Explain ecg abnormality
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough explanation of ECG abnormalities, drawn primarily from Harrison's Principles of Internal Medicine (22nd ed., 2025).
ECG Abnormalities - A Systematic Overview
The ECG records the heart's electrical activity across time. Abnormalities are classified into six major categories.
1. Cardiac Enlargement and Hypertrophy
Atrial Abnormalities
- Right atrial overload: Tall, peaked P waves (≥2.5 mm), historically called "P-pulmonale"
- Left atrial overload: Biphasic P wave in V1 with a broad negative component, OR a broad (≥120 ms), often notched P wave in limb leads ("P-mitrale"). This can also occur with interatrial conduction delays even without true enlargement.
Ventricular Hypertrophy

- Left ventricular hypertrophy (LVH): Increased QRS amplitude directed leftward and posteriorly; ST-segment depression and T-wave inversions in leads with prominent R waves (strain pattern). Common voltage criteria: S in V1 + R in V5/V6 >35 mm.
- Right ventricular hypertrophy (RVH): Rightward QRS axis; tall R in V1 (R, RS, or qR complex); T-wave inversions in right precordial leads. Associated with pulmonary hypertension, pulmonic stenosis.
2. Bundle Branch Blocks and Intraventricular Conduction Defects
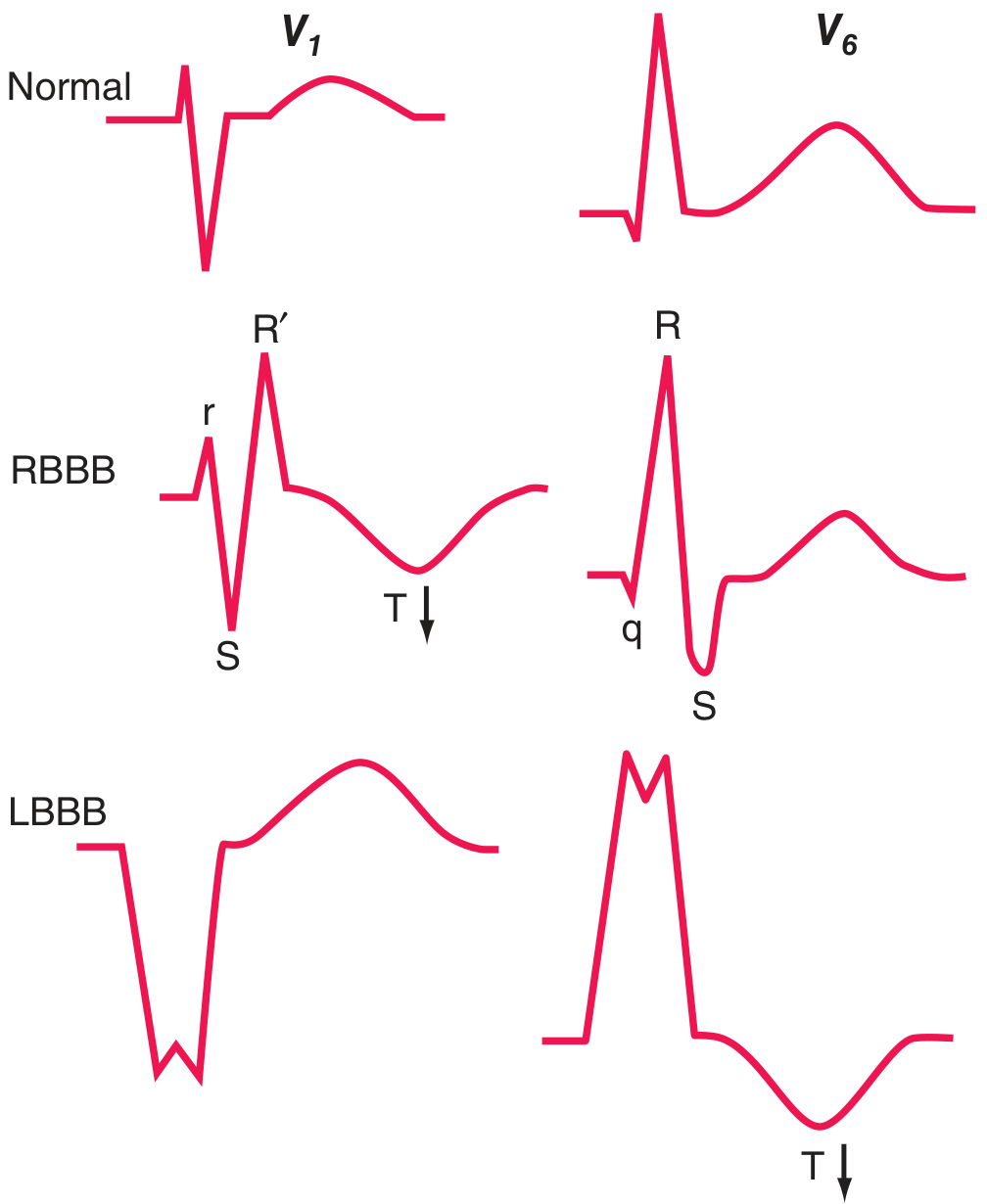
Complete bundle branch blocks have QRS duration ≥120 ms; incomplete blocks are 110-120 ms.
| Feature | RBBB | LBBB |
|---|---|---|
| V1 pattern | rSR' ("rabbit ears") | Wide QS (broad negative) |
| V6 pattern | qRS (deep S wave) | Entirely positive R (no Q, no S) |
| T wave | Inverted in V1-V3 (secondary change) | Inverted in V5-V6 (secondary change) |
| Clinical associations | ASD, pulmonary embolism, normal variant | Coronary artery disease, hypertension, aortic valve disease, cardiomyopathy |
Fascicular blocks (hemiblocks) do not widen the QRS but shift the axis:
- Left anterior fascicular block: axis more negative than -45° (marked left axis deviation) - most common cause of marked left axis deviation in adults
- Left posterior fascicular block: axis more rightward than +110-120° (rare as isolated finding)
Bifascicular block (RBBB + left anterior or posterior fascicular block) carries ~6% annual risk of progression to complete heart block.
Wolff-Parkinson-White (WPW): Wide QRS due to pre-excitation via an accessory bypass tract, NOT a conduction delay. Shows a delta wave (slurred QRS upstroke) and short PR interval.
3. Myocardial Ischemia and Infarction
Ischemia creates "currents of injury" that manifest as ST-segment deviation:
ST-Segment Elevation MI (STEMI)
- Transmural ischemia shifts the ST vector toward the epicardium → ST elevation in overlying leads
- Earliest sign: tall, peaked "hyperacute" T waves
- Evolution over hours to days: ST elevation → T-wave inversions → Q waves
Localization by leads:
| Territory | Leads with changes | Artery |
|---|---|---|
| Anterior/Apical | V1-V6, I, aVL | LAD |
| Inferior | II, III, aVF | RCA or LCX |
| Posterior | Reciprocal ST depression V1-V3 | LCX or RCA |
| Right ventricular | Right-sided leads (V3R, V4R) | RCA |
Non-ST Elevation / Subendocardial Ischemia
- Subendocardial ischemia shifts the ST vector toward the ventricular cavity → ST depression in precordial leads + ST elevation in aVR
- T-wave inversions without ST elevation
Pathological Q Waves
- Width ≥40 ms or depth ≥25% of R-wave height indicates prior transmural infarction
- Exception: septal Q waves in V5-V6 are normal (small, narrow)
4. Arrhythmias and Conduction (Rate/Rhythm Abnormalities)
By Heart Rate
- Tachycardia (>100 bpm): Sinus tachycardia, SVT, atrial flutter/fibrillation, ventricular tachycardia, ventricular fibrillation
- Bradycardia (<60 bpm): Sinus bradycardia, sick sinus syndrome, junctional rhythm
AV Conduction Blocks
| Degree | PR Interval | QRS | Notes |
|---|---|---|---|
| 1st degree | >200 ms (prolonged) | Normal | Benign |
| 2nd degree - Mobitz I (Wenckebach) | Progressive lengthening → dropped beat | Normal | Usually at AV node; relatively benign |
| 2nd degree - Mobitz II | Fixed PR, sudden dropped QRS | Normal or wide | Below the AV node; higher risk |
| 3rd degree (complete) | No relationship between P and QRS | Escape rhythm (wide or narrow) | Full AV dissociation |
Atrial Fibrillation
- Absent P waves, irregularly irregular rhythm, fibrillatory baseline
- Narrow QRS unless aberrant conduction
Ventricular Tachycardia
- Wide QRS (>120 ms), rate >100 bpm, AV dissociation
- Fusion beats and capture beats are diagnostic
5. Metabolic and Drug-Induced Changes
| Cause | ECG Change |
|---|---|
| Hyperkalemia | Peaked (tented) T waves → widening QRS → loss of P waves → sine-wave → asystole |
| Hypokalemia | Flattened T waves, prominent U waves, prolonged QU interval |
| Hypercalcemia | Shortened QT interval |
| Hypocalcemia | Prolonged QT interval (ST portion lengthened) |
| Hypothermia | Osborn (J) waves, bradycardia, prolonged QT |
| Digoxin | "Scooped" ST-T depression, shortened QT, AV block at toxic levels |
| Class IA/III antiarrhythmics | Prolonged QT → risk of torsades de pointes |
| Intracranial hemorrhage | Deep, wide T-wave inversions ("CVA T waves"), especially with SAH |
6. Other Notable Abnormalities
Brugada Pattern
- Right bundle branch block morphology + ST elevation in V1-V3 (coved or saddleback type)
- Associated with sudden cardiac death risk; inherited channelopathy
QT Prolongation
- QTc >440 ms in men, >460 ms in women (Bazett formula)
- Risk of torsades de pointes and sudden death
- Causes: congenital LQTS, drugs, electrolyte disturbances, hypothermia
Pericarditis
- Diffuse ST elevation (concave/"saddle-shaped") in multiple leads + PR depression
- No reciprocal changes (unlike MI), no Q waves
Low QRS Voltage
- Peak-to-trough QRS ≤5 mm in all limb leads and/or ≤10 mm in chest leads
- Causes: pericardial effusion, pleural effusion, COPD, cardiac amyloid, anasarca
Electrical Alternans
- Beat-to-beat alternation in QRS amplitude (and sometimes T waves)
- Classic finding in large pericardial effusion with cardiac tamponade
Pulmonary Embolism (Acute Cor Pulmonale)
- Sinus tachycardia (most common)
- S1Q3T3 pattern (deep S in I, Q and inverted T in III)
- Right axis deviation, new RBBB, atrial fibrillation
Summary Table of Key ECG Abnormalities
| Category | Pattern | Key Leads | Clinical Significance |
|---|---|---|---|
| LVH | Increased voltage + strain | V5-V6, I, aVL | Hypertension, aortic stenosis |
| RVH | Tall R in V1, right axis | V1, III, aVF | Pulmonary HTN, RV pressure overload |
| RBBB | rSR' | V1, V6 | Can be normal; also PE, ASD |
| LBBB | Wide QS, broad R | V1, V6 | Usually significant heart disease |
| STEMI | ST elevation | Localizes by territory | Emergency reperfusion needed |
| NSTEMI | ST depression, T inv | Diffuse | Subendocardial ischemia |
| Hyperkalemia | Peaked T → sine wave | All | Life-threatening |
| Long QT | QTc >440/460 ms | All | Risk of torsades de pointes |
| AF | No P waves, irregular | All | Stroke risk, rate control needed |
| Brugada | RBBB + V1-V3 ST elev | V1-V3 | Sudden cardiac death |
Sources: Harrison's Principles of Internal Medicine, 22nd ed. (2025), Chapter 247 (Electrocardiography); Fuster and Hurst's The Heart, 15th ed.
I need an complete comparison between Mitra, tricuspid, aortic, pulmonary stenosis and regurgitation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.