What is Hamburger phenomenon
Hamburger Phenomenon (Chloride Shift)
Mechanism - Step by Step
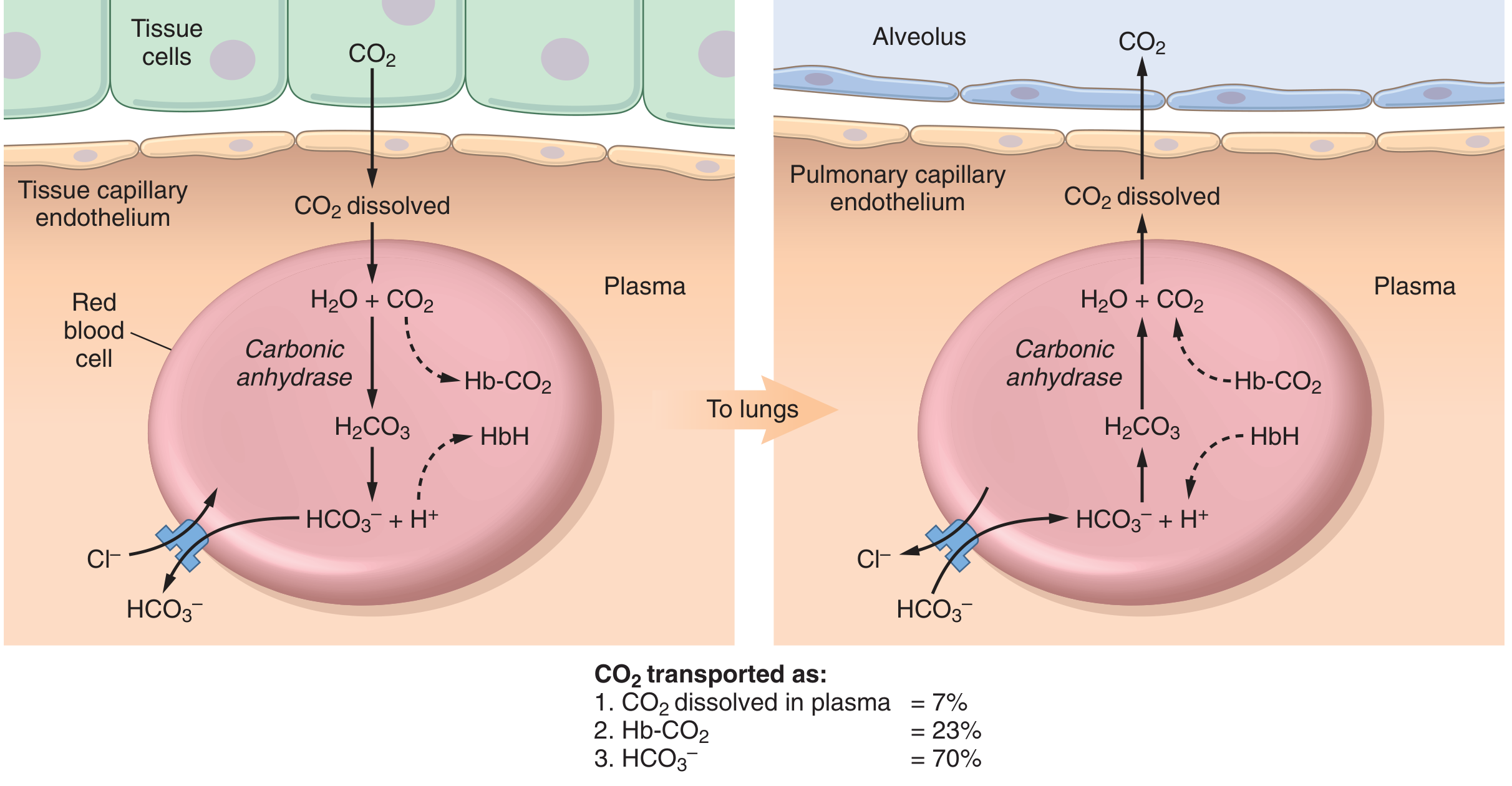
- CO2 produced by metabolism diffuses into RBCs
- Inside the RBC, carbonic anhydrase catalyzes the rapid hydration of CO2:
- CO2 + H2O → H2CO3 → H+ + HCO3-
- This reaction is ~5,000x faster inside the RBC than in plasma
- The H+ ions are buffered by hemoglobin (forming HHb), which prevents dangerous acidification
- The large amount of HCO3- generated inside the RBC creates a concentration gradient - HCO3- begins to diffuse out into the plasma
- To maintain electrical neutrality, Cl- moves from plasma INTO the RBC in exchange - this is the Hamburger/chloride shift
- The transporter responsible is Anion Exchanger 1 (AE1), also called Band 3 protein, a major membrane protein of the RBC
- As CO2 is offloaded into the alveoli, the reaction reverses
- HCO3- moves back into the RBC, Cl- exits
- H2CO3 re-forms CO2 + H2O, and CO2 is exhaled
Key Points
| Feature | Detail |
|---|---|
| Also called | Chloride shift, isohydric shift |
| Named after | H.J. Hamburger (Dutch physiologist) |
| Site | RBC membrane |
| Transporter | AE1 / Band 3 protein |
| Direction in tissues | HCO3- out, Cl- in |
| Direction in lungs | HCO3- in, Cl- out |
| Speed | Essentially complete within ~1 second |
| Result on venous RBC | Higher Cl- content vs arterial RBC |
Why It Matters
- It is the mechanism by which ~70% of all CO2 is carried from tissues to lungs (as dissolved HCO3- in plasma)
- It maintains electrical neutrality across the RBC membrane during CO2 loading
- It also causes a slight increase in RBC osmolarity (because each CO2 entering the cell adds one osmotically active particle - either HCO3- or Cl-), so venous RBCs are slightly larger and venous hematocrit is about 3% higher than arterial hematocrit
- In the lungs, the reverse Hamburger shift removes HCO3- from plasma back into the RBC for reconversion to CO2
Discuss composition, function and regulation of pancreatic juice?
Pancreatic Juice - Composition, Function, and Regulation
Overview
| Component | Produced By | Contents |
|---|---|---|
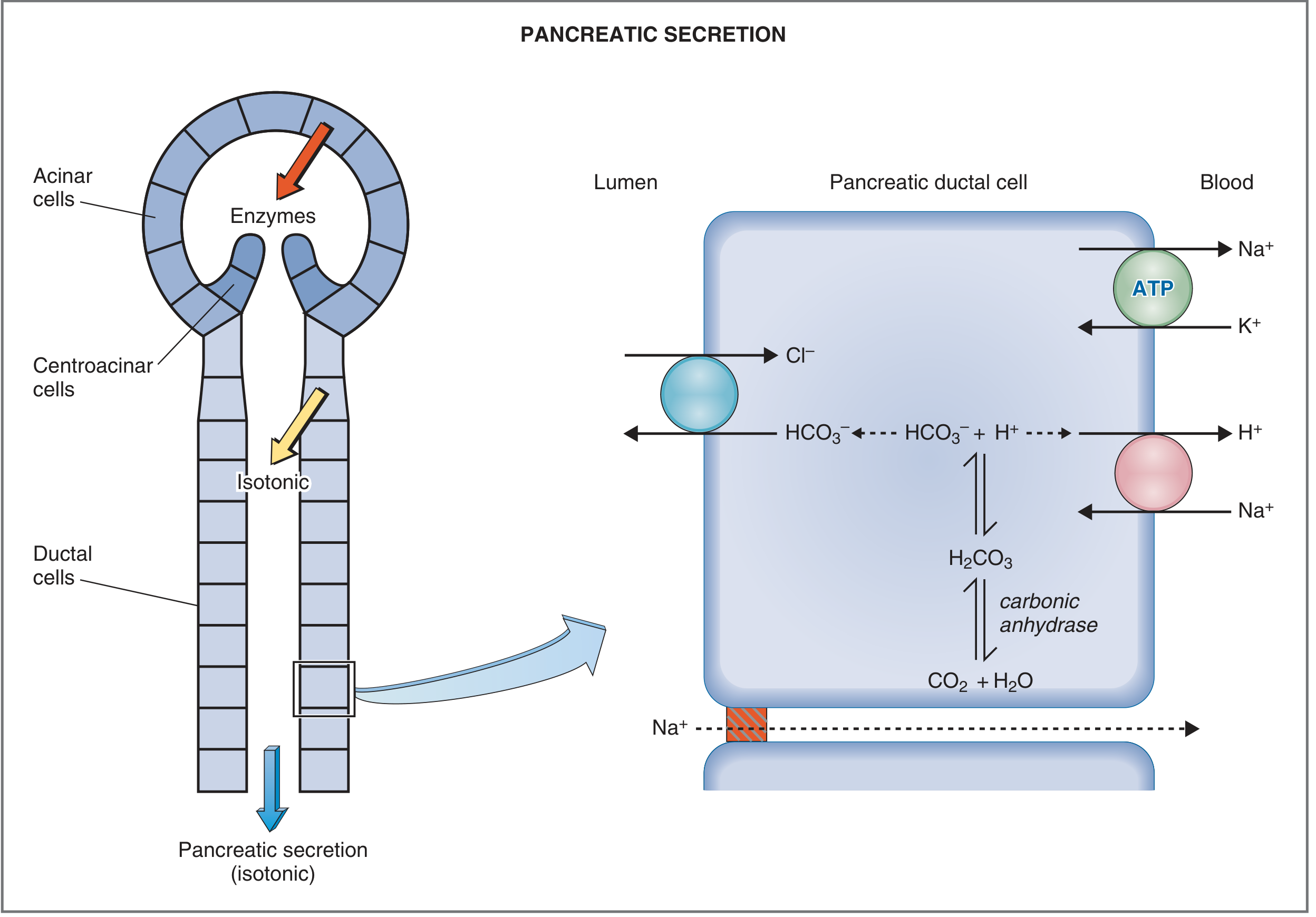
| Enzymatic component | Acinar cells | Digestive enzymes (stored as zymogen granules) |
| Aqueous component | Centroacinar & ductal cells | NaHCO3-rich fluid, Na+, K+, Cl- |
1. Composition
A. Inorganic (Aqueous) Component
- HCO3-: ~113 mEq/L (vs. 24 mEq/L in plasma) - the defining feature
- Na+ and K+: Same concentration as plasma
- Cl-: Inversely related to HCO3- concentration (varies with flow rate)
- At HIGH flow rates (e.g., after secretin stimulation): HCO3- is highest (up to 145 mEq/L), Cl- is lowest
- At LOW flow rates (basal): HCO3- is lowest, Cl- is highest
- Na+ and K+ remain constant regardless of flow rate
B. Enzymatic Component
Proteolytic Enzymes (secreted as INACTIVE precursors = zymogens)
| Zymogen (inactive) | Active form | Action |
|---|---|---|
| Trypsinogen | Trypsin | Cleaves proteins/peptides at Arg, Lys residues |
| Chymotrypsinogen | Chymotrypsin | Cleaves at aromatic amino acid residues |
| Procarboxypeptidase A & B | Carboxypeptidase A & B | Cleaves C-terminal amino acids |
| Proelastase | Elastase | Cleaves elastin and other proteins |
| Prophospholipase A2 | Phospholipase A2 | Splits fatty acid from phospholipids |
- Enterokinase (enteropeptidase) on intestinal mucosa cleaves trypsinogen → trypsin
- Trypsin then activates all other zymogens (including autocatalytic activation of more trypsinogen)
Carbohydrate-Digesting Enzymes (secreted ACTIVE)
- Pancreatic amylase: Hydrolyzes starch, glycogen and most polysaccharides (except cellulose) → disaccharides (maltose) and trisaccharides
Fat-Digesting Enzymes (secreted ACTIVE)
- Pancreatic lipase: Hydrolyzes triglycerides → fatty acids + monoglycerides (requires colipase)
- Cholesterol esterase: Hydrolyzes cholesterol esters
- Phospholipase A2: Cleaves fatty acids from phospholipids (activated from prophospholipase A2 by trypsin)
2. Functions
A. Neutralization of Gastric Acid
HCl + NaHCO3 → NaCl + H2CO3 → NaCl + H2O + CO2
- It protects the duodenal mucosa from acid damage (prevents duodenal ulcers)
- It creates the optimal pH (7.0-8.0) for pancreatic enzymes to function
B. Digestion of Macronutrients
- Proteins: Trypsin, chymotrypsin, elastase produce small peptides; carboxypeptidase releases free amino acids
- Carbohydrates: Amylase converts starch to disaccharides/trisaccharides for further brush-border digestion
- Fats: Lipase + colipase cleave triglycerides; cholesterol esterase and phospholipase handle other lipids
C. Trypsin Inhibitor - Self-protection
3. Regulation
Primary Stimuli (Three Basic Stimuli)
| Stimulus | Source | Target Cell | Effect | 2nd Messenger |
|---|---|---|---|---|
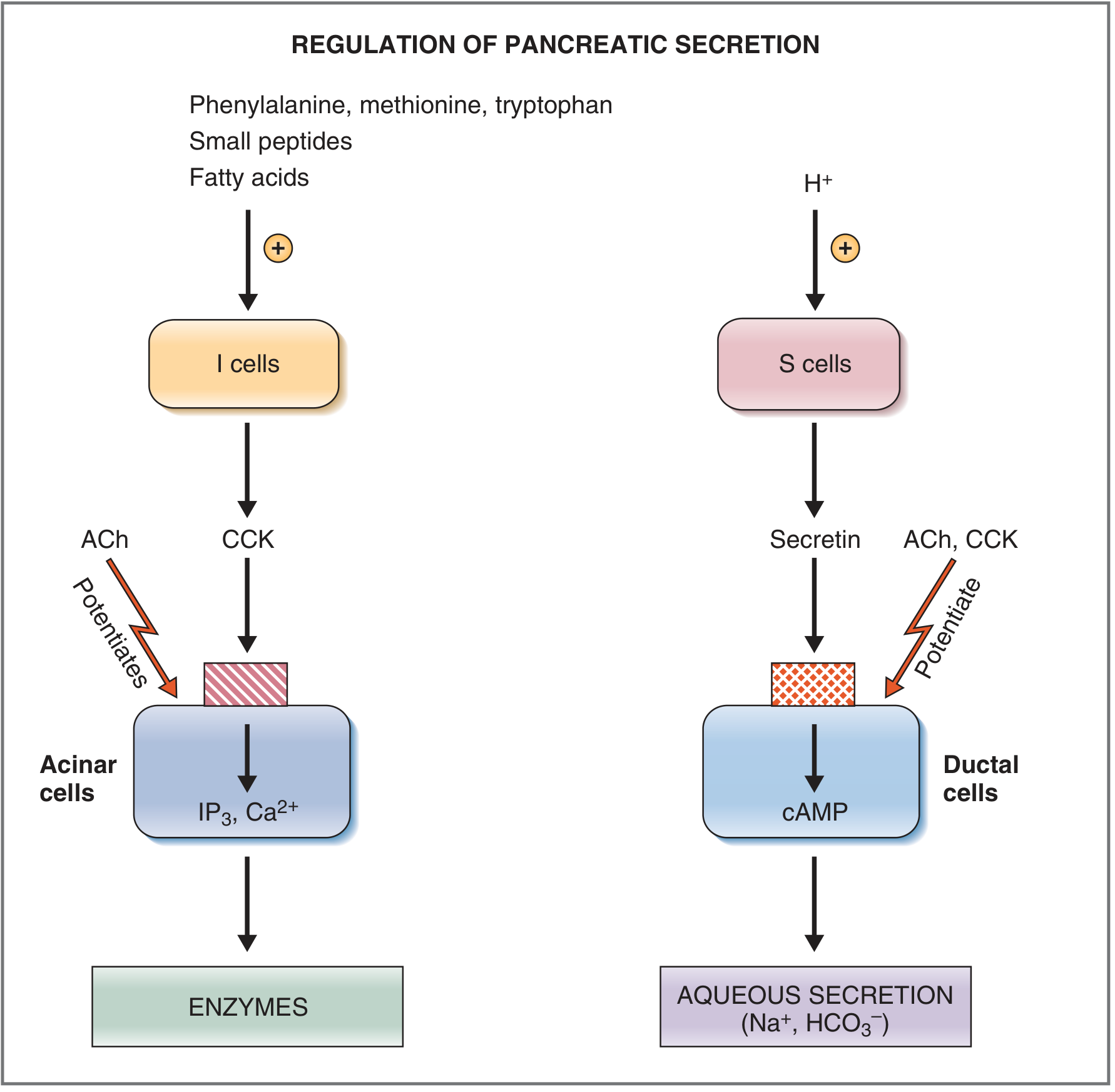
| Acetylcholine (ACh) | Vagus nerve / enteric nervous system | Acinar cells | Enzyme secretion | IP3 / Ca2+ |
| CCK | I cells of duodenum/jejunum | Acinar cells | Enzyme secretion (major) | IP3 / Ca2+ |
| Secretin | S cells of duodenum/jejunum | Ductal cells | HCO3- + water (aqueous) | cAMP |
Phases of Secretion
1. Cephalic Phase (~20% of enzyme secretion)
- Triggered by: sight, smell, taste of food, and conditioned reflex
- Mediated by: vagus nerve (ACh release)
- Effect: moderate enzyme secretion into acini; little fluid flow to duodenum (low water/electrolyte component)
2. Gastric Phase (~5-10% of enzyme secretion)
- Triggered by: gastric distension
- Mediated by: vagovagal reflexes
- Effect: further enzyme secretion, still small aqueous component
3. Intestinal Phase (~70-80% of total secretion - MOST IMPORTANT)
- Triggered by: chyme entering the duodenum
- Two separate arms:
- Stimulus: H+ in duodenum (pH < 4.5 to 5.0, maximal at pH 3.0)
- Source: S cells (duodenum/jejunum) release secretin (27 amino acid polypeptide)
- Action: secretin → cAMP in ductal cells → copious NaHCO3-rich juice (up to 145 mEq/L HCO3-)
- Also stimulates bile secretion
- Stimulus: amino acids, small peptides, fatty acids in duodenum
- Most potent amino acids: phenylalanine, methionine, tryptophan
- Source: I cells (duodenum/upper jejunum) release CCK (33 amino acid polypeptide)
- Action: CCK → IP3/Ca2+ in acinar cells → zymogen granule exocytosis → enzyme-rich juice
- Accounts for 70-80% of post-meal enzyme secretion
Inhibitors of Pancreatic Secretion
- Peptide YY (PYY): secreted by ileal endocrine cells when fat reaches the distal small intestine; signals end of intestinal phase
- Somatostatin: inhibits pancreatic secretion
- Sympathetic activity: inhibits secretion (parasympathetic stimulates it)
Clinical Correlations
- Acute pancreatitis: Premature activation of zymogens within the pancreas → autodigestion; plasma amylase and lipase rise markedly (used for diagnosis)
- Phospholipase A2 in pancreatitis: Activated prematurely in pancreatic ducts, hydrolyzes phosphatidylcholine from bile → lyso-PC → cell membrane damage and fat necrosis
- Carbonic anhydrase inhibitors (e.g., acetazolamide): Block HCO3- secretion, reducing pancreatic juice alkalinity
- Duodenal ulcer: Failure to neutralize gastric acid in the duodenum (inadequate secretin/bicarbonate response)
Draw a well labelled handwritten diagram of Gastro intestinal system
A well-labelled handwritten-style anatomical diagram of the human gastrointestinal system drawn on white paper with pencil/pen sketch aesthetic. Show the complete GI tract from mouth to anus in a frontal body outline. Label all major organs with handwritten annotation arrows: Mouth (oral cavity), Tongue, Salivary glands (parotid, submandibular, sublingual), Pharynx, Esophagus, Stomach (with fundus, body, pylorus labeled), Small intestine (Duodenum, Jejunum, Ileum), Large intestine (Cecum, Ascending colon, Transverse colon, Descending colon, Sigmoid colon, Rectum, Anal canal), Appendix, Liver, Gallbladder, Bile duct, Pancreas, Sphincter of Oddi. Include small inset boxes showing: gastric layers, villi of small intestine. Use neat handwritten annotation style with leader lines, pencil sketch shading, educational textbook appearance. Black ink on white background, clean medical illustration style resembling hand-drawn student notes.
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.
Draw a well labelled handwritten diagram of Gastro intestinal system
A well-labelled handwritten-style anatomical diagram of the human gastrointestinal system. Pencil and ink sketch on white paper, educational medical student notes aesthetic. Show the full GI tract inside a simple human torso outline. Label with handwritten arrow annotations: Mouth, Pharynx, Esophagus, Stomach (fundus, body, pylorus, pyloric sphincter), Duodenum, Jejunum, Ileum, Ileocecal valve, Cecum, Appendix, Ascending colon, Transverse colon, Descending colon, Sigmoid colon, Rectum, Anal canal. Also label accessory organs: Liver, Gallbladder, Common bile duct, Pancreas, Pancreatic duct. Hand-drawn leader lines with neat handwritten labels. Soft pencil shading on organs. Clean white background. Looks like a carefully drawn anatomy student diagram.
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.
Short note on classification of hormones.
Classification of Hormones
I. Classification by Chemical Structure
1. Peptide / Protein Hormones (most numerous class)
- Nature: Chains of amino acids ranging from small peptides (2-3 residues) to large glycoproteins
- Synthesis: Made on ribosomes as larger precursors (preprohormones → prohormones → active hormones), stored in secretory (zymogen) granules
- Solubility: Water-soluble (hydrophilic); cannot cross cell membranes
- Carrier proteins: Generally not required; circulate freely
- Half-life: Short (minutes)
| Gland/Tissue | Hormones |
|---|---|
| Hypothalamus | GnRH, CRH, GHRH, TRH, Somatostatin |
| Anterior pituitary | GH, TSH, ACTH, FSH, LH, Prolactin |
| Posterior pituitary | ADH (Vasopressin), Oxytocin |
| Pancreas | Insulin, Glucagon, Somatostatin |
| Parathyroid | PTH |
| Thyroid | Calcitonin |
| Heart | ANP (Atrial Natriuretic Peptide) |
| GI tract | Secretin, CCK, GLP-1, VIP |
2. Steroid Hormones
- Nature: Derived from cholesterol; have a characteristic four-ring (cyclopentanoperhydrophenanthrene) nucleus
- Synthesis: Not stored; synthesized on demand from cholesterol (in smooth ER and mitochondria); released by diffusion
- Solubility: Lipid-soluble (lipophilic); freely cross cell membranes
- Carrier proteins: Circulate bound to specific plasma proteins (e.g., CBG for cortisol, SHBG for sex hormones); this extends half-life significantly
- Half-life: Long (hours to days)
| Gland | Hormones |
|---|---|
| Adrenal cortex | Cortisol, Aldosterone, DHEA |
| Gonads (ovary) | Estradiol (E2), Progesterone |
| Gonads (testis) | Testosterone |
| Kidney/Skin | 1,25-dihydroxycholecalciferol (Vitamin D3) |
| Placenta | Estrogens, Progesterone, hCG |
3. Amine Hormones (Amino Acid-Derived)
a) Catecholamines (from Tyrosine)
- Epinephrine (Adrenaline) and Norepinephrine - adrenal medulla
- Dopamine - hypothalamus, brain
- Water-soluble, act on cell-surface receptors, short half-life
b) Thyroid Hormones (from Tyrosine + Iodine)
- T3 (Triiodothyronine) and T4 (Thyroxine)
- Unique: lipophilic despite amino acid origin (due to iodination)
- Circulate bound to TBG (thyroxine-binding globulin)
- Act like steroid hormones on nuclear receptors
- Long half-life: T4 = 7 days; T3 = 1 day
c) Indolamines (from Tryptophan)
- Serotonin (5-HT) - GI tract, pineal gland
- Melatonin - pineal gland
II. Classification by Mechanism of Action (Receptor Location)
| Class | Receptor Location | Second Messenger | Examples | Onset |
|---|---|---|---|---|
| Group I | Intracellular (cytosolic/nuclear) | None - direct gene regulation | Steroids, thyroid hormones, Vitamin D, retinoids | Slow (hours) |
| Group II | Cell membrane | cAMP, IP3/Ca2+, tyrosine kinase | Peptide hormones, catecholamines | Fast (minutes) |
Group I (Intracellular receptors - "SATIN" mnemonic):
- Hormone diffuses into cell → binds cytosolic/nuclear receptor → conformational change → hormone-receptor complex dimerizes → binds steroid-responsive elements (SREs) on DNA → mRNA transcription → new protein synthesis → physiologic effect
Group II (Membrane receptors):
| Second Messenger | Mediator | Examples |
|---|---|---|
| cAMP (via Gs → adenylyl cyclase) | PKA activation | Glucagon, ACTH, TSH, PTH, Secretin, ADH (V2) |
| IP3/Ca2+ (via Gq → phospholipase C) | PKC activation | GnRH, TRH, Oxytocin, CCK, ADH (V1) |
| Tyrosine kinase (receptor or JAK-STAT) | Phosphorylation cascades | Insulin, IGF-1, GH, Prolactin, Cytokines |
| cGMP | PKG activation | ANP, NO |
III. Classification by Mode of Delivery / Target Distance
| Type | Mode | Target | Example |
|---|---|---|---|
| Endocrine | Secreted into bloodstream | Distant cells | Insulin, cortisol |
| Paracrine | Acts on adjacent/neighboring cells | Local cells | Somatostatin (inhibits nearby islet cells) |
| Autocrine | Acts on the same cell that secreted it | Self-regulation | IGF-1 in some tissues |
| Neuroendocrine | Released from nerve terminals into blood | Distant cells | ADH, Oxytocin |
| Juxtacrine | Cell-to-cell contact via membrane-bound ligands | Adjacent cells | Notch signaling |
IV. Classification by Water Solubility
| Property | Water-Soluble Hormones | Lipid-Soluble Hormones |
|---|---|---|
| Examples | Peptides, catecholamines | Steroids, thyroid hormones |
| Carrier protein | Not needed | Required (e.g., TBG, CBG, SHBG) |
| Cell membrane crossing | Cannot cross - cell-surface receptor | Can cross - intracellular receptor |
| Onset of action | Fast (seconds-minutes) | Slow (hours) |
| Duration of action | Short | Long |
| Storage | Stored in granules | Not stored (synthesized on demand) |
Summary Comparison Table
| Feature | Peptide | Steroid | Thyroid | Catecholamines |
|---|---|---|---|---|
| Precursor | Amino acids | Cholesterol | Tyrosine + I | Tyrosine |
| Water solubility | High | Low | Low | High |
| Carrier protein | No | Yes | Yes | No |
| Receptor location | Cell surface | Intracellular | Intracellular | Cell surface |
| Second messenger | Yes | No | No | Yes |
| Action onset | Minutes | Hours | Hours-days | Seconds |
| Half-life | Short | Long | Long (T4: 7d) | Short |
| Gene expression change | No (primary) | Yes | Yes | No (primary) |