Make a one-page reference card on pterygium definition etiology pathogenesis clinical features diagnosis and treatment with diagram
pterygium eye definition etiology pathogenesis clinical features diagnosis treatment
A detailed one-page medical reference card titled "PTERYGIUM - Quick Reference Card" for ophthalmology students and clinicians. The card is structured in clean, color-coded sections on a white background with a professional medical layout. Include the following sections clearly labeled: 1. DEFINITION (blue header): "Triangular fibrovascular sub-epithelial ingrowth of degenerative bulbar conjunctival tissue over the limbus onto the cornea. From Greek 'pterygos' = wing. Also called Surfer's Eye." 2. ETIOLOGY (green header): UV radiation (most important), dry/dusty/windy environments, geographic - equatorial regions, genetic predisposition, chronic ocular surface dryness, low latitude residence 3. PATHOGENESIS (orange header): UV-induced limbal stem cell damage → elastotic degeneration of subepithelial stromal collagen → fibrovascular proliferation → invasion of Bowman layer → corneal encroachment. P53 mutation, MMP upregulation, VEGF-mediated neovascularization 4. PARTS DIAGRAM: A clear labeled anatomical diagram of pterygium showing the three parts: CAP (avascular halo at advancing edge), HEAD (invades cornea), BODY (on conjunctiva, vascularized). Also label Stocker line (iron deposition) and Fuchs islets. Include a simple wing-shaped triangle overlaid on an eye schematic showing nasal location. 5. CLINICAL FEATURES (purple header): Symptoms: irritation/grittiness, foreign body sensation, redness, reduced vision (axis obscuration or astigmatism), cosmetic concern. Signs: wing-shaped fibrovascular growth at 3 or 9 o'clock (nasal > temporal), Stocker line (iron deposition in corneal epithelium), Fuchs islets, dellen effect 6. DIAGNOSIS (teal header): Clinical - slit-lamp examination. Grading: Grade I (episcleral vessels visible), Grade II (vessels partially obscured), Grade III (vessels fully obscured). Rule out: CIN (conjunctival intraepithelial neoplasia), pseudopterygium, limbal dermoid. Biopsy for atypical lesions. 7. TREATMENT (red header): - Medical: lubricants, topical steroids, UV-protective sunglasses - Surgery: INDICATIONS - visual axis encroachment, induced astigmatism, motility restriction, cosmesis - Techniques: Bare sclera (high recurrence ~80%) | Conjunctival autograft (gold standard, recurrence 2-40%) | Amniotic membrane graft (recurrence 2.6-10.7%) - Adjuvants: Mitomycin C, beta-irradiation (reduce recurrence) 8. KEY FACTS BOX (yellow): Pseudopterygium - attached only at apex; passes probe test. Stocker line = iron deposition. Avoid bare sclera alone. Recurrence risk reduced by conjunctival autograft + MMC. The card should look professional, use colored section boxes, include the anatomical parts diagram prominently, and fit all content on one page in a visually organized two-column layout.
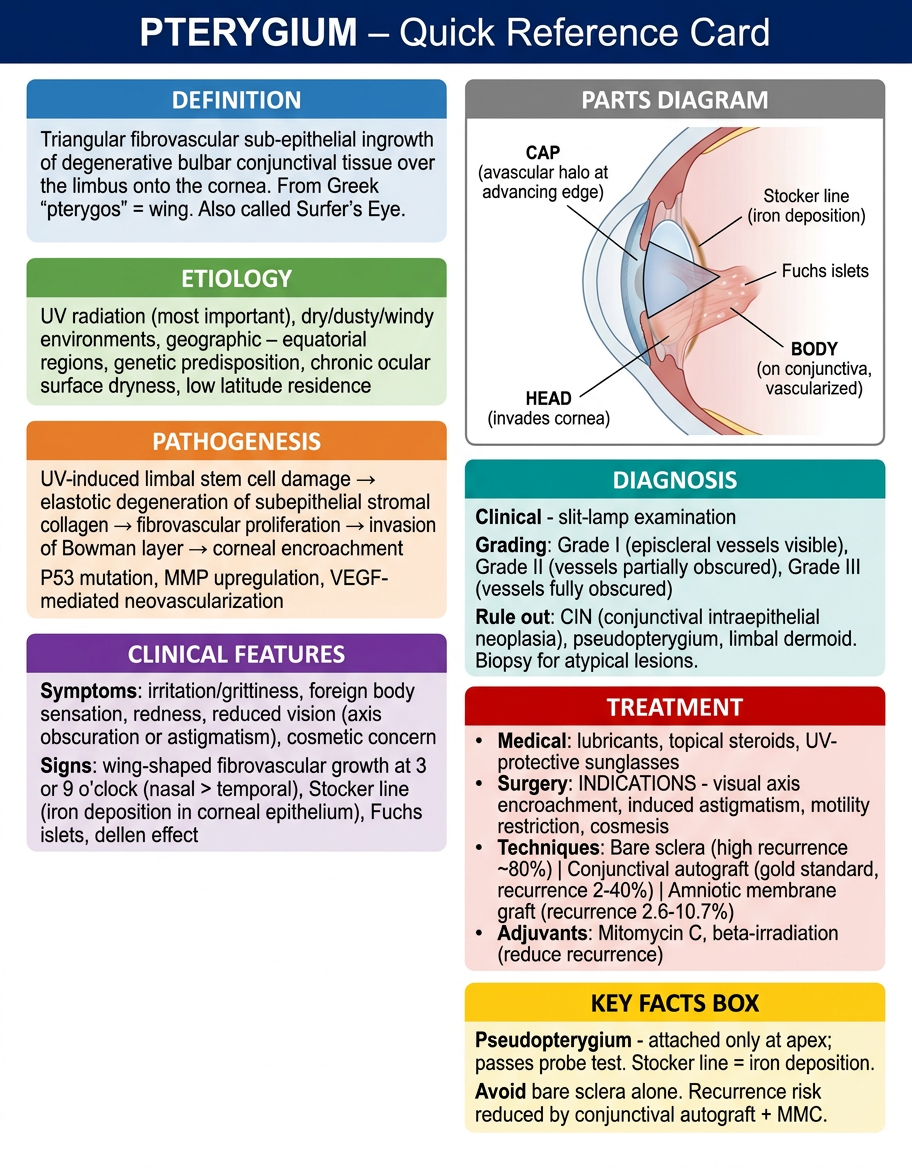
PTERYGIUM - Quick Reference Card
DEFINITION
- Kanski's Clinical Ophthalmology, p.215
ETIOLOGY
| Factor | Details |
|---|---|
| UV radiation | Most important; cumulative exposure damages limbal stem cells |
| Geographic | Higher prevalence near equator; <2% above 40th parallel vs 5-15% at 28-36° latitude |
| Environmental | Chronic dryness, dust, wind, heat |
| Genetic | Tends to run in families |
| Occupation | Outdoor workers, farmers, fishermen, surfers |
PATHOGENESIS
ANATOMY OF PTERYGIUM (Three Parts)
[ BODY ]──────[ HEAD ]──[ CAP ]─ → cornea
(vascularized (invades (avascular
conjunctival) cornea) advancing edge)
↑ Stocker line (iron deposition ahead of cap)
↑ Fuchs islets (discrete epithelial cell clusters at edge)
CLINICAL FEATURES
- Small lesions: often asymptomatic
- Irritation, grittiness (dellen effect - localized tear film disruption)
- Foreign body sensation
- Redness / intermittent inflammation (pterygitis)
- Reduced vision (axis encroachment or induced astigmatism)
- Contact lens intolerance
- Cosmetic concern
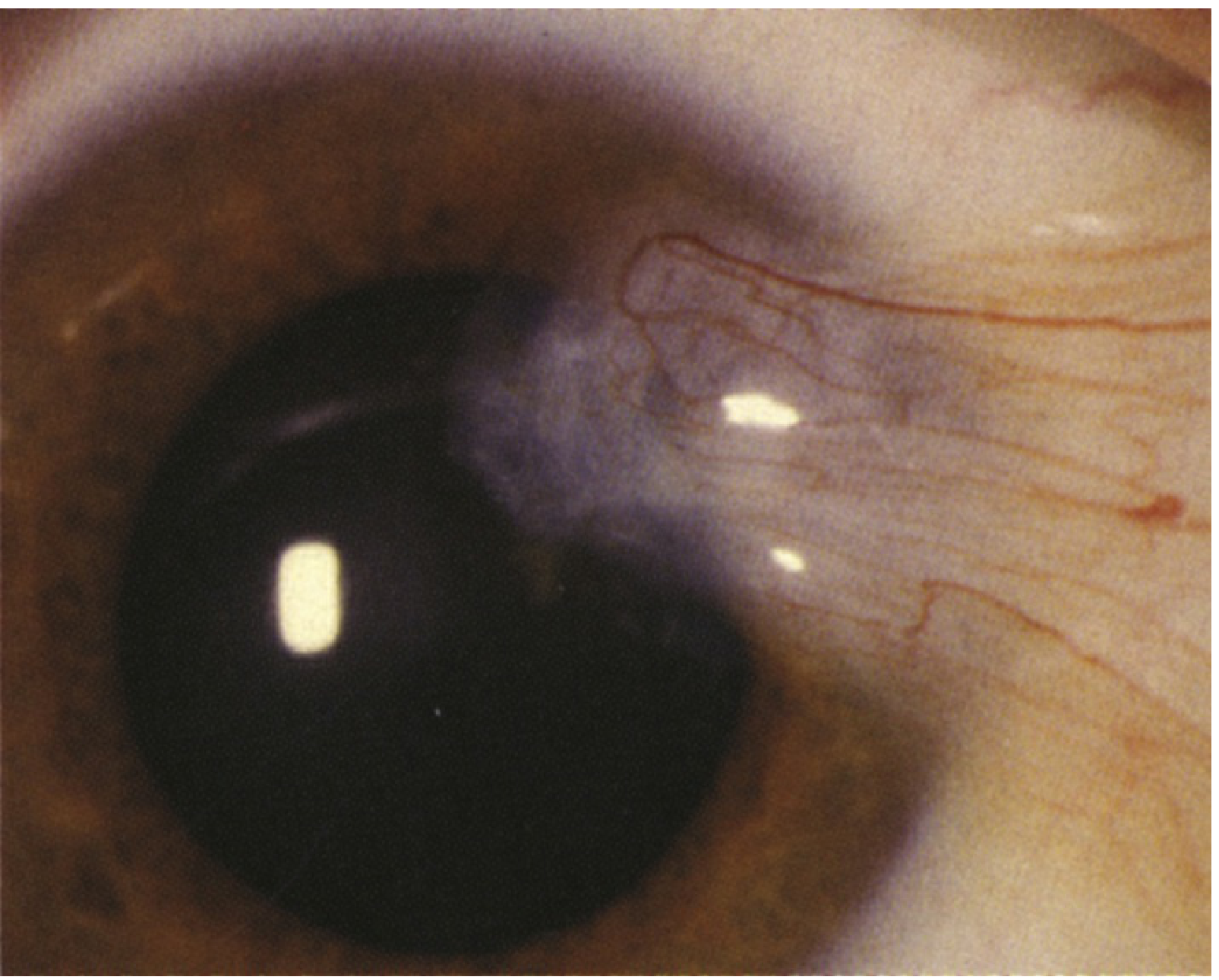
- Wing-shaped pink-red fibrovascular growth, nasal > temporal
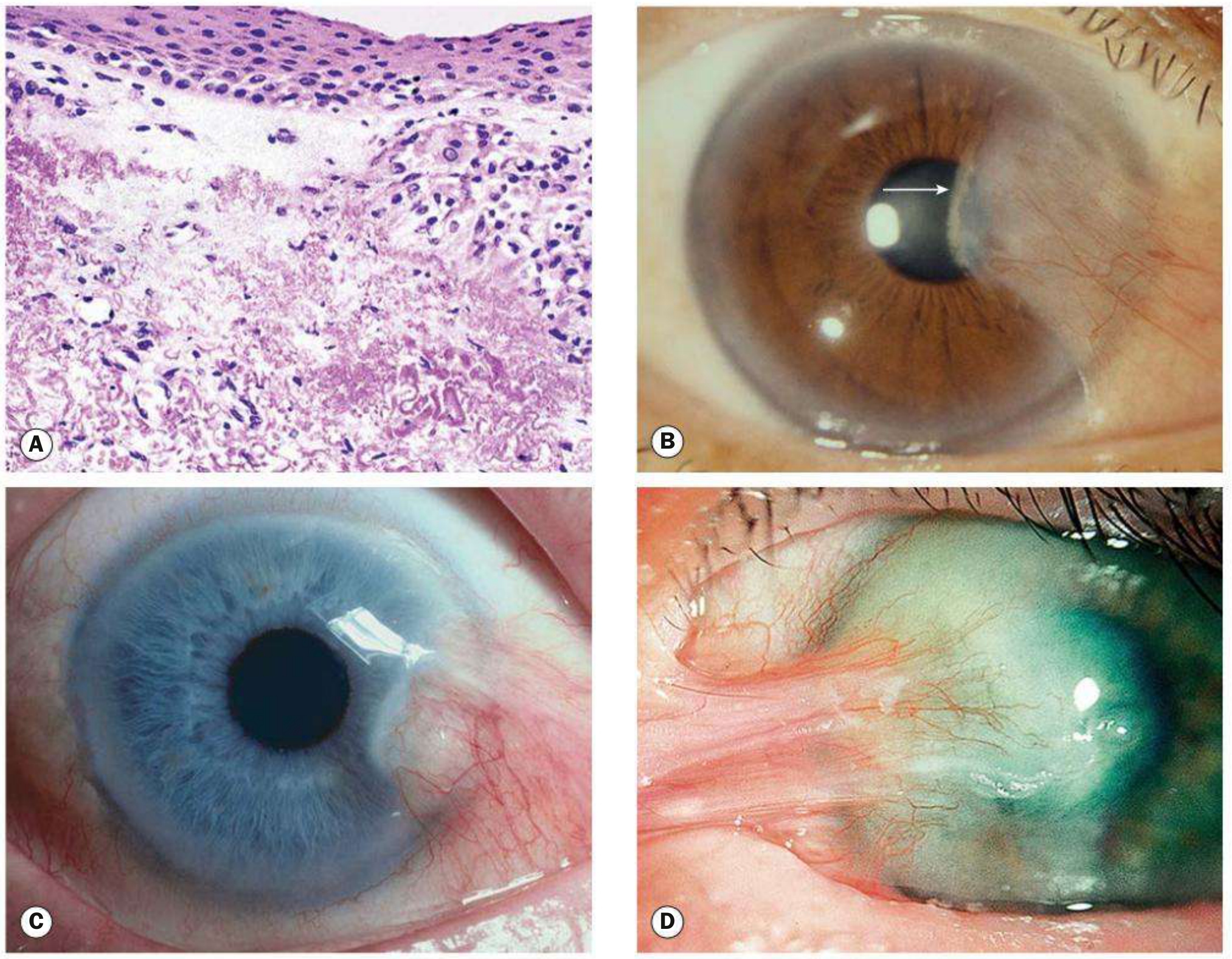
- Stocker line - linear iron deposition in corneal epithelium anterior to head
- Fuchs islets at advancing edge
- Dellen (corneal thinning adjacent to elevated head)
- Advanced: subconjunctival fibrosis, restricted ocular excursion
| Grade | Scleral Vessels |
|---|---|
| I (atrophic) | Clearly visible through pterygium |
| II (intermediate) | Partially obscured |
| III (fleshy) | Completely obscured |
DIAGNOSIS
- Clinical: Slit-lamp examination - characteristic location, wing-shape, slit-beam assessment of depth
- Topography/Keratometry: Assess induced astigmatism
- Biopsy: For atypical pterygia to exclude Conjunctival Intraepithelial Neoplasia (CIN)
- Pseudopterygium - attached only at apex (probe can pass under body); associated with prior trauma/burn/ulcer
- CIN - papillomatous, velvety, not necessarily 3 or 9 o'clock
- Limbal dermoid
- Pinguecula (does not encroach onto cornea)
TREATMENT
- Artificial tears / lubricants
- Topical steroids (short course for inflammation)
- UV-protective sunglasses (primary prevention)
- Encroachment toward visual axis
- Significant induced astigmatism
- Restricted ocular motility
- Cosmesis / recurrent inflammation unresponsive to drops
| Technique | Recurrence Rate | Notes |
|---|---|---|
| Bare sclera excision | ~80% | Not recommended alone |
| Conjunctival autograft | 2-40% (gold standard) | Harvested from superior/upper temporal limbus; can use fibrin glue (TISSEEL) instead of sutures |
| Amniotic membrane graft | 2.6-10.7% (primary); up to 37.5% (recurrent) | Preserves bulbar conjunctiva |
- Mitomycin C (MMC) - antifibrotic, inhibits fibroblasts; applied intraoperatively
- Beta-irradiation - reduces recurrence
- Peripheral lamellar keratoplasty - for deep lesions
TIP (Kanski's): Recurrence risk is best reduced by conjunctival autograft + MMC application.
CLINICAL IMAGES (from Kanski's, Fig. 6.28)