Cardiology drugs
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive, clinician-oriented overview of the major cardiology drug classes:
Major Cardiology Drug Classes - Clinical Overview
1. Renin-Angiotensin-Aldosterone System (RAAS) Blockers
ACE Inhibitors (e.g., ramipril, lisinopril, captopril, enalapril)
- Mechanism: Block conversion of angiotensin I to angiotensin II, reducing vasoconstriction and aldosterone secretion
- Key indications: HFrEF (all NYHA classes), post-MI LV dysfunction, hypertension, diabetic nephropathy, asymptomatic LV systolic dysfunction
- Evidence: RCTs conclusively show increased survival, reduced hospitalizations, and improved NYHA class in HFrEF. ACE inhibitors also delay progression to symptomatic HF in asymptomatic LV dysfunction.
- Key contraindications/cautions: Bilateral renal artery stenosis, pregnancy, angioedema, severe renal impairment (K+ monitoring required), concurrent NSAID use (worsens renal dysfunction)
- Common SE: Dry cough (bradykinin-mediated), hyperkalemia, hypotension, angioedema (rare but serious)
ARBs (e.g., candesartan, valsartan, losartan)
- Mechanism: Block AT1 angiotensin II receptors directly
- Role: First choice when ACE inhibitor is not tolerated. Candesartan reduces CV death + HF hospitalization. Valsartan is non-inferior to captopril post-MI.
- Advantage: No cough (no bradykinin accumulation)
ARNI - Sacubitril/Valsartan (Entresto)
- Mechanism: Combines neprilysin inhibitor (sacubitril, which raises natriuretic peptides, BNP) + ARB (valsartan)
- Role: Now the preferred RAAS blocker for HFrEF (NYHA II-III), replacing ACE inhibitors/ARBs as first-line. PARADIGM-HF trial showed superior mortality reduction vs. enalapril.
- Caution: Do NOT combine with ACE inhibitor (risk of angioedema). Wash out ACE inhibitor for 36 hours before starting.
Mineralocorticoid Receptor Antagonists / MRAs (e.g., spironolactone, eplerenone)
- Mechanism: Block aldosterone receptors; anti-fibrotic, diuretic
- Role: One of the four foundational HFrEF therapies. Also used in resistant hypertension, primary hyperaldosteronism.
- Key trial: RALES (spironolactone), EMPHASIS-HF (eplerenone)
- SE: Hyperkalemia (monitor K+), gynecomastia (spironolactone - eplerenone is more selective)
2. Beta-Blockers (e.g., carvedilol, metoprolol succinate, bisoprolol)
- Mechanism: Block beta-1 (and beta-2/alpha-1 for carvedilol) adrenergic receptors; reduce HR, BP, myocardial oxygen demand; anti-arrhythmic
- Key indications:
- HFrEF (all three evidence-based agents: carvedilol, metoprolol succinate, bisoprolol)
- Post-MI (reduce mortality and re-infarction)
- Angina (reduce oxygen demand)
- Hypertension
- Rate control in AF/flutter
- Specific arrhythmias (SVT, LVOT obstruction)
- Contraindications: Acute decompensated HF (don't initiate; can continue if already on them), high-degree AV block, severe reactive airway disease, severe bradycardia
- Key principle: In HFrEF, start at low dose, up-titrate slowly. Do not abruptly discontinue (rebound ischemia/arrhythmia).
3. SGLT2 Inhibitors (e.g., dapagliflozin, empagliflozin)
- Mechanism: Block sodium-glucose cotransporter 2 in the proximal tubule - glucosuria, natriuresis, osmotic diuresis, reduced preload/afterload, cardiorenal protection (exact cardioprotective mechanism still under study)
- Key indications: Now part of the four foundational HFrEF therapies alongside ARNI, beta-blocker, and MRA (2022 AHA/ACC/HFSA guidelines). Also indicated for HFpEF (dapagliflozin, empagliflozin). Type 2 diabetes with established CV disease.
- Trials: DAPA-HF, EMPEROR-Reduced, EMPEROR-Preserved, DELIVER
- SE: Genitourinary fungal infections, DKA (rare, especially in T1DM), Fournier's gangrene (rare), euglycemic DKA
- Note: Benefit is seen regardless of diabetes status
4. Diuretics
Loop Diuretics (e.g., furosemide, torsemide, bumetanide)
- Mechanism: Block Na+/K+/2Cl- cotransporter in the ascending loop of Henle
- Role: Congestion control in HF, pulmonary edema, acute decompensation. No proven mortality benefit but essential for symptom relief - nearly all symptomatic HF patients need them.
- SE: Hypokalemia, hyponatremia, hypomagnesemia, hyperuricemia, ototoxicity (high doses), prerenal azotemia
- Principle: Use minimum dose needed to maintain "dry weight." Dose should be flexible based on symptoms/weight.
Thiazide/Thiazide-like (e.g., hydrochlorothiazide, chlorthalidone, indapamide)
- Role: Hypertension, mild HF with preserved renal function. Chlorthalidone preferred over HCTZ for BP (longer duration, better outcome data)
- SE: Hypokalemia, hyperuricemia, glucose intolerance, dyslipidemia
5. Antiarrhythmic Drugs (Vaughan Williams Classification)
| Class | Drugs | Mechanism | Key Use |
|---|---|---|---|
| Ia | Quinidine, procainamide, disopyramide | Na+ channel block (intermediate kinetics) + K+ block | Rarely used; AF, VT |
| Ib | Lidocaine, mexiletine | Na+ channel block (fast kinetics) | Lidocaine: acute VT/VF. Mexiletine: chronic VT |
| Ic | Flecainide, propafenone | Na+ channel block (slow kinetics) | Paroxysmal AF (structurally normal heart only - CAST trial showed mortality increase post-MI) |
| II | Beta-blockers | See above | AF rate control, post-MI, SVT |
| III | Amiodarone, sotalol, dronedarone, dofetilide | K+ channel block (prolong repolarization/QT) | AF/VT/VF - amiodarone is broadest spectrum |
| IV | Verapamil, diltiazem | Ca2+ channel block (non-DHP) | SVT, AF rate control |
| Other | Adenosine, digoxin | - | Adenosine: acute SVT termination. Digoxin: AF rate control, HFrEF (symptom relief) |
Critical CAST lesson: Class I antiarrhythmics suppress ambient VECs but increase mortality post-MI - never use for ventricular ectopy suppression post-MI.
Amiodarone: Most effective antiarrhythmic; broad spectrum (Class I, II, III, IV effects). SE profile is significant: thyroid (hypo/hyper), pulmonary toxicity, hepatotoxicity, corneal deposits, photosensitivity, peripheral neuropathy. Monitor TFTs, LFTs, PFTs, and CXR annually.
6. Calcium Channel Blockers (CCBs)
Dihydropyridines (DHPs) - e.g., amlodipine, nifedipine, felodipine
- Mechanism: Block L-type Ca2+ channels in vascular smooth muscle (mainly) - arterial vasodilation
- Indications: Hypertension, angina (vasospastic and effort), Raynaud's
- Avoid in HFrEF: Some (e.g., nifedipine) may worsen outcomes; amlodipine and felodipine are considered safer in HF if needed
Non-DHPs - diltiazem, verapamil
- Mechanism: Also slow AV node conduction (negative chronotropy)
- Indications: AF rate control, SVT, angina, hypertension
- Avoid in: HFrEF (negative inotropic effect), in combination with beta-blockers (risk of severe bradycardia/heart block)
7. Nitrates (e.g., isosorbide mononitrate, isosorbide dinitrate, GTN/nitroglycerin)
- Mechanism: Donate NO - venous dilation (preload reduction) and coronary vasodilation at higher doses
- Indications: Angina (prophylaxis and acute relief), acute pulmonary edema, ACS, HFrEF (hydralazine-nitrate combination in Black patients: A-HeFT trial)
- SE: Headache (very common), hypotension, tachycardia (reflex)
- Key note: Nitrate tolerance develops with continuous use - a daily nitrate-free interval (8-10 hours) is needed
8. Statins (e.g., atorvastatin, rosuvastatin, simvastatin)
- Mechanism: HMG-CoA reductase inhibitors - reduce hepatic cholesterol synthesis, upregulate LDL receptors, pleiotropic anti-inflammatory effects
- Indications: All patients with atherosclerotic CV disease (ASCVD) regardless of baseline LDL. High-intensity statin (atorvastatin 40-80 mg or rosuvastatin 20-40 mg) is standard for established ASCVD or age ≤75 with prior CV event.
- SE: Myopathy/rhabdomyolysis (rare; check CK if symptoms), elevated transaminases, new-onset diabetes
- Drug interactions: CYP3A4 inhibitors increase myopathy risk (e.g., simvastatin + amiodarone)
9. Antiplatelet Agents
| Drug | Mechanism | Indication |
|---|---|---|
| Aspirin | COX-1 inhibition - blocks TXA2 | ACS, ASCVD (secondary prevention) |
| Clopidogrel | P2Y12 ADP receptor antagonist (prodrug, CYP2C19 activation) | ACS, PCI (DAPT), PAD |
| Ticagrelor | P2Y12 antagonist (direct, reversible) | ACS - superior to clopidogrel (PLATO trial) |
| Prasugrel | P2Y12 antagonist (prodrug, stronger/faster) | ACS with PCI (avoid in prior stroke/TIA, age >75, low weight) |
DAPT duration: 12 months after ACS; can shorten to 6 months with high bleeding risk after elective PCI.
10. Anticoagulants in Cardiology
| Drug | Class | Key Cardiac Use |
|---|---|---|
| Warfarin | Vitamin K antagonist | AF (mechanical valves, some antiphospholipid), VTE |
| Apixaban, rivaroxaban | Direct Xa inhibitors | AF (non-valvular), VTE, ACS (rivaroxaban 2.5 mg bid) |
| Dabigatran | Direct thrombin inhibitor | AF (non-valvular) |
| Heparin (UFH/LMWH) | Antithrombin III activation | ACS, bridging, STEMI |
Note: DOACs are now preferred over warfarin for non-valvular AF (lower bleeding risk, no INR monitoring). Warfarin remains the choice for mechanical heart valves.
11. Vasodilators and Other Agents
| Drug | Use | Notes |
|---|---|---|
| Hydralazine | Arteriolar dilator; HFrEF (with nitrates, especially Black patients) | Reflex tachycardia, lupus-like syndrome with high doses |
| Ivabradine | If-channel blocker (reduces HR without affecting inotropy) | HFrEF with HR ≥70 on max beta-blocker, sinus rhythm |
| Digoxin | Na+/K+-ATPase inhibitor | HFrEF symptom control, AF rate control (narrow therapeutic index - check levels) |
| Adenosine | A1 receptor agonist - AV node block | Acute termination of SVT/AVNRT |
| Ezetimibe | Blocks NPC1L1 (intestinal cholesterol absorption) | Add-on to statin for LDL reduction |
| PCSK9 inhibitors (evolocumab, alirocumab) | Monoclonal antibody - increases LDL receptor recycling | High-risk ASCVD with LDL not at goal on max statin |
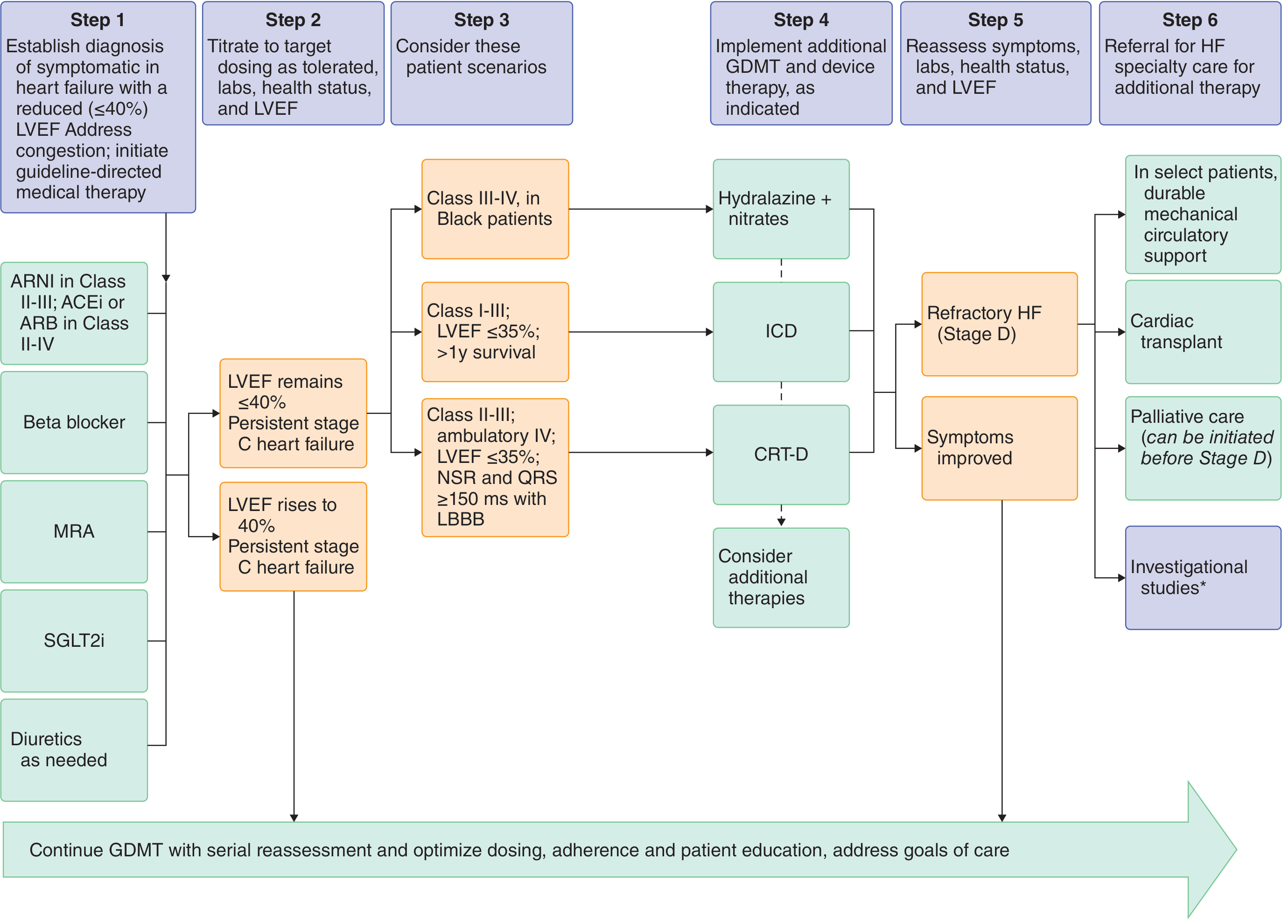
HFrEF Guideline-Directed Medical Therapy (GDMT) - 2022 AHA/ACC
The four foundational therapies that must be started in any order (titrated to evidence-based target doses):
- ARNI (sacubitril/valsartan) - preferred; or ACE inhibitor/ARB if not tolerated
- Beta-blocker (carvedilol, metoprolol succinate, or bisoprolol)
- MRA (spironolactone or eplerenone)
- SGLT2i (dapagliflozin or empagliflozin)
Plus loop diuretic as needed for congestion.
Sources: Goldman-Cecil Medicine, Braunwald's Heart Disease, Goodman & Gilman's Pharmacological Basis of Therapeutics, Fuster and Hurst's The Heart (15th ed)
This is a shared conversation. Sign in to Orris to start your own chat.