Edematous Gall bladder with no sign of stone on ultrasound
Reading File
Finding Sources
Finding Sources
Searching the Web
acalculous cholecystitis edematous gallbladder ultrasound diagnosis management
Reading File
Reading File
Reading File
Searching Images
acalculous cholecystitis ultrasound gallbladder wall thickening edema
Loading Image
Loading Image
Here is a comprehensive clinical overview:
Edematous Gallbladder Without Stones — Acute Acalculous Cholecystitis (AAC)
An edematous, thickened gallbladder wall with no calculi on ultrasound is the hallmark imaging presentation of Acute Acalculous Cholecystitis (AAC) — inflammation of the gallbladder in the absence of gallstones.
Ultrasound Findings
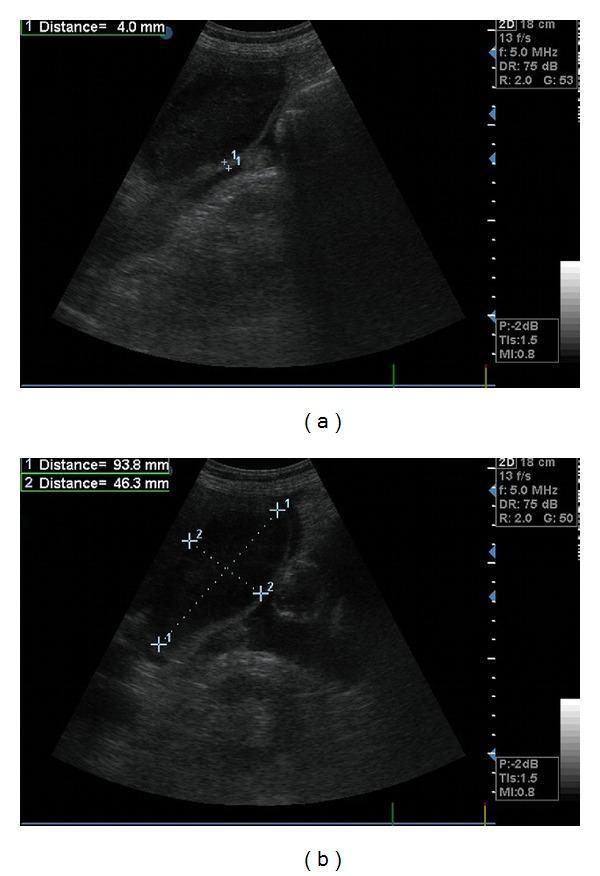
Major US criteria (two required for diagnosis):
- Gallbladder wall thickness > 3 mm (often 4–6+ mm in AAC)
- Pericholecystic fluid (hypoechoic rim around wall)
- Positive sonographic Murphy sign (tenderness directly over GB with probe)
- Intramural gas (emphysematous cholecystitis variant)
Minor US criteria:
- Gallbladder distension (long axis > 8 cm, short axis > 4 cm)
- Biliary sludge
- Sloughed mucosal membrane
Diagnosis requires 2 major criteria, OR 1 major + 2 minor criteria.
Who Gets It?
AAC is predominantly a disease of critically ill patients. Risk factors include:
- ICU patients on prolonged fasting or total parenteral nutrition (TPN)
- Major surgery, severe burns, polytrauma
- Sepsis / multi-organ failure
- Prolonged mechanical ventilation
- Immunocompromised states (HIV/AIDS, transplant, hematologic malignancy)
- Infections: Salmonella, Shigella, Leptospira, CMV, Cryptosporidium, Candida
- Vasculitides: SLE, polyarteritis nodosa, Kawasaki disease, HSP
Pathogenesis: Bile stasis + gallbladder ischemia → mucosal damage → edema of the serosa and muscular layers with patchy arteriolar/venular thrombosis → risk of gangrene, empyema, and perforation.
(Schwartz's Principles of Surgery, 11th ed.)
Clinical Features
| Feature | Detail |
|---|---|
| Pain | RUQ or epigastric, may be masked in sedated/ICU patients |
| Fever | Common; may be the only sign in obtunded patients |
| Murphy's sign | Positive on physical exam or sonography |
| Jaundice | Occasional |
| Leukocytosis | Typical; WBC elevated |
| LFTs | ↑ Alkaline phosphatase, ↑ direct bilirubin common |
Differential Diagnosis for Edematous GB Without Stones
| Condition | Key Feature |
|---|---|
| Acute acalculous cholecystitis | Critically ill, fever, leukocytosis, positive Murphy sign |
| Acute hydrops of GB | Non-inflammatory distension; sterile bile; associated with Kawasaki, HSP, scarlet fever; usually benign |
| Hypoalbuminemia / ascites | GB wall thickening without tenderness or fever (systemic cause) |
| Congestive heart failure / hepatitis | Diffuse wall thickening from portal hypertension or systemic edema |
| Primary sclerosing cholangitis | Thickening + ductal involvement |
| GB carcinoma / adenomyomatosis | Focal thickening, asymmetric |
In a patient who is not critically ill and has no systemic cause of edema, consider acalculous cholecystitis triggered by infection (Salmonella, viral hepatitis, parasites).
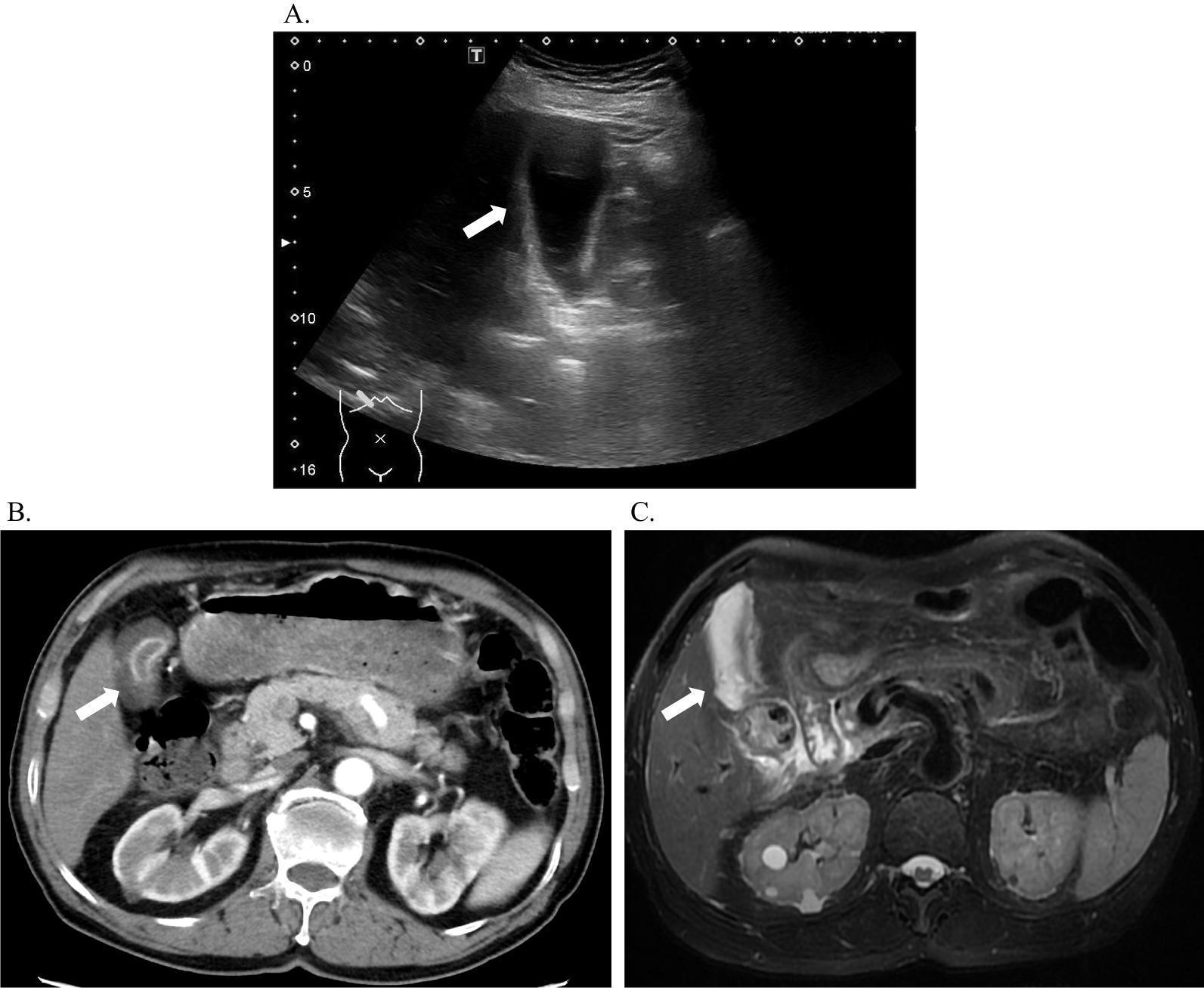
Further Investigations
If USS is equivocal or acalculous cholecystitis is suspected:
- HIDA scan (cholescintigraphy) — most reliable test; non-visualization of gallbladder = positive. Can use CCK augmentation for chronic/functional cases.
- CT abdomen — confirms distension, wall thickening, pericholecystic fat stranding; better systemic assessment; can detect complications (perforation, abscess).
- MRI/MRCP — best soft-tissue characterization; T2 shows mural edema; rules out choledocholithiasis.
Management
Acute AAC
- Urgent intervention — rapid deterioration (gangrene, perforation) is a real risk.
- Broad-spectrum IV antibiotics + fluid resuscitation immediately.
- If surgically fit → Laparoscopic cholecystectomy (definitive; safe even in severe inflammation).
- If critically ill / unfit for surgery → Percutaneous cholecystostomy (drainage tube); ~90% improve. Interval cholecystectomy can follow recovery.
- Endoscopic gallbladder stenting (EUS-guided or ERCP) — for patients with end-stage liver disease where even percutaneous drainage is high-risk.
Acute Hydrops (non-inflammatory)
- Usually conservative — observation, treat the underlying cause (e.g., Kawasaki, infection).
- Most resolve spontaneously.
Morphology (Pathology)
"There are no specific morphologic differences between acute acalculous and calculous cholecystitis, save the absence of stones in the acalculous form." — Robbins & Cotran Pathologic Basis of Disease
Histology shows: edema of serosa + muscular layers, neutrophilic infiltration, patchy mucosal ulceration, and in severe cases — gangrenous necrosis.
Bottom line: An edematous gallbladder without stones = Acute Acalculous Cholecystitis until proven otherwise. Look for the clinical context (ICU, TPN, sepsis, trauma), confirm with HIDA if USS alone is inconclusive, and intervene urgently — cholecystectomy if fit, percutaneous cholecystostomy if not.
Sources: Schwartz's Principles of Surgery 11e; Sleisenger & Fordtran's GI and Liver Disease; Bailey & Love's Surgery 28e; Robbins & Cotran Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.