Morphological and radiological classification (rotteveel classification) of otosclerosis. MS ent university exam pattern for 10 marks.
Rotteveel classification otosclerosis morphological radiological CT scan
Rotteveel classification otosclerosis morphological radiological types
Morphological and Radiological (Rotteveel) Classification of Otosclerosis
Introduction (Brief)
PART 1: MORPHOLOGICAL CLASSIFICATION
A. Based on Site of Involvement
| Type | Description |
|---|---|
| Fenestral (Stapedial) | Most common (~80-85%). Foci at fissula ante fenestram, anterior oval window. Causes conductive hearing loss by fixing the stapes footplate |
| Retrofenestral (Cochlear) | Less common (~15%). Foci around otic capsule/cochlea. Causes sensorineural or mixed hearing loss |
| Combined | Both fenestral and retrofenestral involvement |
B. Based on Disease Phase (Histopathological)
- Resorption of dense enchondral bone by abnormal osteoclasts
- Replaced by vascular, sponge-like bone with wide marrow spaces
- Abundant blood vessels (Schwartze sign: flamingo pink blush through tympanic membrane)
- Seen as hypodensity on CT
- Osteoblasts deposit dense, lamellar sclerotic bone
- Hypercellular woven bone fills the marrow spaces
- Mosaic pattern of irregular cement lines (similar to Paget's disease but localized)
- Less vascular, seen as isodense or hyperdense on CT
C. Valvassori's Morphological Grading (Histological)
| Grade | Description |
|---|---|
| Grade 1 | Single foci, not involving oval window or cochlea |
| Grade 2 | Single or multiple foci involving oval window/cochlea |
| Grade 3 | Diffuse involvement |
PART 2: RADIOLOGICAL CLASSIFICATION - ROTTEVEEL CLASSIFICATION
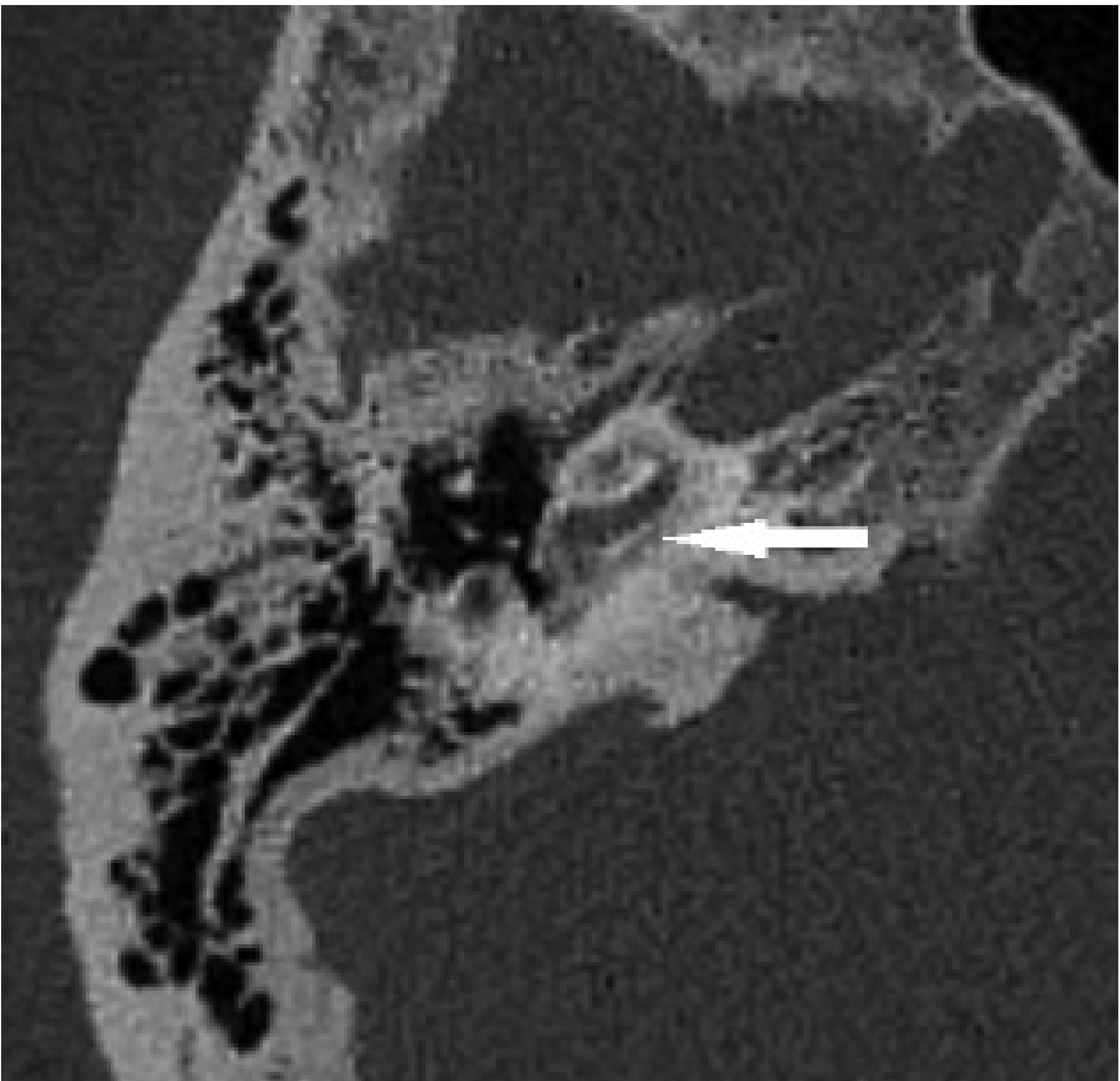
CT is the imaging modality of choice. Normal otic capsule appears uniformly dense. Otosclerotic foci appear as focal hypodensities (lucencies/plaques) in the active phase.
ROTTEVEEL CLASSIFICATION - COMPLETE TABLE
| Type | Description | CT Findings |
|---|---|---|
| Type 1 | Fenestral only | Thickened footplate (>0.6 mm) and/or narrowed or enlarged oval/round windows. Plaque at fissula ante fenestram |
| Type 2a | Retrofenestral - double ring effect | Halo of hypodensity surrounding the cochlea (the "double ring" or "halo sign") WITHOUT narrowing of basal turn |
| Type 2b | Retrofenestral - narrowed basal turn | Narrowing of the lumen of the basal turn of cochlea, WITHOUT the double ring sign |
| Type 2c | Retrofenestral - both | Double ring effect PLUS narrowing of basal turn. Most severe form of Type 2 |
| Type 3 | Severe retrofenestral | Such extensive involvement that the otic capsule is unrecognizable on CT. With or without fenestral involvement |
Explanation of Key CT Signs
- Earliest and most characteristic finding
- Small hypodense focus anterior to the oval window
- Pathognomonic of Type 1 disease
- Pericochlear hypodensity surrounds the dense cochlear endosteum
- Creates a "ring within a ring" appearance
- Represents active otospongiosis around the cochlea
- Also called "fourth ring of Valvassori" when seen around the full otic capsule
- Otosclerotic bone encroaches on the lumen of the basal cochlear turn
- Indicates significant cochlear involvement
- Relevant for cochlear implant electrode insertion
PART 3: COMPARISON WITH OTHER CT CLASSIFICATION SYSTEMS
| System | Basis | Types |
|---|---|---|
| Rotteveel | Type of lesion (double ring sign + basal turn narrowing) | Types 1, 2a, 2b, 2c, 3 |
| Symons/Fanning | Location of foci | Grade 1 (solely fenestral), Grade 2 (patchy cochlear), Grade 3 (diffuse cochlear) |
| Veillon | Extent and contact with cochlear endosteum | Types 1a, 1b, 2, 3, 4a, 4b |
| Valvassori (original) | Site and progression | Grades 1-3 |
PART 4: CLINICAL RELEVANCE OF ROTTEVEEL CLASSIFICATION
-
Type 1 (Fenestral only): Best prognosis. Managed with stapedotomy/stapedectomy. CT may not be mandatory but is useful to confirm diagnosis.
-
Type 2 (Retrofenestral): Mixed or sensorineural hearing loss. Type 2c has the poorest cochlear reserve. Important in counselling regarding degree of SNHL. May require cochlear implantation if stapedotomy fails.
-
Type 3 (Severe/Obliterative): Most challenging. Risk of incomplete electrode insertion during cochlear implantation. "Drillout" procedure may be needed. Worst audiological prognosis.
- Rotteveel Types 2 and 3 predict difficulties in cochlear implantation
- Narrowed basal turn (2b, 2c) may prevent full electrode array insertion
- Obliterative otosclerosis (Type 3) requires special surgical planning
SUMMARY MNEMONIC
- F = Fenestral only (Type 1)
- D = Double ring (Type 2a)
- N = Narrowed basal turn (Type 2b)
- B = Both double ring + narrowed basal turn (Type 2c)
- S = Severe - otic capsule unrecognizable (Type 3)
IMPORTANT POINTS FOR EXAM
- Rotteveel classification was published in Otology & Neurotology, 2004 (based on 53 cochlear implant patients)
- CT is the gold standard for imaging - high-resolution temporal bone CT (HRCT) at ≤0.5 mm slice thickness
- MRI (FLAIR/T2) shows endolymphatic hydrops in some cases but CT is preferred for bony detail
- The classification is not universally accepted - Symons/Fanning has higher inter/intraobserver reliability
- Active otosclerosis = hypodense on CT; inactive = isodense/hyperdense
- "Double ring sign" is essentially the fourth ring of Valvassori on CT
- Bilateral disease in up to 85% of cases
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2, p. 1235
- Cummings Otolaryngology Head and Neck Surgery, 7th Ed, Ch. 146
- Rotteveel LJ et al. Otol Neurotol 2004;25(6):943-52
- Imaging Studies in Otosclerosis: An Up-to-date Comprehensive Review, PMC8096512
Thyroid autoantibodies. Ms ent university exam pattern for 10 marks.
thyroid autoantibodies TPO TgAb TRAb types mechanisms clinical significance ENT
Thyroid Autoantibodies
INTRODUCTION
- Thyroid Peroxidase (TPO)
- Thyroglobulin (Tg)
- TSH Receptor (TSHR)
PART 1: ANTI-THYROID PEROXIDASE ANTIBODIES (TPOAb / Anti-TPO)
Antigen
- Oxidation of iodide on tyrosine residues in thyroglobulin
- Organification of iodine
- Coupling of iodotyrosines to form T3 and T4
Mechanism of Damage
- TPOAb activate complement via the classical pathway
- Complement-mediated cytotoxicity destroys thyrocytes
- Also involves antibody-dependent cell-mediated cytotoxicity (ADCC)
- Considered a pathogenic antibody (unlike TgAb which is mostly a disease marker)
Clinical Significance / Prevalence
| Disease | Prevalence of TPOAb |
|---|---|
| Hashimoto's (autoimmune) thyroiditis | >95% (most sensitive marker) |
| Graves' disease | >80% |
| General population (false positive) | 10-15% |
| Postpartum thyroiditis | ~80% |
Clinical Uses
- Diagnosis of Hashimoto's thyroiditis - most sensitive screening test
- Risk stratification - positive TPOAb in a euthyroid patient predicts ~2-4% annual risk of progression to hypothyroidism
- Postpartum thyroiditis prediction - TPOAb-positive women in first trimester have 30-50% risk
- Subclinical hypothyroidism - guides decision to treat (treatment recommended if TPOAb positive)
- Hashimoto's encephalopathy - diagnosis requires elevated TPOAb
- Infertility/recurrent miscarriage - associated with thyroid autoimmunity
- Serial measurement has little clinical value - treatment targets the dysfunction, not the autoimmune process
Normal Values
- >25 IU/mL is considered significant (Bailey and Love)
- Assay results from different laboratories cannot be directly compared (lack of standardization)
PART 2: ANTI-THYROGLOBULIN ANTIBODIES (TgAb / Anti-Tg)
Antigen
Mechanism
- TgAb binds thyroglobulin but is considered largely passive (not directly cytotoxic)
- Acts mainly as a disease marker rather than a pathogenic antibody
- T cells sensitized to Tg play a larger role in tissue destruction
Clinical Significance / Prevalence
| Disease | Prevalence of TgAb |
|---|---|
| Hashimoto's thyroiditis | 60-85% |
| Graves' disease | 50-60% |
| Differentiated thyroid cancer (DTC) | 10-15% |
| General population | 3-18% |
Clinical Uses
- Diagnosis of Hashimoto's thyroiditis - lower sensitivity than TPOAb; often ordered together
- Critical use: interference detection in Tg immunoassay
- TgAb competes with assay antibodies, causing falsely LOW serum Tg in immunometric assays (IMA)
- Can cause falsely HIGH Tg in radioimmunoassay (RIA)
- This interference is the most important practical reason for always measuring TgAb alongside Tg
- Thyroid cancer surveillance - TgAb is mandatory when monitoring post-thyroidectomy Tg levels in DTC. A rising TgAb titre may itself indicate disease recurrence even when Tg is undetectable
- Significant titre: >1:100 (Bailey and Love)
Key Point for ENT:
- Tg is the most sensitive tumour marker - detects residual/recurrent disease
- TgAb must always be checked simultaneously - its presence renders Tg unreliable
- A rising TgAb is itself a surrogate marker of recurrence
PART 3: TSH RECEPTOR ANTIBODIES (TRAb / TSH-RAb)
Antigen
Subtypes - The 3 Classes of TRAb
| Class | Old Name | Action | Effect | Disease |
|---|---|---|---|---|
| Thyroid Stimulating Immunoglobulin (TSI) | LATS (Long-Acting Thyroid Stimulator) | Mimics TSH - binds and activates TSHR | Hyperthyroidism | Graves' disease |
| TSH-Binding Inhibitory Immunoglobulin (TBII) - Blocking type | TBAb | Blocks TSH binding without activation | Hypothyroidism | Hashimoto's (8%), neonatal hypothyroidism |
| Neutral/Apoptotic TRAb | - | Binds TSHR, induces thyrocyte apoptosis | Hypothyroidism or euthyroid | Some cases of AITD |
All three subtypes may coexist and can switch over time ("class switching"), which complicates management.
Detection Methods (Generations of TRAb Assay)
| Generation | Method | Detection Limit | Notes |
|---|---|---|---|
| 1st generation | TBII: radiolabelled TSH competition with detergent-solubilized TSHR | ~2 IU/L | Cannot distinguish stimulating from blocking |
| 2nd generation | Automated: immobilized TSHR + chemiluminescent TSH | ~1 IU/L | Improved sensitivity, automation |
| 3rd generation | High-affinity monoclonal Ab (M22) instead of TSH | ~0.4 IU/L | Most sensitive; still cannot distinguish subtypes |
| Cell-based bioassays | cAMP generation assay (TSI-specific) | Highly sensitive | Can distinguish stimulating from blocking; not widely available |
Clinical Significance / Prevalence
| Disease | Prevalence of TRAb |
|---|---|
| Graves' disease | >90-98% (virtually diagnostic) |
| Hashimoto's thyroiditis (blocking type) | 0-20% |
| Neonatal Graves' (maternal transfer) | As per maternal level |
Clinical Uses
- Diagnosis of Graves' disease - unparalleled diagnostic accuracy (>98% sensitivity); most specific test
- Distinguishing Graves' from other causes of thyrotoxicosis (toxic nodular goitre, thyroiditis)
- Monitoring antithyroid drug (ATD) therapy - TRAb level at time of ATD withdrawal predicts relapse; high levels = likely relapse
- Prediction of neonatal thyrotoxicosis - maternal TRAb (IgG) crosses the placenta freely; measured at 28-36 weeks gestation; guides neonatal monitoring
- Prediction of neonatal hypothyroidism - maternal blocking antibodies (TBAb) can cause transient neonatal hypothyroidism
- "Class switching" - patients can switch from stimulating to blocking antibodies, converting Graves' hyperthyroidism to hypothyroidism; TRAb monitoring anticipates this
- Graves' orbitopathy (GO) - TRAb correlates with severity; high levels before radioiodine therapy predict worsening of GO
- Cost-effective diagnosis - TRAb measurement for Graves' disease is more cost-effective and faster than radioactive iodine uptake (RAIU) scan
PART 4: COMPREHENSIVE COMPARISON TABLE
| Feature | Anti-TPO (TPOAb) | Anti-Tg (TgAb) | Anti-TSHR (TRAb) |
|---|---|---|---|
| Antigen | Thyroid Peroxidase | Thyroglobulin | TSH Receptor |
| Immunoglobulin class | IgG | IgG | IgG |
| Action | Cytotoxic (complement activation) | Passive (marker) | Stimulatory / Blocking / Apoptotic |
| Hashimoto's prevalence | >95% | 60-85% | 0-20% (blocking) |
| Graves' prevalence | >80% | 50-60% | >90-98% |
| Normal population | 10-15% | 3-18% | <1% |
| Primary clinical use | Diagnosis of AITD; hypothyroidism risk | Tg assay interference; cancer surveillance | Diagnosis of Graves' disease |
| Crosses placenta? | IgG - yes | IgG - yes | IgG - yes (clinically significant) |
| Significant titre | >25 IU/mL | >1:100 | Any detectable level in clinical context |
PART 5: MINOR / EMERGING THYROID AUTOANTIBODIES
| Antibody | Target | Significance |
|---|---|---|
| Anti-NIS (Sodium Iodide Symporter) | NIS transporter | Present in ~25% AITD; no established diagnostic role |
| Anti-T4 antibodies | Thyroxine itself | Rare; causes falsely HIGH fT4 in 1-step competitive assays |
| Anti-T3 antibodies | Triiodothyronine | Similar interference as anti-T4 |
| Anti-megalin antibodies | Megalin (endocytic receptor) | Under investigation |
| Anti-pendrin antibodies | Pendrin (iodide transporter) | Described but no diagnostic role yet |
PART 6: ENT-SPECIFIC CLINICAL CONTEXTS
- Thyroid goitre workup - TPOAb and TgAb to distinguish Hashimoto's from simple/multinodular goitre
- Post-thyroidectomy for well-differentiated thyroid cancer - TgAb is mandatory alongside Tg surveillance
- Graves' disease with ophthalmopathy - TRAb correlates with activity of Graves' orbitopathy; high TRAb before radioiodine predicts worsening
- Recurrent laryngeal nerve palsy in Hashimoto's - rare but reported association
- Preoperative assessment - knowing TRAb status helps predict intraoperative bleeding (hypervascular Graves' gland) and postoperative neonatal risk in pregnant patients
- Thyroid cancer recurrence monitoring - TgAb interference must always be considered; rising TgAb = red flag for recurrence even with undetectable Tg
SUMMARY MNEMONIC
KEY EXAM POINTS
- TPOAb is the most sensitive test for Hashimoto's thyroiditis (>95%)
- TRAb is the most specific test for Graves' disease (>90%)
- TgAb's most important ENT/surgical use is detecting interference in Tg assay used for thyroid cancer surveillance
- TRAb crosses the placenta - can cause neonatal thyrotoxicosis (stimulating) or neonatal hypothyroidism (blocking)
- Falling TRAb levels during ATD treatment = good prognostic sign; persistently elevated = predict relapse
- In subclinical hypothyroidism: TPOAb positivity is the key indication to start thyroxine therapy (even at mildly elevated TSH levels)
- A histologically normal-looking thyroid can still have significant autoantibodies (seronegative AITD exists)
- Tietz Textbook of Laboratory Medicine, 7th Ed, Chapter 57 (Tables 57.7)
- Bailey and Love's Short Practice of Surgery, 28th Ed, p. 874
- Sabiston Textbook of Surgery, p. 1492
- Medscape: Thyroid Autoantibodies (TPOAb, TgAb and TRAb), Thyroid 2003;13(1)
Gelle test and bing test. Ms ent University exam pattern for 10 marks.
Gelle test Bing test tuning fork hearing ENT clinical significance procedure
Gelle test procedure positive negative result otosclerosis stapes fixation clinical significance
Gelle test procedure Politzer bag air pressure tuning fork positive negative interpretation hearing
Gelle test Bing test procedure interpretation significance
Gelle Test and Bing Test
INTRODUCTION
PART 1: GELLE'S TEST
History
Physiological Basis / Principle
- The tympanic membrane (TM) is pushed inward (medially)
- This displaces the ossicular chain inward
- The stapes footplate is pushed into the oval window
- This raises intralabyrinthine (perilymphatic) pressure
- Increased perilymph pressure causes stiffening/immobility of the basilar membrane
- A stiff basilar membrane is less responsive to vibration
- Therefore, hearing decreases (bone-conducted sound is perceived as softer)
Equipment Required
- Vibrating tuning fork (512 Hz preferred) placed on the mastoid process
- Siegle's pneumatic speculum (or a Politzer bag + airtight speculum) - to create positive and negative pressure changes in the sealed EAC
Siegle's speculum consists of a conical ear speculum with a magnifying glass at one end and a rubber tube attached to a rubber bulb - allowing visual inspection of the TM while simultaneously varying EAC pressure.
Procedure
- Strike the tuning fork and place its stem firmly on the mastoid process of the patient
- Insert the Siegle's speculum into the EAC, creating an airtight seal
- Alternately compress and release the rubber bulb to increase and decrease EAC air pressure
- Ask the patient: "Does the sound you hear become louder and softer as I compress and release?"
Interpretation
| Result | Finding | Cause |
|---|---|---|
| Positive Gelle | Loudness of bone-conducted sound fluctuates (louder when pressure released, softer when increased) | Normal hearing OR Sensorineural hearing loss (ossicular chain is mobile) |
| Negative Gelle | No change in loudness with pressure variation | Conductive hearing loss with ossicular fixation - classically otosclerosis |
Clinical Significance
-
Otosclerosis (most important):
- Stapes is fixed to the oval window by abnormal bone
- Pressure changes cannot be transmitted to the inner ear through the immobile ossicular chain
- Result: Negative Gelle - pathognomonic of stapes fixation
-
Ossicular discontinuity:
- If ossicular chain is broken/disarticulated, pressure changes also fail to reach the inner ear
- Result: Also gives a Negative Gelle
- Clinically distinguishing ossicular fixation from discontinuity requires other tests (e.g., tympanometry - Type Ad in discontinuity vs. Type As in fixation)
-
Normal and SNHL patients:
- Ossicular chain is intact and mobile
- Result: Positive Gelle
-
Modern replacement:
- Gelle's test has been largely replaced by tympanometry in modern practice
- Tympanometry provides more objective, quantitative data:
- Type As (shallow/stiff peak) = stapes fixation (otosclerosis)
- Type Ad (deep/flaccid peak) = ossicular discontinuity
- Type B (flat) = middle ear effusion
Summary Table - Gelle Test
| Condition | Gelle Result |
|---|---|
| Normal | Positive (fluctuates) |
| SNHL | Positive (fluctuates) |
| Otosclerosis (stapes fixation) | Negative |
| Ossicular discontinuity | Negative |
| Middle ear effusion | Negative (variation) |
PART 2: BING TEST
History
Physiological Basis / Principle - The Occlusion Effect
- When the external ear canal is occluded (blocked), bone-conducted sound is perceived as louder
- This occurs because:
- In an open EAC, low-frequency vibrations transmitted via bone conduction cause the walls of the EAC and the residual air column to vibrate in phase with the TM, and some sound energy is radiated/dissipated out of the open EAC
- When the EAC is occluded, this "sound leakage" is prevented
- The trapped air column in the sealed EAC now vibrates and adds to the mechanical energy reaching the TM and ossicles
- This results in enhancement of bone-conducted sound (by ~20 dB at low frequencies)
Equipment Required
- Vibrating tuning fork (256 or 512 Hz)
- Examiner's finger (to occlude/open the EAC) - simple and readily available
Procedure
- Strike the tuning fork and place its stem on the mastoid process behind the ear
- While the patient listens to the bone-conducted tone, the examiner alternately:
- Occludes the EAC by pressing the tragus inward (or placing a fingertip at the opening)
- Opens the EAC by releasing
- Ask the patient: "Does the sound change when I press on the ear?"
- Alternatively: ask if tone is louder with ear closed or open
Interpretation
| Result | Finding | Mechanism | Condition |
|---|---|---|---|
| Positive Bing | Tone becomes louder when EAC is occluded | Occlusion effect present - ossicular chain is mobile | Normal hearing OR Sensorineural hearing loss |
| Negative Bing | No change in loudness with occlusion | Occlusion effect absent - ossicular chain has conductive pathology | Conductive hearing loss |
Clinical Significance
-
Conductive hearing loss:
- In CHL, the middle ear mechanism is already compromised (e.g., fluid, ossicular fixation, perforated TM)
- The "extra" energy from EAC occlusion cannot be effectively transmitted through the diseased middle ear
- Negative Bing = CHL present
-
Sensorineural hearing loss:
- Middle ear is structurally normal; the problem lies in the cochlea or beyond
- Ossicular chain is intact and mobile
- Occlusion effect is preserved
- Positive Bing = SNHL (important distinguishing point - same result as normal)
-
Otosclerosis:
- Fixed stapes → no occlusion effect
- Negative Bing
-
Clinical utility:
- Helps differentiate CHL from SNHL when combined with Weber and Rinne
- Particularly useful in patients with unilateral deafness to determine the type
- Simpler than Gelle test - no equipment needed beyond a tuning fork and finger
Summary Table - Bing Test
| Condition | Bing Result |
|---|---|
| Normal hearing | Positive (louder when occluded) |
| SNHL | Positive (louder when occluded) |
| CHL (any cause) | Negative (no change) |
| Otosclerosis | Negative |
| Otitis media with effusion | Negative |
PART 3: COMPARISON OF GELLE AND BING TESTS
| Feature | Gelle Test | Bing Test |
|---|---|---|
| Described by | Marie-Ernest Gelle (1881) | Albert Bing (1891) |
| Principle | Effect of EAC air pressure on bone-conducted hearing | Occlusion effect on bone-conducted hearing |
| Mechanism tested | Mobility of ossicular chain under pressure | Presence of occlusion effect (middle ear integrity) |
| Equipment needed | Tuning fork + Siegle's speculum | Tuning fork + finger (simple) |
| Positive result | Fluctuation in loudness (normal/SNHL) | Louder when occluded (normal/SNHL) |
| Negative result | No change (ossicular fixation) | No change (CHL) |
| Specific for | Stapes fixation (otosclerosis) - most specific | Any type of CHL |
| Modern equivalent | Tympanometry (Type As = stapes fixation) | Impedance audiometry |
| Current use | Largely replaced by tympanometry | Limited clinical use; mainly historical/teaching |
PART 4: COMPLETE TUNING FORK TEST BATTERY (CONTEXT)
| Test | Normal | CHL | SNHL |
|---|---|---|---|
| Weber | Midline | Lateralizes to poorer ear | Lateralizes to better ear |
| Rinne | Positive (AC > BC) | Negative (BC > AC) | Positive (AC > BC) - "false positive" if severe |
| Bing | Positive (louder when occluded) | Negative (no change) | Positive (louder when occluded) |
| Gelle | Positive (fluctuates) | Negative if ossicles fixed | Positive (fluctuates) |
| Schwabach | Normal (equal to examiner) | Prolonged (patient hears longer) | Diminished (patient hears shorter) |
PART 5: SPECIFIC OTOSCLEROSIS BATTERY
| Test | Expected Finding | Reason |
|---|---|---|
| Weber | Lateralizes to worse ear | CHL in affected ear |
| Rinne | Negative (BC > AC) | CHL due to stapes fixation |
| Bing | Negative | No occlusion effect - fixed stapes |
| Gelle | Negative | No pressure transmission - fixed stapes |
| Schwabach | Prolonged | CHL prolongs perceived bone conduction |
| Tympanometry | Type As | Reduced compliance - stiffened ossicular chain |
| Audiogram | CHL with Carhart notch at 2 kHz | Mechanical resonance loss |
KEY EXAM POINTS
- Both Gelle and Bing are bone conduction tests
- Gelle uses pressure change (Siegle's speculum); Bing uses canal occlusion (finger)
- Both are negative in CHL, specifically stapes fixation/otosclerosis
- Both are positive in SNHL (ossicular chain mobile) - this distinguishes them from Rinne
- The Bing test detects the occlusion effect; absent occlusion effect = CHL
- The Gelle test is the most specific test for stapes fixation among tuning fork tests
- Gelle is now replaced by tympanometry (Type As); Bing is replaced by impedance audiometry
- Negative Gelle + Negative Rinne + Weber lateralizing to bad ear = classic otosclerosis tuning fork pattern
- A Negative Gelle with ossicular discontinuity also occurs - differentiated by tympanometry (Type Ad vs. Type As)
- Tuning fork frequency: 512 Hz preferred for Rinne and Bing; Gelle can use 512 Hz
- KJ Lee's Essential Otolaryngology, 11th Ed, Table 14-5 (Tuning Fork Tests), p. 293-294
- Cummings Otolaryngology Head and Neck Surgery, 7th Ed
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
- Epomedicine: Hearing Tests with Tuning Fork
- LITFL Eponymictionary: Tuning Fork Tests (Albert Bing, 1891)
A/N ratio for adenoid assessment with respect to obstructive sleep apnea. Ms ent University exam format for 10 marks.
AN ratio adenoid nasopharyngeal ratio measurement lateral neck X-ray obstructive sleep apnea children
Cohen Konak AN ratio adenoid measurement method grading lateral radiograph OSA significance 0.8
AN ratio Fujioka 1979 adenoid nasopharyngeal measurement technique grading 0.8 0.6 OSA pediatric adenotonsillectomy
AN ratio adenoid nasopharyngeal measurement technique landmark grading OSA significance
AN ratio grading Fujioka method measurement adenoid OSA lateral radiograph
A/N Ratio for Adenoid Assessment in Obstructive Sleep Apnea
INTRODUCTION
- Confirming the diagnosis of AH
- Correlating adenoid size with severity of OSA
- Planning adenoidectomy / adenotonsillectomy (AT)
- Monitoring response to treatment (e.g., intranasal steroids)
PART 1: HISTORICAL BACKGROUND
- First described by Fujioka et al. in 1979 (American Journal of Roentgenology)
- Fujioka studied 1,398 infants and children with lateral skull radiographs
- Introduced the A/N ratio as a reliable method to express adenoid size and patency of the nasopharyngeal airway
- Established the landmark threshold: A/N ratio >0.80 = enlarged adenoids
- Found that an A/N ratio >0.80 was present in 34 of 36 patients (94%) subjectively judged to have enlarged adenoids by experienced observers
- Prior to Fujioka, Linder-Aronson had used a similar ratio as a parameter in symptomatic adenoid hypertrophy
PART 2: ANATOMY OF THE NASOPHARYNX (RELEVANT TO MEASUREMENT)
- Basiocciput (clivus): The sloping bone forming the posterior wall of the nasopharynx; the adenoid pad lies along its anterior surface
- Sphenobasioccipital synchondrosis (SBS): The junction between the sphenoid and occipital bones at the skull base; the anteroinferior edge serves as the superior landmark for nasopharyngeal depth
- Hard palate (posterior nasal spine / PNS): The inferior landmark for nasopharyngeal depth
- Adenoid shadow: The soft tissue mass along the posterior wall; the point of maximal convexity is used for measurement
- Pterygoid plates: Alternative inferior reference point in some methods
PART 3: THE A/N RATIO - MEASUREMENT TECHNIQUE
Radiographic Requirements
- Lateral soft-tissue radiograph of the nasopharynx (lateral neck X-ray)
- Patient position: Erect, head in true lateral position, mouth closed, neck slightly extended (standard "sniffing" or neutral position)
- Taken during inspiration (to visualize the nasopharyngeal airway at its maximum)
- Focus-film distance: 100 cm
- Exposure: ~65 kV, 200 mA (low-dose technique)
- Timing: NOT during crying or swallowing (these alter adenoid position and nasopharyngeal dimensions)
Measurement Points (Fujioka Method)
Sphenobasioccipital
Synchondrosis (SBS)
↑
___________│____________
| Adenoid shadow |
| (A = maximal | ← Adenoid depth (A)
| convexity to | measured perpendicular
| clivus line) | to anterior margin of
|_______________________| basiocciput
↕
N = Posterior hard palate → Anteroinferior SBS
(Nasopharyngeal depth)
- The perpendicular distance from the point of maximal convexity of the adenoid shadow to a line drawn along the anterior margin of the basiocciput (clivus)
- The distance measured along a line from the posterior border of the hard palate (posterior nasal spine) to the anteroinferior edge of the sphenobasioccipital synchondrosis
- This line represents the full sagittal depth of the nasopharyngeal cavity
Formula
PART 4: GRADING OF ADENOID HYPERTROPHY BY A/N RATIO
Fujioka Grading (Original)
| Grade | A/N Ratio | Adenoid Size | Clinical Status |
|---|---|---|---|
| Grade I (Small) | 0.3 - 0.5 | Normal/small adenoid | No significant obstruction |
| Grade II (Medium) | 0.5 - 0.7 | Moderate enlargement | Borderline; may have mild symptoms |
| Grade III (Large) | > 0.7 | Significant hypertrophy | Symptomatic obstruction likely |
Key Threshold Values
| A/N Ratio | Significance |
|---|---|
| < 0.60 | Normal; unlikely significant obstruction |
| 0.60 - 0.70 | Borderline/mild hypertrophy |
| 0.70 - 0.80 | Moderate hypertrophy; probable obstruction |
| > 0.80 | Pathological adenoid hypertrophy (Fujioka's criterion - 94% PPV) |
| > 0.73 | Pathological criterion per Elwany |
| > 0.71 | Used by some authors (Mahboubi, Kemaloglu) |
Most widely used cut-off: A/N ratio > 0.8 = enlarged adenoids requiring treatment (Fujioka 1979)
PART 5: A/N RATIO AND OBSTRUCTIVE SLEEP APNEA (OSA)
Pathophysiology of OSA in Adenoid Hypertrophy
- Increased upper airway resistance → increased respiratory effort during sleep
- Partial obstruction → hypopneas, snoring, increased work of breathing
- Complete obstruction → obstructive apneas, oxygen desaturation
- Arousal response → sleep fragmentation, non-restorative sleep
- Chronic sequelae: cor pulmonale, pulmonary hypertension, growth retardation, neurocognitive deficits, adenoid facies
OSA Diagnostic Parameters
- Gold standard: Overnight polysomnography (PSG) - measures:
- Apnea-Hypopnea Index (AHI): Number of apneas + hypopneas per hour
- Minimum oxygen saturation (SpO₂ nadir)
- Arousal index
- AHI thresholds in children:
- Normal: AHI < 1/hour
- Mild OSA: AHI 1-5/hour
- Moderate OSA: AHI 5-10/hour
- Severe OSA: AHI > 10/hour
Correlation Between A/N Ratio and OSA Severity
| A/N Ratio | Predicted OSA Impact |
|---|---|
| < 0.6 | Minimal nasopharyngeal obstruction; OSA unlikely from adenoids alone |
| 0.6 - 0.7 | Mild-moderate nasopharyngeal narrowing |
| 0.7 - 0.8 | Moderate obstruction; risk of OSA increased |
| > 0.8 | High probability of significant OSA from adenoid obstruction; adenoidectomy indicated |
- Best correlations between A/N ratio and PSG parameters (OAHI and minimum SpO₂) were seen using the anterior airway measurement (Cohen method variant)
- The A/N ratio correlates significantly with OSA severity particularly in preschool children (age 3-6 years) - when the nasopharyngeal space is narrowest (narrowest at ~4.5 years) relative to adenoid size (peaks at 7-10 years)
- In school-age children, clinical symptoms may be more predictive than A/N ratio alone
- The nasopharynx is smallest relative to body size at age 3-6 years
- Adenoids grow rapidly in infants up to age 2 (filling half the nasopharynx)
- Adenoids reach maximum size at age 7-10 years
- Adenoids involute after puberty
- Therefore, A/N ratio is most clinically significant in ages 2-10 years
PART 6: COMPARISON WITH OTHER METHODS OF ADENOID ASSESSMENT
| Method | A/N Ratio (Fujioka) | Cohen-Konak Method | Flexible Nasopharyngoscopy (FNE) | Endoscopic Grading (Parikh) |
|---|---|---|---|---|
| Basis | Adenoid depth / Nasopharyngeal depth | Airway width / Soft palate width | Direct visualization | Degree of choanal obstruction |
| Landmarks | Clivus, posterior hard palate, SBS | Soft palate (1 cm below hard palate) | Posterior choanae | Choanal space |
| Grading | Grade I: <0.5; II: 0.5-0.7; III: >0.7 | Small/Medium/Large (Airway:SP ratio ≥1, 0.5-1, <0.5) | Grade 1-4 | Grade 1: <50%; Grade 2: 50-75%; Grade 3: >75% choanal obstruction |
| Sensitivity | 100% (excellent for ruling out) | 83.3% | High | Very high |
| Specificity | Lower | 75% (better for ruling in) | High | Highest |
| Correlation with DISE | r = 0.670 | r = 0.458 | N/A | Gold standard-like |
| Advantages | Simple, objective, reproducible, no patient cooperation needed | Widely used, simple | Direct visualization, no radiation | Most accurate grading |
| Disadvantages | Radiation, 2D only, affected by positioning | Radiation | Requires cooperation, gagging | Equipment-dependent, invasive |
| Current preference | Best screening tool | Complementary | Preferred initial assessment if cooperative | Preoperative planning |
Parikh Endoscopic Grading (for context)
- Grade 1: Adenoid tissue NOT in contact with adjacent structures
- Grade 2: Adenoid tissue in contact with torus tubarius (Eustachian tube cushion)
- Grade 3: Adenoid tissue in contact with vomer
- Grade 4: Adenoid tissue completely obstructs the choanae (some systems add Grade 4)
PART 7: FACTORS AFFECTING A/N RATIO ACCURACY
Technical Factors (Causes of Error)
-
Patient positioning:
- Head rotation → superimposition of structures → false measurement
- Neck flexion vs. extension alters nasopharyngeal dimensions (erect with slightly extended neck is standard)
-
Phase of respiration:
- Adenoid may appear larger during expiration
- Measurement should be during quiet inspiration
-
Crying or swallowing:
- Adenoid pad elevates during swallowing → falsely low A
- Must be avoided during imaging
-
Age and skull growth:
- Nasopharyngeal depth (N) increases with age
- Age-stratified reference ranges are important (A/N varies by age group)
-
2D limitation:
- Lateral X-ray provides only a sagittal view
- Does not assess lateral dimensions of adenoid or choanal width
-
Inter-observer variability:
- Inter-rater ICC >0.90 for Fujioka method (excellent)
- Some variation between junior and senior radiologists
-
Radiation exposure:
- A limitation especially with repeated studies; comparable in cost to FNE
PART 8: CLINICAL DECISION-MAKING USING A/N RATIO IN OSA
Child with suspected adenoid hypertrophy + OSA symptoms
(snoring, apneas, mouth breathing, daytime sleepiness)
↓
Lateral neck X-ray → A/N ratio
↓
┌───────────────┬──────────────────┐
A/N < 0.6 0.6-0.8 A/N > 0.8
Unlikely AH Borderline Probable AH
↓ ↓ ↓
Other causes FNE/Endoscopy Adenoidectomy
(obesity, + PSG indicated
TH, LPR) assessment (consider PSG
if doubt about
tonsils or
OSA severity)
Indications for Adenoidectomy (OSA context)
- A/N ratio > 0.8 with clinical symptoms of OSA
- A/N ratio > 0.7 with AHI > 5/hour on PSG
- Failing medical management (intranasal steroids, montelukast)
- Complications: cor pulmonale, failure to thrive, dental malocclusion, adenoid facies
Response to Treatment (monitoring with A/N ratio)
- Intranasal beclomethasone reduces adenoid/choanae ratio from 91% → 62% after 6 months
- Post-adenoidectomy A/N ratio should normalize to < 0.6
- Residual OSA after adenoidectomy is common in obese children and those with craniofacial abnormalities → reassess with PSG
PART 9: LIMITATIONS OF A/N RATIO IN OSA ASSESSMENT
- Correlates poorly with OSA in school-age children (>7 years) - clinical score and body weight become more important
- Does not account for tonsillar hypertrophy - combined adenotonsillar assessment required for complete OSA workup
- 2D measurement - does not assess lateral or circumferential obstruction
- No universal cut-off agreed upon - values range from 0.71 to 0.80 in different studies
- Radiation exposure - limits serial studies in young children
- Cannot replace PSG for definitive OSA diagnosis - A/N ratio reflects anatomy, not functional airway collapse
- A/N ratio is age-dependent - requires age-stratified interpretation
SUMMARY TABLE
| Parameter | Details |
|---|---|
| Full name | Adenoid-Nasopharyngeal (A/N) Ratio |
| Introduced by | Fujioka et al., 1979 |
| Imaging modality | Lateral soft-tissue X-ray of nasopharynx |
| Measurement A | Perpendicular distance from maximal adenoid convexity to anterior clivus line |
| Measurement N | Distance from posterior hard palate to anteroinferior edge of SBS |
| Formula | A ÷ N |
| Normal | < 0.6 |
| Borderline | 0.6 - 0.8 |
| Pathological | > 0.8 (Fujioka) / >0.73 (Elwany) |
| Grading | I (<0.5), II (0.5-0.7), III (>0.7) |
| Sensitivity | 100% |
| Best age for use | 2-10 years (especially 3-6 years for OSA correlation) |
| Modern replacement | Flexible nasopharyngoscopy + PSG |
| OSA gold standard | Polysomnography (AHI > 1/hour in children = abnormal) |
KEY EXAM POINTS
- A/N ratio was first described by Fujioka et al. (1979) - studied 1,398 children
- A/N ratio = Adenoid depth ÷ Nasopharyngeal depth on lateral neck X-ray
- A/N > 0.8 = pathological adenoid hypertrophy (94% PPV)
- Patient must be erect, true lateral, mouth closed, during quiet inspiration
- A/N ratio correlates best with OSA in preschool children (3-6 years); clinical score is better in school-age
- NOT a substitute for PSG - diagnoses anatomy, not functional obstruction
- Fujioka grading: Grade I <0.5, Grade II 0.5-0.7, Grade III >0.7
- Cohen-Konak method uses airway-to-soft-palate ratio; complementary - better specificity; Fujioka has better sensitivity
- Main limitation: 2D imaging, radiation, position-dependent, no tonsillar assessment
- Post-adenoidectomy: A/N should normalize; residual OSA in obese children requires follow-up PSG
- Fujioka M, Young LW, Girdany BR. Radiographic evaluation of adenoidal size in children: adenoidal-nasopharyngeal ratio. AJR Am J Roentgenol. 1979;133(3):401-404. (PMID: 111497)
- Parikh SR et al. Validation of a new grading system for endoscopic examination of adenoid hypertrophy. Otolaryngol Head Neck Surg. 2006;135:684-687
- Assessing pediatric adenoid hypertrophy: reliability of radiographic vs. endoscopic techniques. PMC12990599
- A New Clinical Scoring System for Adenoid Hypertrophy in Children. PMC4344975
- Pediatric Obstructive Sleep Apnea Syndrome. Children's Hospital Boston