfiram - inhibits dopamine beta-hydroxylase; reduces cocaine use in some trials (especially co-occurring alcohol disorder)
Management Summary Diagram
COCAINE PROBLEM
|
├── ACUTE INTOXICATION
│ ├── Benzodiazepines (agitation, seizures, HTN)
│ ├── Antipsychotics (psychosis)
│ ├── Active cooling (hyperthermia)
│ ├── NaHCO₃ (QRS widening)
│ └── AVOID beta-blockers
│
├── WITHDRAWAL (crash + protracted)
│ ├── Supportive care + monitoring for suicidality
│ ├── Bupropion / mirtazapine / topiramate (off-label)
│ └── Bromocriptine for acute crash
│
└── DEPENDENCE (long-term)
├── Contingency Management (strongest evidence)
├── CBT / Motivational Interviewing
├── 12-Step programs
└── Emerging: GLP-1 agonists, disulfiram, vaccine
Explain the dopamine hypothesis of addiction and reward pathway neurobiology
The Dopamine Hypothesis of Addiction and Reward Pathway Neurobiology
PART 1 - THE REWARD PATHWAY: ANATOMY AND NEUROBIOLOGY
The Mesolimbic Dopamine System
Key Anatomical Nodes
| Structure | Role |
|---|---|
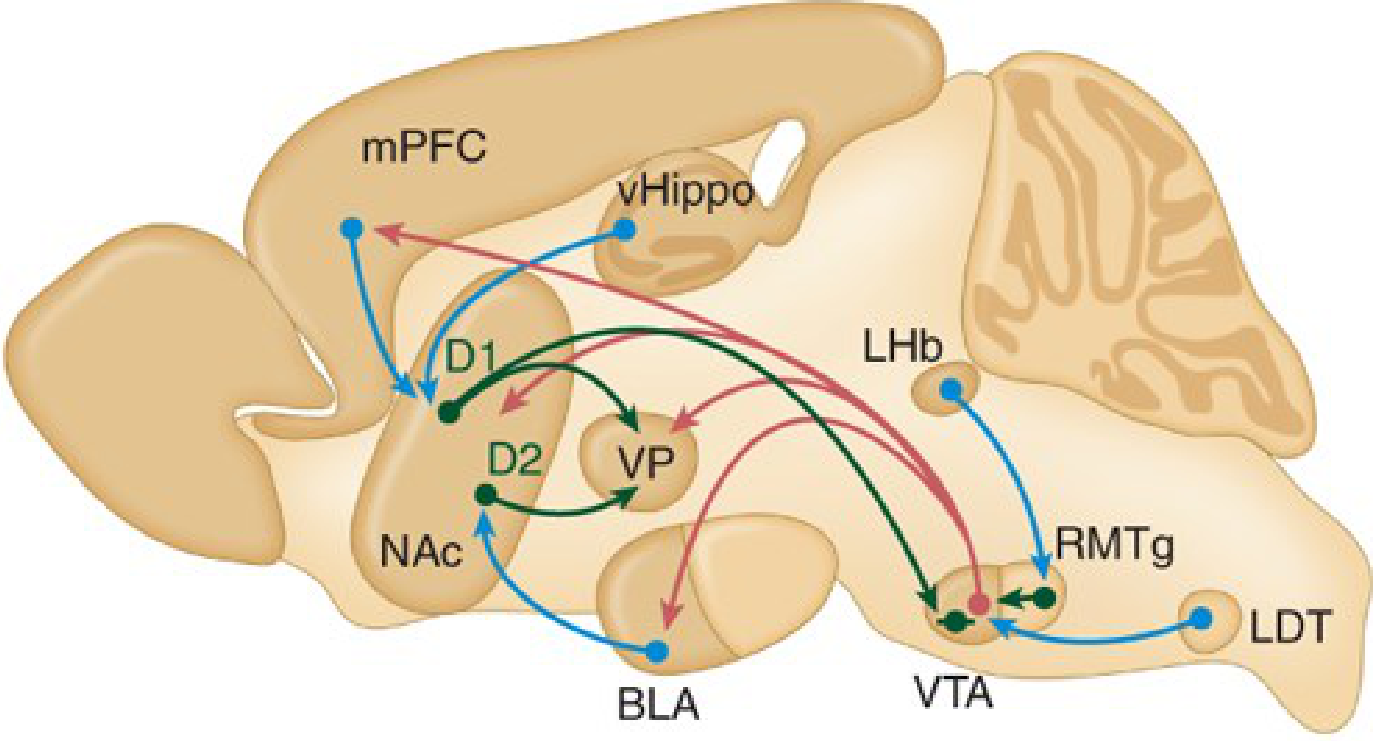
| Ventral Tegmental Area (VTA) | Origin of dopamine neurons; the "engine" of the reward circuit; located at the tip of the brainstem |
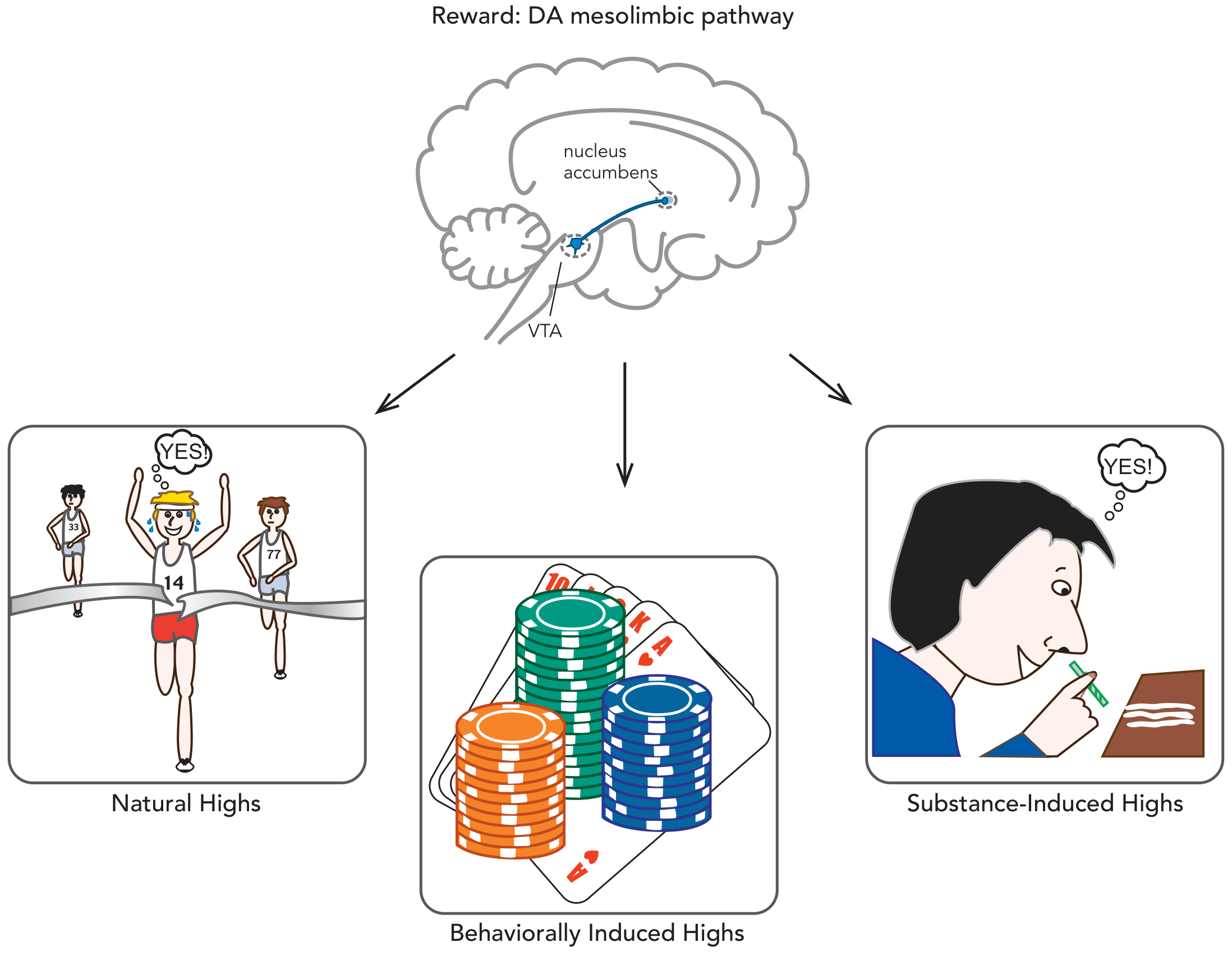
| Nucleus Accumbens (NAc) | Primary target; "reward hub"; receives DA from VTA; mediates pleasure, motivation, and reinforcement |
| Medial Prefrontal Cortex (mPFC) | Receives DA from VTA; involved in decision-making, impulse control, evaluating consequences |
| Basolateral Amygdala (BLA) | Emotional memory of rewarding/aversive events; drives cue-triggered craving |
| Ventral Hippocampus (vHippo) | Contextual memory; encodes "where and when" the drug experience occurred |
| Ventral Pallidum (VP) | Downstream output; connects reward circuit to motor systems |
| Orbitofrontal Cortex (OFC) | Value-coding; projects to dorsal striatum - implicated in compulsive drug-seeking |
D1 vs. D2 Receptor Neurons in the Nucleus Accumbens
- D1-receptor expressing neurons - form the "direct pathway" → project to VP and VTA → promote reward and drug-seeking
- D2-receptor expressing neurons - form the "indirect pathway" → project selectively to VP → inhibit reward and suppress drug-seeking
Neurotransmitter Inputs That Modulate the VTA
- Endorphins (brain's own morphine/heroin) - activate mu-opioid receptors on GABAergic interneurons in VTA, disinhibiting DA neurons
- Endocannabinoids/anandamide (brain's own cannabis) - suppress inhibitory GABA tone on DA neurons
- Acetylcholine (brain's own nicotine) - via LDT/PPT cholinergic inputs excite VTA DA neurons
- Dopamine itself (brain's own cocaine/amphetamine) - provides natural reward signal
- Serotonin (from raphe nuclei) - modulates VTA activity
- Glutamate (from mPFC, hippocampus, amygdala) - excitatory inputs to both VTA and NAc
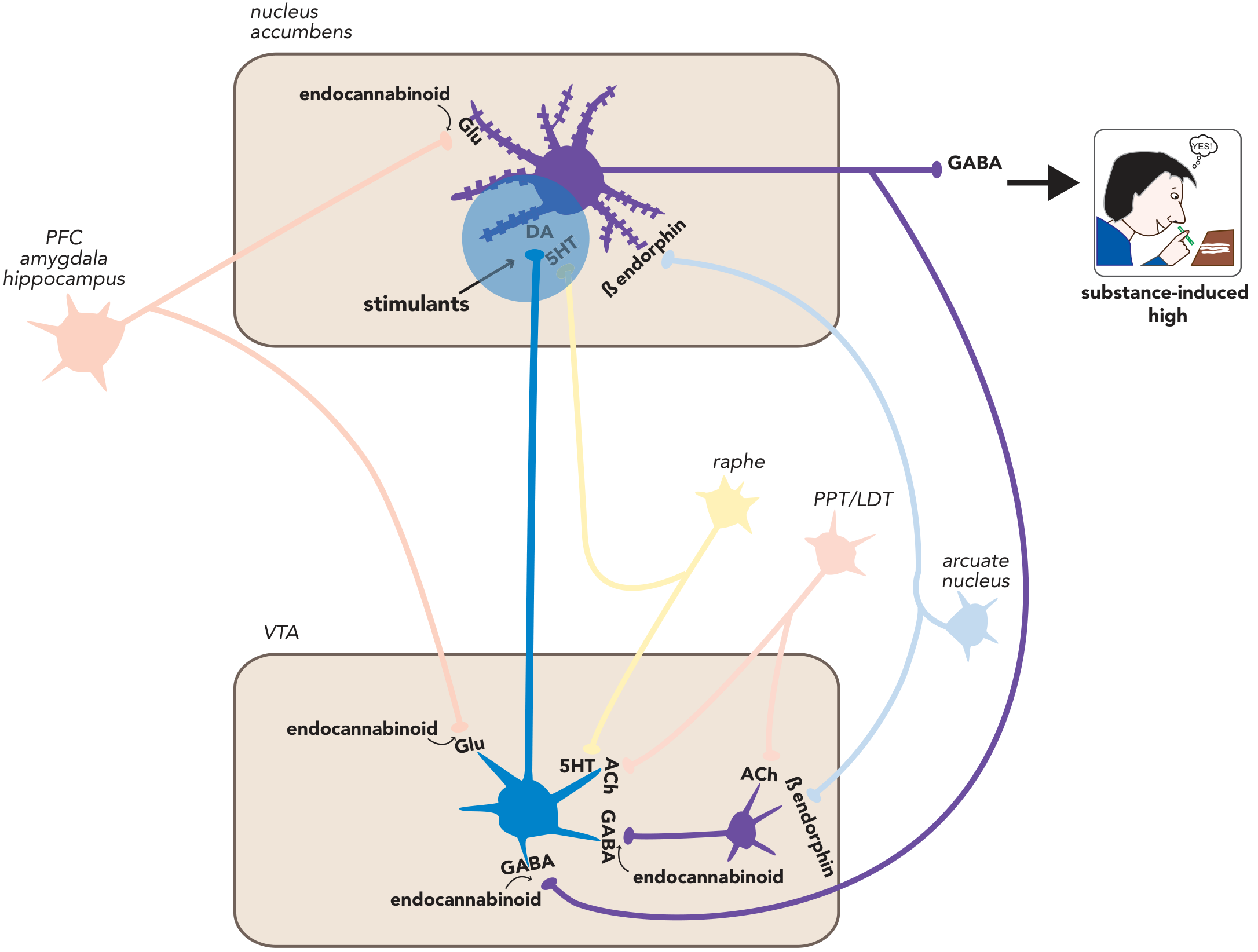
"The inputs to the mesolimbic pathway that mediate natural highs include a most incredible pharmacy of naturally occurring substances - the brain's own morphine/heroin (endorphins), the brain's own marijuana (anandamide), the brain's own nicotine (acetylcholine), the brain's own cocaine and amphetamine (dopamine itself)." - Stahl's Essential Psychopharmacology
PART 2 - THE DOPAMINE HYPOTHESIS OF ADDICTION
Original (Classical) Version
- Natural rewards (food, sex, achievement) cause modest, earned dopamine release in NAc
- Drugs of abuse cause explosive, pharmacologically hijacked dopamine release - far exceeding any natural reward in both magnitude and speed
Refined Version: Dopamine as "Prediction Error" Signal
- Unexpected reward delivered → DA neurons fire robustly ("positive prediction error")
- Reward predicted by a cue, then delivered as expected → DA neurons fire at the cue, not the reward itself (the reward is "already predicted" so no error)
- Reward predicted but not delivered → DA neurons go silent at the moment the reward was expected ("negative prediction error" = disappointment)
"The mesolimbic system continuously scans the reward situation. It increases its activity when reward is larger than expected and shuts down when a promised reward is omitted, thus coding for the prediction error of reward." - Katzung's Basic & Clinical Pharmacology
How Drugs Hijack This System
- More explosive than any natural reward
- Occurs on demand (bypasses the "earning" process)
- Not subject to habituation in the same way as natural rewards
PART 3 - THE THREE CLASSES OF DRUG ACTION ON THE REWARD CIRCUIT
| Class | Drug Examples | Mechanism |
|---|---|---|
| Direct DA neuron stimulation | Nicotine | Binds excitatory nicotinic ACh receptors on VTA DA cell bodies → directly fires DA neurons |
| Reuptake blockade / release promotion | Cocaine (reuptake block), Amphetamine (release + reuptake block) | Block DAT → dopamine floods the synapse; amphetamine also reverses DAT to forcibly eject DA |
| Disinhibition (GABA interneuron suppression) | Opioids, Cannabis, Alcohol | Suppress inhibitory GABA interneurons in VTA → removes brake from DA neurons → DA release |
"Antidepressants that block serotonin and norepinephrine uptake, but not dopamine uptake, do not cause addiction even after prolonged use." - Katzung - this is critical evidence that DAT blockade specifically is the key to addiction, not just monoamine reuptake inhibition in general.
PART 4 - SPEED OF DRUG ENTRY AND REINFORCEMENT
| Route | Speed to Brain | Reinforcing Potential |
|---|---|---|
| Intravenous / Smoked | Seconds (bypasses GI, hits brain like intra-arterial bolus) | Maximum |
| Intranasal (snorted) | Minutes | High |
| Oral | 30-60 minutes (GI absorption, first-pass metabolism) | Lower |
"The speed with which a stimulant enters the brain dictates the degree of the subjective high. The most rapid and robust way to deliver drugs to the brain is to smoke those compatible with this route...akin to giving the drug by intra-arterial bolus via immediate absorption across the massive lung surface area." - Stahl's Essential Psychopharmacology
PART 5 - NEUROADAPTATION AND THE PROGRESSION TO ADDICTION
The Critical Shift: Phasic vs. Tonic Dopamine
- Phasic dopamine firing (burst firing): brief, large amplitude spikes of DA release - the "reward signal" - associated with pleasure and reinforcement
- Tonic dopamine firing (background): steady low-level release - associated with baseline motivation and motor tone
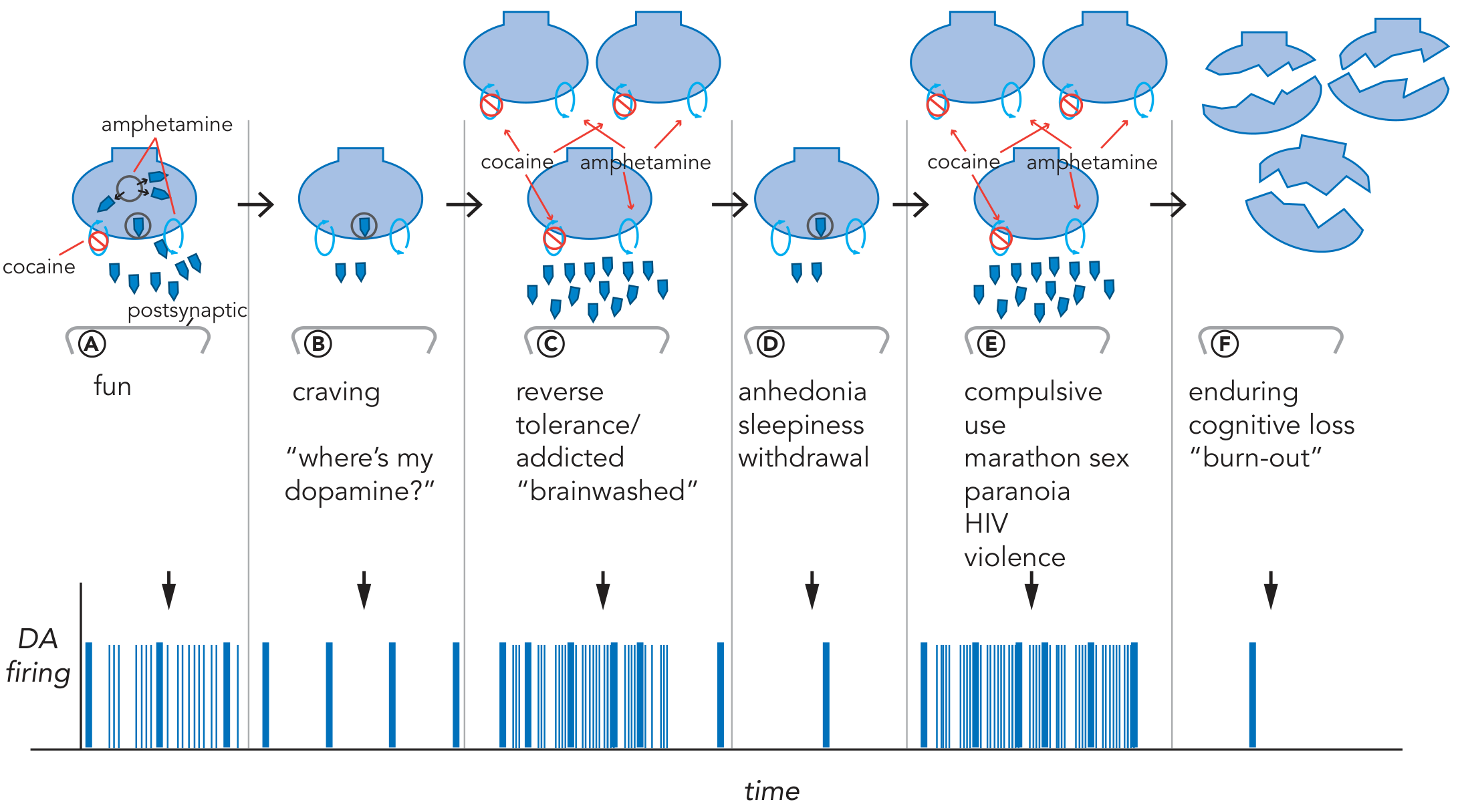
The Six Stages of Progression
PART 6 - MOLECULAR AND SYNAPTIC NEUROADAPTATION
D2 Receptor Downregulation (Tolerance)
- The brain compensates for chronic dopamine excess by reducing D2 receptor density
- With fewer receptors, the same amount of dopamine produces less effect → tolerance
- PET imaging in cocaine addicts shows dramatically reduced D2 receptor binding in striatum compared to controls
- This D2 hypofunction persists for months after stopping the drug - explaining protracted anhedonia
DAT Upregulation
- The brain also increases the number of dopamine transporter (DAT) molecules to clear dopamine faster
- When the drug is removed: upregulated DAT rapidly clears whatever dopamine is made → dopamine depletion state
CREB and ΔFosB (Transcription Factor Changes)
- CREB (cAMP Response Element Binding Protein) - activated acutely; reduces cocaine reward and contributes to tolerance; reverses quickly with abstinence
- ΔFosB - accumulates with repeated drug use; extremely long-lasting; promotes compulsive drug-seeking even after abstinence; changes the expression of proteins involved in synaptic strength
Glutamate and Synaptic Plasticity
- Glutamatergic projections from mPFC and hippocampus to NAc are modified during addiction
- During drug use: glutamate surges in NAc alongside dopamine
- During abstinence/withdrawal: glutamate levels in NAc drop, triggering upregulation of AMPA receptors
- When re-exposed to drug or cues, the sensitized glutamate system drives intense craving and relapse
- This is why glutamate modulators (e.g., N-acetylcysteine, topiramate) are being explored as addiction treatments
PART 7 - THE IMPULSIVITY-TO-COMPULSIVITY TRANSITION
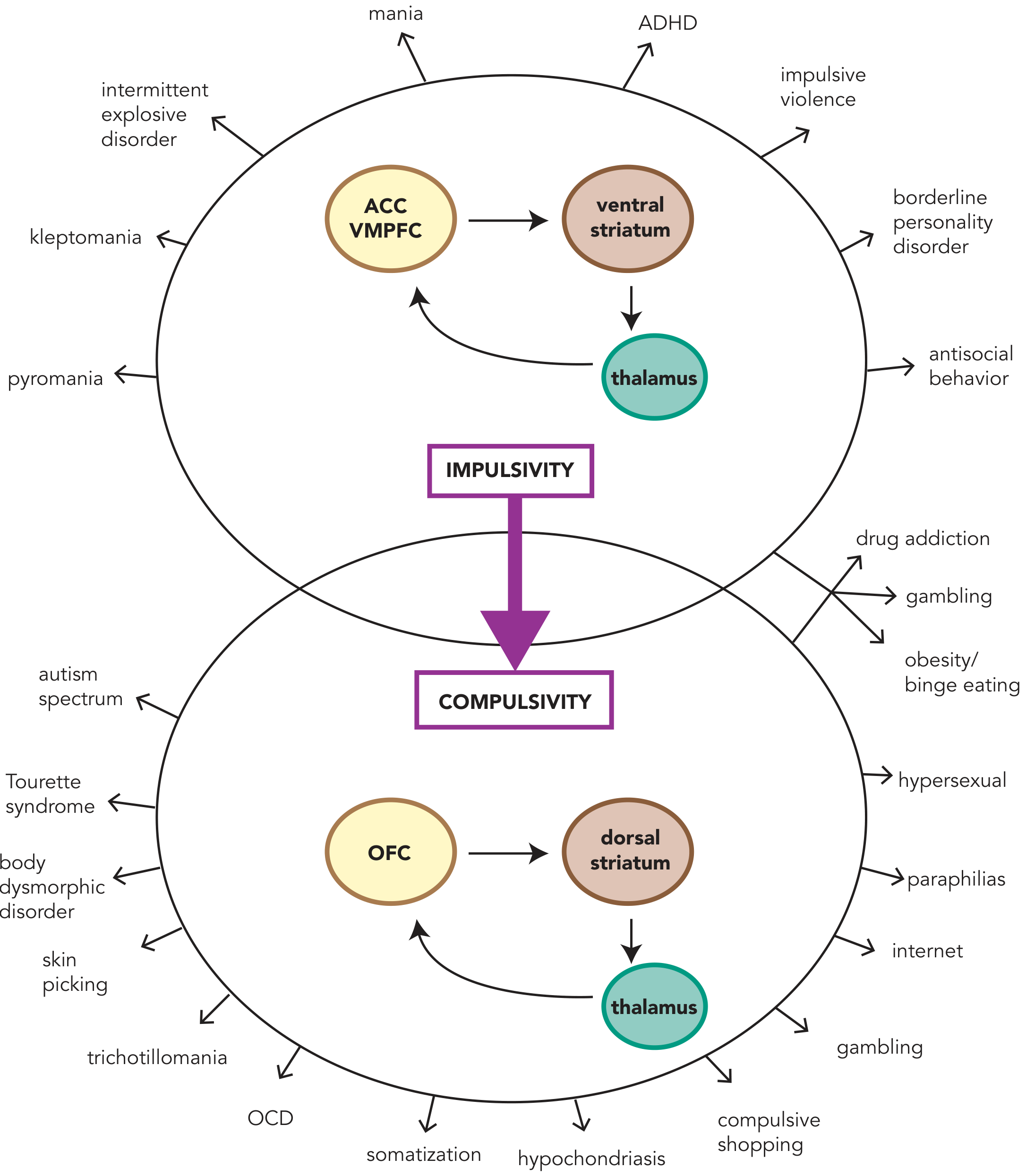
- Impulsive phase: Drug use is governed by the ventral striatum (reward) and the ACC/VMPFC (emotional decision-making). At this stage, the person could theoretically choose to stop.
- Compulsive phase: Through neuroplastic changes, control shifts to the dorsal striatum (habit circuit) and OFC (value/compulsive drive). Drug-seeking becomes an automatic habit - as reflexive as brushing your teeth.
"What starts out as fun and increased dopamine release in the ventral striatum ends up with the locus of control in the habit circuit as a mindless, automatic, and powerful compulsive drive to obtain drugs that is basically irresistible." - Stahl's Essential Psychopharmacology
PART 8 - RELAPSE: THE ROLE OF CUE-CONDITIONING AND NEGATIVE REINFORCEMENT
Positive Reinforcement (early addiction)
Negative Reinforcement (late addiction)
- Dynorphin and κ-opioid receptor (KOR) activation - produce dysphoria during withdrawal
- Corticotropin-releasing factor (CRF) hyperactivation - drives stress-induced craving
Cue-Triggered Relapse
- Drug-associated cues (places, people, objects, smells)
- Stress (activates CRF and corticosteroid pathways that engage the reward circuit)
- Re-exposure to a small dose of the drug ("priming")
"More than 85% of people with addictions who stop using a drug reinstate drug use within a year. This is not due to physical symptoms, but to emotional craving." - Goodman & Gilman's Pharmacological Basis of Therapeutics
PART 9 - LIMITATIONS OF THE DOPAMINE HYPOTHESIS
- Not all addictive drugs produce equal DA effects - marijuana and opioids have weaker/indirect effects on DA compared to cocaine/amphetamine
- DAT-knockout mice still self-administer cocaine (until both NET and SERT are also removed) - showing that serotonin and norepinephrine transporters can substitute
- Dopamine neurons also respond to aversive stimuli - a subpopulation of VTA neurons projecting to mPFC/tail of striatum fire to aversive events, not just rewards
- Serotonin, GABA, glutamate, opioids, and endocannabinoids all contribute independently to reinforcement
- Social, genetic, and environmental factors determine who becomes addicted - most people who try cocaine do NOT become addicted
Summary: From Reward to Addiction - The Core Sequence
NATURAL REWARD
→ Modest phasic DA release (VTA → NAc)
→ Reinforcement learning (prediction error)
→ Normal motivated behavior
DRUG EXPOSURE (first use)
→ Explosive phasic DA release (much greater than natural)
→ Massive artificial prediction error: "DO THIS ALWAYS"
→ Strong reinforcement of drug-seeking behavior
REPEATED DRUG USE
→ D2 downregulation + DAT upregulation (tolerance)
→ CREB activation (tolerance, reduced reward)
→ ΔFosB accumulation (long-lasting compulsive drive)
→ Glutamate plasticity in NAc (sensitization)
ADDICTION (established)
→ Control shifts from ventral (voluntary) → dorsal striatum (habit/compulsion)
→ OFC drives compulsive seeking despite consequences
→ Cue-conditioned DA release → craving even in abstinence
→ Negative reinforcement: drug taken to escape withdrawal dysphoria
BURN-OUT (chronic)
→ Depleted dopamine stores, axonal degeneration
→ Persistent anhedonia, cognitive deficits
→ Natural rewards no longer activate the system