Cholinergic system
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Here is a comprehensive overview of the cholinergic system, synthesized from Ganong's, Goodman & Gilman's, Katzung's, and Lippincott's:
The Cholinergic System
1. Overview
The cholinergic system uses acetylcholine (ACh) as its neurotransmitter. It operates at multiple sites:
- Autonomic ganglia (both sympathetic and parasympathetic)
- Parasympathetic postganglionic nerve-effector organ junctions
- Somatic motor nerve-skeletal muscle junctions (neuromuscular junction)
- Select CNS pathways (basal forebrain, striatum, reticular formation)
ACh does not normally circulate in the blood. Its effects are discrete and short-lived because acetylcholinesterase (AChE) at cholinergic nerve endings rapidly degrades it.
2. Synthesis, Storage, Release, and Degradation
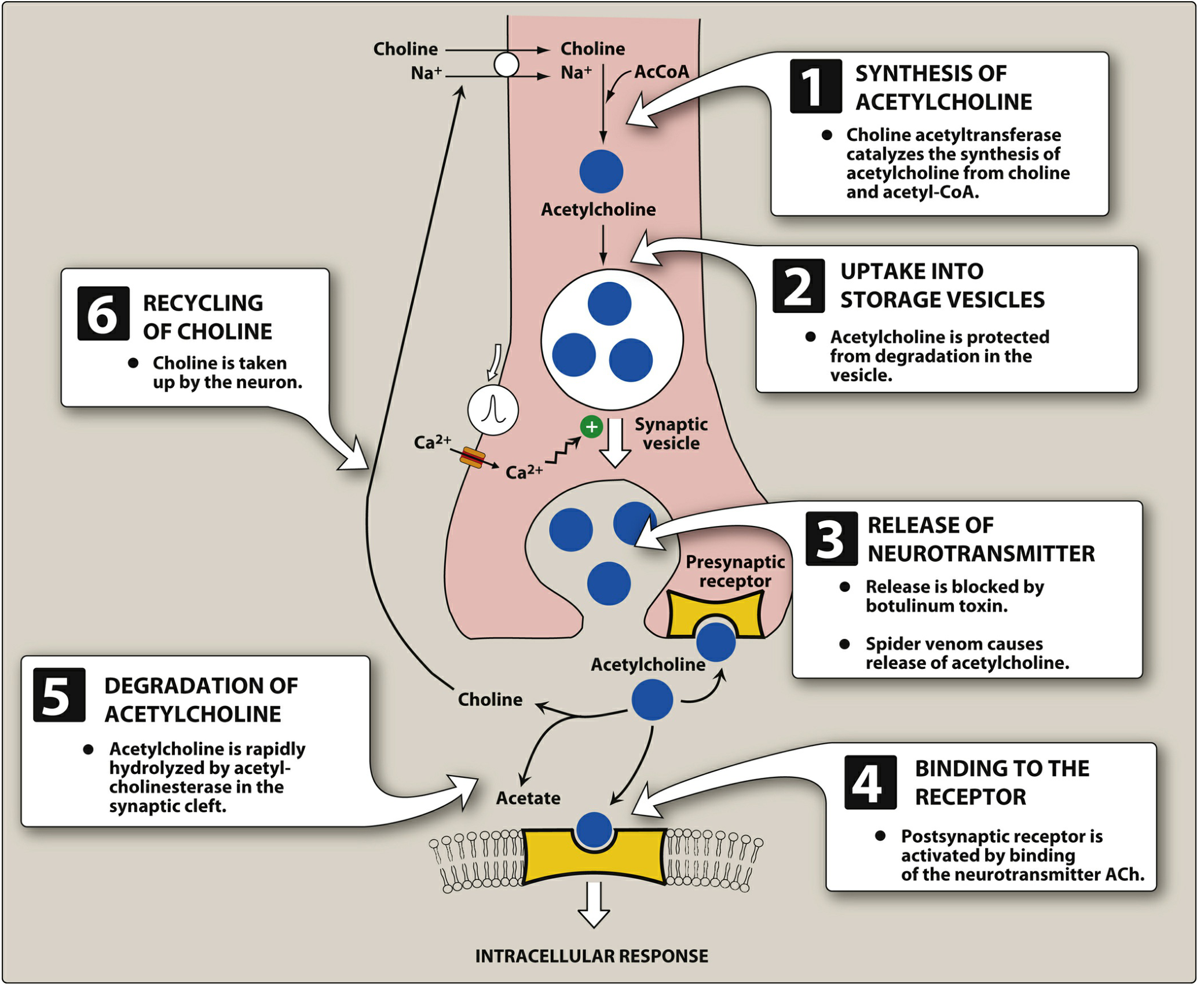
The life cycle of ACh involves six steps:
| Step | Event | Key Detail |
|---|---|---|
| 1 | Synthesis | Choline + Acetyl-CoA → ACh, catalyzed by choline acetyltransferase (ChAT). Choline uptake is the rate-limiting step; requires Na⁺-coupled transporter. |
| 2 | Storage | ACh packaged into vesicles by active transport. Vesicles also contain ATP (a cotransmitter) and proteoglycan. |
| 3 | Release | Action potential → voltage-gated Ca²⁺ channels open → Ca²⁺ influx → vesicle fusion → exocytosis. Botulinum toxin blocks release; black widow spider venom causes massive release. |
| 4 | Receptor binding | ACh binds muscarinic or nicotinic receptors on postsynaptic membranes or presynaptic autoreceptors. |
| 5 | Degradation | AChE rapidly cleaves ACh into choline + acetate in the synaptic cleft. |
| 6 | Choline recycling | Choline recaptured by high-affinity Na⁺-coupled transporter back into the neuron; hemicholinium blocks this step. |
- Lippincott Illustrated Reviews: Pharmacology, pp. 145-146
- Goodman & Gilman's Pharmacological Basis of Therapeutics
3. Cholinergic Receptors
ACh acts on two broad families of receptors:
A. Nicotinic Receptors (nAChR) - Ionotropic
- Structure: Pentameric ligand-gated ion channels composed of subunits from 17 known types (α1-10, β1-4, γ, δ). Two ACh molecules must bind simultaneously (one on each α subunit) for efficient channel opening.
- Mechanism: Agonist binding opens Na⁺/K⁺ channels → depolarization + Ca²⁺ influx.
- Subtypes and locations:
| Subtype | Location | Blocked by |
|---|---|---|
| N_N (neuronal, α3β4 dominant) | Autonomic ganglia, adrenal medulla | Hexamethonium |
| N_M (muscle) | Neuromuscular junction | D-tubocurarine (curare) |
| α4β2 | Most abundant in CNS (hippocampus, hypothalamus) | - |
| α7 (homomeric) | CNS and peripheral immune cells | - |
- The α4β2 subtype mediates nicotine addiction via dopamine release in the mesolimbic system.
- The α7 subtype is involved in cognition, pain, and anti-inflammatory signaling (reduces cytokine release from macrophages/microglia).
- Katzung's Basic and Clinical Pharmacology, 16th Ed., pp. 544-552
B. Muscarinic Receptors (mAChR) - Metabotropic (GPCR)
All five subtypes are G protein-coupled receptors (GPCRs). Non-selective antagonists: atropine, scopolamine, ipratropium.
| Subtype | G Protein / Effector | Location | Key Function |
|---|---|---|---|
| M1 | Gq → PLC → IP3/DAG → ↑Ca²⁺ | Cortex, hippocampus, gastric glands | Cognition, gastric acid secretion; M1 KO → impaired forebrain plasticity |
| M2 | Gi/Go → ↓adenylyl cyclase; opens K⁺ channels | Heart (SA/AV node), presynaptic terminals | ↓Heart rate, ↓AV conduction; presynaptic autoreceptor inhibiting ACh release |
| M3 | Gq → PLC → ↑Ca²⁺ | Smooth muscle, glands, eye, hypothalamus | Contraction of smooth muscle, glandular secretion; M3 KO → reduced appetite |
| M4 | Gi/Go → ↓adenylyl cyclase | Striatum, CNS | Modulation of dopamine in striatum |
| M5 | Gq → PLC | CNS, dopaminergic neurons | Modulation of mesolimbic dopamine |
- Agonists: ACh, carbachol, oxotremorine, pilocarpine (M1/M3 selective), cevimeline
- Selective antagonists: pirenzepine (M1), AF-DX 116 (M2), darifenacin (M3)
- Goodman & Gilman's, Table 16-3; Ganong's, p. 267
4. Autonomic Ganglionic Transmission
At autonomic ganglia, ACh produces two types of postsynaptic potentials in postganglionic neurons:
-
Fast EPSP - via nicotinic (N_N) receptors → rapid depolarization, action potential generation
-
Slow EPSP - via muscarinic (M1) receptors on the postganglionic neuron → modulates and regulates ganglionic transmission
-
Ganong's Review of Medical Physiology, 26th Ed., p. 267
5. Peripheral Parasympathetic Effects (via M2 and M3)
| Organ | Cholinergic (Parasympathetic) Effect |
|---|---|
| Heart (SA node) | Decreased heart rate (M2 → ↑K⁺ conductance → hyperpolarization) |
| Heart (AV node) | Decreased conduction velocity |
| Heart (atria) | Decreased contractility |
| Sphincter muscle of iris | Contraction → miosis |
| Ciliary muscle | Contraction → accommodation for near vision |
| Bronchial smooth muscle | Bronchoconstriction |
| GI smooth muscle | Increased motility and secretion |
| Bladder detrusor | Contraction (urination) |
| Salivary/lacrimal glands | Increased secretion |
| Blood vessels (endothelium) | Vasodilation via NO release |
- Ganong's Review of Medical Physiology, Table 13-1
6. CNS Cholinergic Pathways
Eight major ACh-containing nuclei in the CNS project diffusely throughout the brain:
- Basal nucleus of Meynert → cortex (memory, cognition)
- Medial septal nucleus → hippocampus
- Reticular formation → arousal, attention
- Neostriatum → motor control, reward
Clinical relevance:
-
Loss of cholinergic neurons in these pathways is the hallmark of Alzheimer's disease (associated with marked reductions in ChAT and ACh concentrations)
-
Nicotinic receptor activation in the CNS (especially α4β2) promotes dopamine release in the mesolimbic system → basis of nicotine's addictive and alerting effects
-
Katzung's Basic and Clinical Pharmacology, 16th Ed., p. 592
7. Pharmacological Modulation Summary
| Target | Drug Class | Examples | Effect |
|---|---|---|---|
| AChE | Anticholinesterases | Neostigmine, physostigmine, organophosphates | ↑ACh (indirect agonism) |
| Muscarinic receptors | Muscarinic agonists | Pilocarpine, bethanechol, carbachol | Direct cholinomimetic |
| Muscarinic receptors | Muscarinic antagonists | Atropine, scopolamine, ipratropium | Block parasympathetic effects |
| Nicotinic (NMJ) | NMJ blockers | D-tubocurarine, succinylcholine | Muscle relaxation |
| Nicotinic (ganglia) | Ganglion blockers | Hexamethonium | ↓Autonomic ganglionic transmission |
| ACh synthesis | Hemicholinium | Hemicholinium-3 | Blocks choline reuptake |
| ACh release | Botulinum toxin | Botox | Prevents ACh exocytosis |
| ACh vesicle loading | Vesamicol | Vesamicol | Blocks vesicular ACh transport |
Key Clinical Correlates
- Organophosphate poisoning / nerve agents: Irreversible AChE inhibition → SLUDGE syndrome (Salivation, Lacrimation, Urination, Defecation, GI distress, Emesis) + nicotinic effects (muscle fasciculations, paralysis). Treat with atropine + pralidoxime.
- Myasthenia gravis: Autoantibodies against N_M receptors at the NMJ → muscle weakness. AChE inhibitors (pyridostigmine) are first-line.
- Alzheimer's disease: Cholinergic deficit treated with AChE inhibitors (donepezil, rivastigmine, galantamine).
- Glaucoma: Pilocarpine (M3 agonist) contracts ciliary muscle and sphincter pupillae → opens trabecular meshwork → ↓intraocular pressure.
This is a shared conversation. Sign in to Orris to start your own chat.