Post dated pregnancy in ms level
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Now I have comprehensive content. Let me compile the full answer.
Post-Dated (Postterm) Pregnancy
Definition & Terminology
- Postterm pregnancy: Pregnancy continuing beyond 42 weeks (294 days) of gestation
- "Post-dates" is a misleading/imprecise term — some interpret it as simply going past the EDC (40 weeks); "postterm" is the preferred nomenclature
- "Late-term" = 41 0/7 to 41 6/7 weeks
- Incidence: ~7–12% of pregnancies
Dating of Pregnancy
- Nägele's Rule: Subtract 3 months from LMP + add 7 days = EDC
- EDC should ideally be confirmed by ultrasound before 22 weeks
- ≤ 12 weeks: margin of error ± 7 days
- 12–20 weeks: ± 14 days
- Most postterm pregnancies are due to inaccurate EDC calculation
Risk Factors
| Risk Factor |
|---|
| Primiparity |
| Fetal anencephaly |
| Male fetus |
| Personal or family history of postterm pregnancy |
| Maternal age > 30 years |
| Obesity |
| Placental sulfatase deficiency |
Complications
Maternal Complications
- Labor dystocia
- 3rd and 4th degree perineal lacerations
- Postpartum hemorrhage
- Maternal infection (intra-amniotic infection, endometritis)
- Increased risk of cesarean section
Fetal/Neonatal Complications
- Macrosomia (large for gestational age)
- Intrauterine fetal demise (risk increases as pregnancy progresses)
- Meconium aspiration syndrome
- Decreased 5-minute Apgar score (< 4)
- Neonatal convulsions
- Note: Umbilical cord prolapse is NOT increased; amniotic fluid volume actually decreases
Dysmaturity Syndrome (Clifford Syndrome)
- Affects 10–20% of postterm pregnancies
- Cause: uteroplacental insufficiency (chronic intrauterine malnutrition)
- Infant features: meconium stained, small for gestational age, peeling (desquamating) skin
- Neonatal risks: respiratory distress from meconium aspiration, hypoglycemia, neonatal seizures, cerebral palsy
Antepartum Surveillance
- Begin at 41 weeks
- Twice-weekly NST, BPP, or both
Biophysical Profile (BPP) — 5 Elements (each scored 0 or 2; total = 10)
| Element | Normal Criterion |
|---|---|
| Non-stress test (NST) | Reactive |
| Fetal breathing movement | Rhythmic, ≥ 30 seconds in 30 min |
| Fetal movement | ≥ 3 discrete movements in 30 min |
| Fetal tone | ≥ 1 episode of extension + flexion |
| Amniotic fluid index (AFI) | ≥ 5 cm or single pocket ≥ 2 cm |
- BPP 8–10 = Normal | 6 = Equivocal | 0–4 = Abnormal
- Modified BPP = NST + AFI (acceptable alternative)
Reactive NST Criteria
- ≥ 32 weeks: 2 accelerations of ≥ 15 bpm lasting ≥ 15 sec in a 20-min window
- < 32 weeks: 2 accelerations of ≥ 10 bpm lasting ≥ 10 sec
Management / Induction of Labor
- Induction can begin electively at 41 weeks or as surveillance dictates
- ACOG recommends induction before 42 6/7 weeks' gestation
- Use Bishop score (< 6 per AAFP; < 8 per ACOG) to determine need for cervical ripening
Bishop Score
| Parameter | Score 0 | Score 1 | Score 2 | Score 3 |
|---|---|---|---|---|
| Dilation (cm) | Closed | 1–2 | 3–4 | ≥5 |
| Effacement (%) | 0–30 | 40–50 | 60–70 | ≥80 |
| Station | −3 | −2 | −1, 0 | +1 |
| Consistency | Firm | Medium | Soft | — |
| Position | Posterior | Mid | Anterior | — |
Cervical Ripening Methods
Mechanical:
- Intrauterine Foley catheter
- Cook double balloon
- Osmotic dilators (laminaria)
Pharmacological (Prostaglandins):
- Vaginal misoprostol (Cytotec) 25 mcg q4h
- Dinoprostone (Cervidil) 10 mg insert × 12h; or Prepidil gel 0.5 mg q6h × 3 doses
(Note: Nipple stimulation may produce contractions but is NOT a recommended ripening option)
Sources: Swanson's Family Medicine Review, pp. 510–511 | Creasy & Resnik's Maternal-Fetal Medicine
Dystosia
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Now I have comprehensive information to compile a thorough answer on dystocia.
Dystocia (Abnormal Labor)
Definition
Dystocia = any abnormality in the progression or duration of labor (abnormal labor).
- Accounts for 1/3 of all cesarean sections and 1/2 of primary cesarean sections
- The term "failure to progress" is vague and should NOT be used — use specific terminology instead
The 3 P's — Causes of Dystocia
| Category | Factor | Examples |
|---|---|---|
| Power | Uterine contractions / expulsive force | Inadequate contractions (< 200 Montevideo units), maternal exhaustion |
| Passageway | Bony pelvis / soft tissue | Non-gynecoid pelvic shape, prominent ischial spines, abnormal pubic arch, obstructive sacral promontory |
| Passenger | Fetus | Macrosomia, malpresentation, malposition (e.g., occiput posterior) |
Dystocia is usually caused by a combination of these factors.
Stages of Labor — Normal Limits
| Stage | Definition | Upper Limit of Normal |
|---|---|---|
| 1st stage – Latent phase | 0 to 5 cm dilation | Prolonged if > 20 hrs (nulliparous) / > 14 hrs (multiparous) |
| 1st stage – Active phase | 6 to 10 cm dilation | Nulliparous: 0.5–0.7 cm/hr; Multiparous: 0.5–1.3 cm/hr |
| 2nd stage | Complete dilation → delivery of infant | 3 hrs (nulliparous) / 2 hrs (multiparous) |
| 3rd stage | Delivery of infant → delivery of placenta | > 30 min = prolonged |
Types of Labor Arrest
1. Arrest of Dilation (First-Stage Arrest)
- No cervical change despite:
- 4 hours of adequate contractions (≥ 200 Montevideo units/10 min by IUPC), OR
- 6 hours of oxytocin augmentation with inadequate uterine activity + no cervical change
- Most common indication for primary cesarean section in the US
- Allowing 4 hours of arrest (rather than 2 hrs) before resorting to cesarean results in successful vaginal delivery in most women with no adverse neonatal effect
2. Arrest of Descent (Second-Stage Arrest)
- No descent after adequate pushing beyond the time limits above
- Longer durations may be considered if progress is documented and maternal/fetal status is reassuring
Key Diagnostic Tool: Montevideo Units (MVUs)
- Measured by intrauterine pressure catheter (IUPC)
- External tocometer measures only frequency, not amplitude
- ≥ 200 MVUs in 10 minutes = adequate contractions → increased oxytocin is of no benefit
- < 200 MVUs = augment with oxytocin
Management of Labor Dystocia
- Oxytocin augmentation — mainstay for inadequate uterine activity
- IUPC placement — to accurately measure contraction strength
- Ambulation — often encouraged but NOT shown to resolve active-phase arrest
- Operative vaginal delivery (forceps/vacuum) — option only in 2nd stage
- Cesarean section — for confirmed arrest unresponsive to augmentation
Malpresentations — Incidence
| Malpresentation | Incidence |
|---|---|
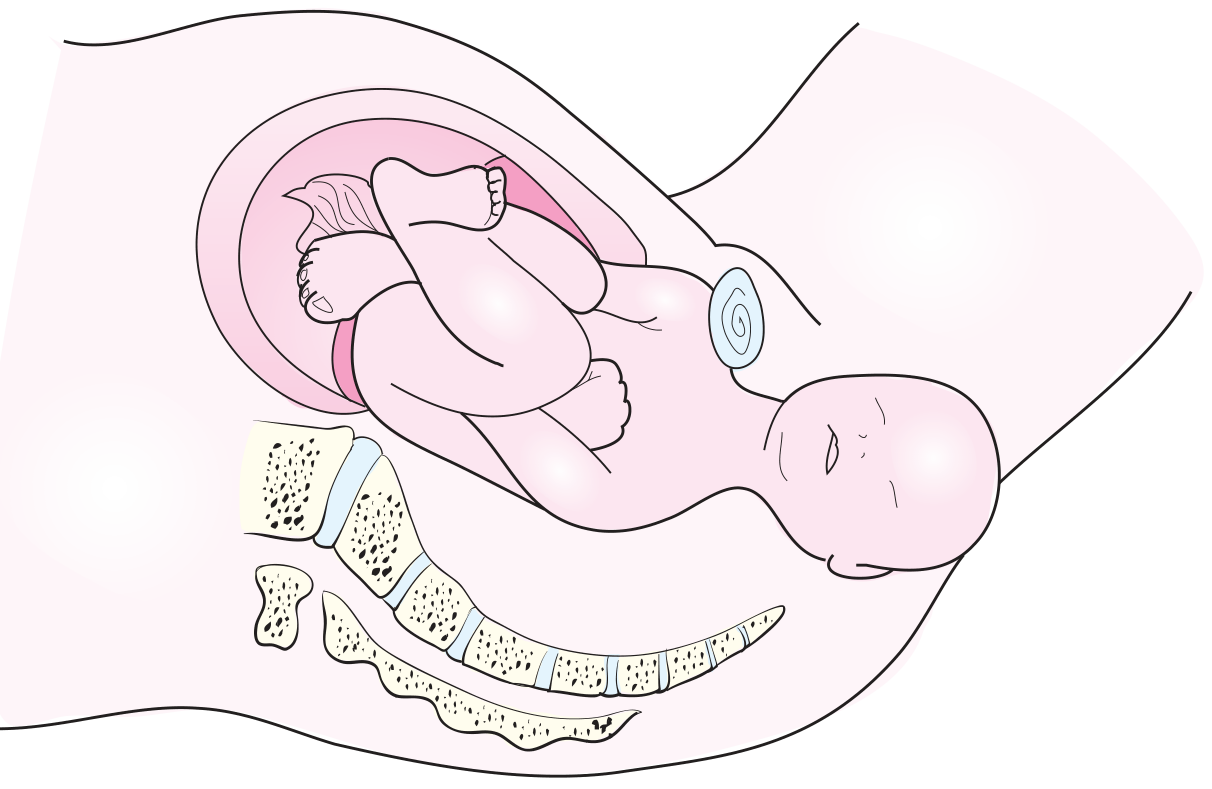
| Breech | 1 in 25 live births |
| Shoulder dystocia | 1 in 300 live births |
| Face presentation | 1 in 550 live births |
| Brow presentation | 1 in 1400 live births |
Shoulder Dystocia
Definition: Impaction of the anterior shoulder against the pubic symphysis after delivery of the head — occurs when shoulder breadth > biparietal diameter.
Incidence
- Overall: 0.3–1%
- With macrosomia (birth weight > 4500 g): 5–7%
- ~50% occur with normal-weight fetuses and are unanticipated
Risk Factors
- Macrosomia / maternal diabetes
- Maternal obesity / prepregnancy weight > 180 lb
- Excessive weight gain
- Advanced maternal age
- Postterm pregnancy
- Prior shoulder dystocia
- Contracted pelvis
- Prolonged 2nd stage / operative vaginal delivery
Warning Signs
- Prolonged 2nd stage
- Use of vacuum or forceps
Complications
Maternal: 4th-degree lacerations, postpartum hemorrhage, uterine rupture (rare)
Fetal:
- Brachial plexus injury — most common
- Erb's palsy (C5–C6) — most common
- Klumpke's palsy (C8–T1)
- Clavicular fracture
- Fetal hypoxia → neurological damage, death
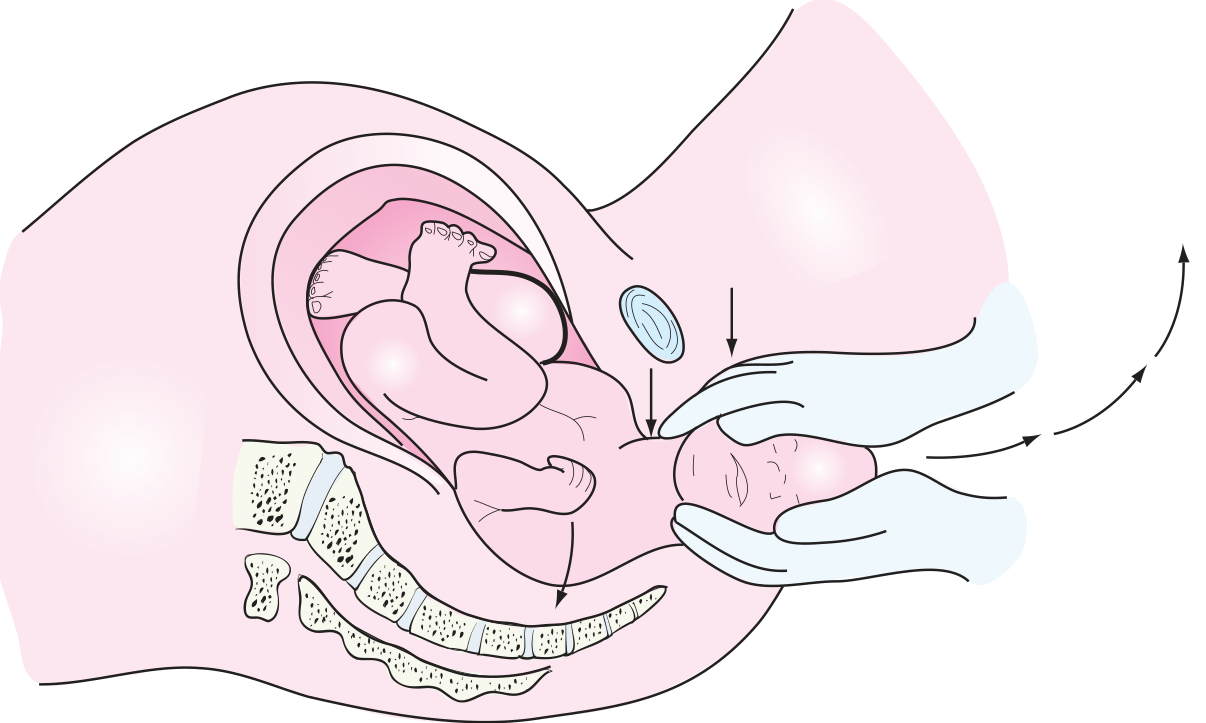
Management — HELPERR Mnemonic
| Step | Maneuver |
|---|---|
| H | Call for Help |
| E | Episiotomy (if needed for access) |
| L | Legs — McRoberts maneuver (hyperflex maternal thighs onto abdomen → increases inlet diameter, flattens lumbosacral lordosis) |
| P | Suprapubic pressure (dislodge anterior shoulder — NOT fundal pressure, which worsens impaction) |
| E | Enter — internal rotational maneuvers |
| R | Remove the posterior arm |
| R | Roll the patient (Gaskin all-fours maneuver) |
McRoberts maneuver + suprapubic pressure = first-line and most effective combination.
⚠️ Fundal pressure is contraindicated — it worsens shoulder impaction.
Sources: Swanson's Family Medicine Review, pp. 514–516 | Textbook of Family Medicine 9e, p. 507 | Rosen's Emergency Medicine, p. 3415 | Miller's Anesthesia 10e, p. 8827–8829
Tell me from obs gynae book in ms level
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.