Flat foot
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pes planus" OR "flat foot" management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile everything.
Flat Foot (Pes Planus)
Definition
Flat foot is a deformity characterized by flattening of the medial longitudinal arch, with the entire plantar surface making ground contact. All children under 3 years have flat feet (obscured by a fat pad), and the arch develops over time - but 15% of adults retain flat feet, influenced by familial and racial factors. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Classification
The single most important clinical distinction is flexible vs. rigid (fixed):
| Type | Characteristics |
|---|---|
| Flexible | Arch returns and heel corrects to varus on tiptoe; subtalar movements full and pain-free |
| Rigid | Arch fails to return and heel remains in valgus on tiptoe; subtalar movements restricted and painful |
- Bailey and Love's, 28th Ed.
Causes
Physiological / Developmental
- Normal variant (most common) - frequently familial, almost always bilateral
- Ligamentous laxity / hyperlaxity syndromes (e.g. Marfan syndrome)
Acquired (Pathological)
- Tibialis posterior tendon dysfunction (PTTD) - most common cause of Adult Acquired Flatfoot Deformity (AAFD)
- Spring (calcaneonavicular) ligament rupture
- Tarsometatarsal arthritis/injury
- Charcot neuroarthropathy (e.g. diabetes)
- Inflammatory/degenerative arthritis (subtalar, talonavicular, naviculocuneiform joints)
Rigid Flatfoot
-
Tarsal coalition (failure of mesenchymal segmentation) - affects 1 in 100 people, 50% bilateral, typically presents in adolescence
-
Bailey and Love's 28th Ed.; Miller's Review of Orthopaedics, 9th Ed.
Clinical Features
Symptoms:
- Medial ankle/foot pain early in AAFD
- Progressive arch collapse
- Lateral ankle pain late (due to subfibular impingement)
- Aching midfoot, pretibial pain
Signs:
- Asymmetric hindfoot valgus (standing)
- Depressed arch
- Abducted forefoot
- "Too-many-toes" sign: viewed from behind, more than 5 toes are visible lateral to the heel on the affected side - indicates forefoot abduction in AAFD

Key clinical tests:
- Single-limb heel rise test: inability or pain = significant PTT dysfunction
- Windlass test: ask patient to stand on tiptoes - arch should form; failure = fixed flat foot
- Jack's test: with patient standing, lift great toe - arch should reconstitute in flexible flat foot; failure = fixed flat foot
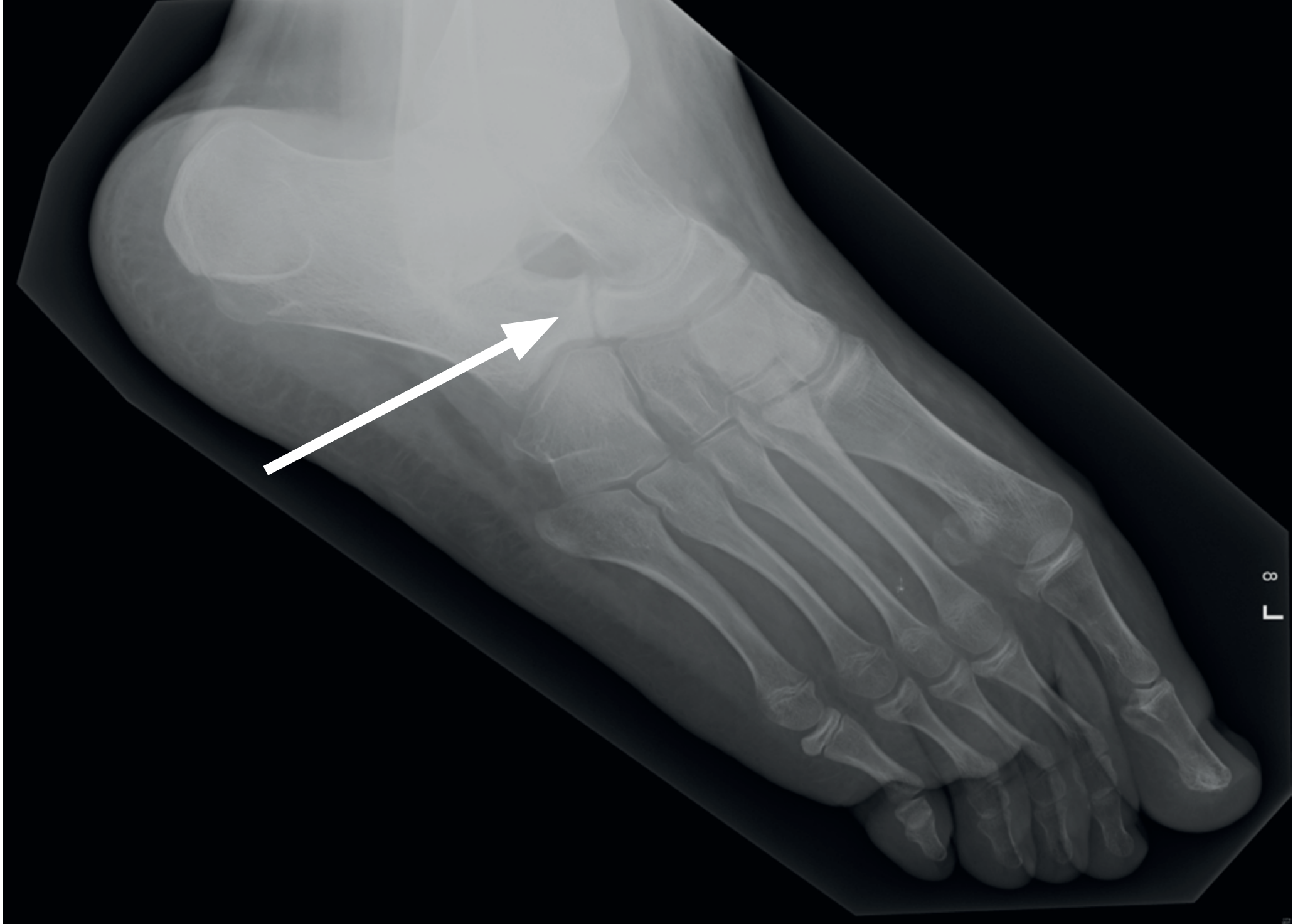
Radiographic Assessment
Weight-bearing X-rays are standard:
| Radiograph | Measurement | Normal | Pes Planus |
|---|---|---|---|
| Lateral | Meary angle (talar-first metatarsal angle) | 0-4° | >4° (negative/plantar-directed sag) |
| Lateral | Calcaneal pitch | 17-32° | Reduced |
| AP | TN (talonavicular) uncoverage | Minimal | Increased (forefoot abduction) |
For tarsal coalition:
- C-sign / dorsal talar beaking on X-ray (middle facet / talocalcaneal coalition)
- Elongated anterior process of calcaneus on lateral view (calcaneonavicular coalition)
- CT scan for definitive evaluation
AAFD / PTTD Staging & Treatment
The PTT is the primary dynamic support of the arch; the spring (calcaneonavicular) ligament is the primary static stabilizer of the talonavicular joint. PTTD has a zone of hypovascularity 2-6 cm proximal to the navicular insertion - Miller's Review of Orthopaedics, 9th Ed.
Stage I - Tenosynovitis, no deformity
- Conservative: Immobilization (cast or boot), then arch support/medial heel wedge orthotic
- Surgical: PTT synovectomy
Stage II - Flexible deformity; PTT functionally incompetent
- Conservative (first-line, at least 6 months): Ankle-foot orthosis (AFO) + physiotherapy (highest success rate); full-length orthotic with arch support + medial heel wedge
- Surgical (if conservative fails):
- FDL or FHL tendon transfer into navicular to reconstruct PTT
- Gastrocnemius recession (if contracture present)
- Spring ligament reconstruction (synthetic tape augmentation now widely accepted)
- Stage IIA (hindfoot valgus, <40% TN uncoverage): Medial slide calcaneal osteotomy
- Stage IIB (hindfoot valgus + significant forefoot abduction): Lateral column lengthening (Evans osteotomy) ± medial slide osteotomy
Stage III - Fixed (rigid) deformity
- Surgical: Triple arthrodesis (subtalar + talonavicular + calcaneocuboid)
Stage IV - Stage III + ankle valgus/arthritis
- TAR (total ankle replacement) or tibiotalar + subtalar arthrodesis
Flexible Pes Planus (Pediatric / Physiological)
- Foot is flat only with standing; arch reconstitutes with toe-walking or non-weight-bearing
- Commonly associated with ligamentous laxity and mild lower extremity rotational problems
- Asymptomatic cases: observation only; orthoses do NOT alter natural history
- Symptomatic cases: arch supports and shoes with stiffer soles for pain relief (not corrective); surgical correction reserved for severe cases failing extensive non-operative treatment
- Miller's Review of Orthopaedics, 9th Ed.
Tarsal Coalition
- Rigid flat foot in an adolescent should raise suspicion
- Peroneal muscle spasm is a consequence, not a cause, of tarsal coalition (peroneal spastic flat foot)
- Types: calcaneonavicular (most common, may have some residual motion), talocalcaneal (middle facet most common)
- Treatment: resection (if <50% of middle facet involved); arthrodesis if >50% or severe deformity
- Campbell's Operative Orthopaedics, 15th Ed. 2026; Miller's Review of Orthopaedics, 9th Ed.
Summary of Key Points
- The painless, flexible flat foot needs no treatment in most cases
- The symptomatic rigid flat foot requires investigation (tarsal coalition, PTTD)
- PTTD is the most common cause of AAFD in adults; occurs especially in overweight women
- The single-limb heel rise test is the most important clinical test for PTT integrity
- Orthoses do not correct deformity but can provide symptomatic relief
- Surgery is a major undertaking but is highly successful at achieving symptomatic relief in carefully selected patients
Recent evidence note: A 2025 meta-analysis (PMID 40516166) found that foot orthoses alter lower extremity kinematics and kinetics in runners with asymptomatic flatfeet, providing biomechanical support for their use even in asymptomatic runners at risk of injury.
This is a shared conversation. Sign in to Orris to start your own chat.