How to measure bp procedure
Reading File
Finding Sources
Searching the Web
blood pressure measurement procedure steps technique 2024
Reading File
Reading File
Reading File
Loading Image
Here is a complete, evidence-based guide to blood pressure (BP) measurement procedure, sourced from Harrison's Principles of Internal Medicine 22nd Edition (2025) and Brenner & Rector's The Kidney:
Blood Pressure Measurement Procedure
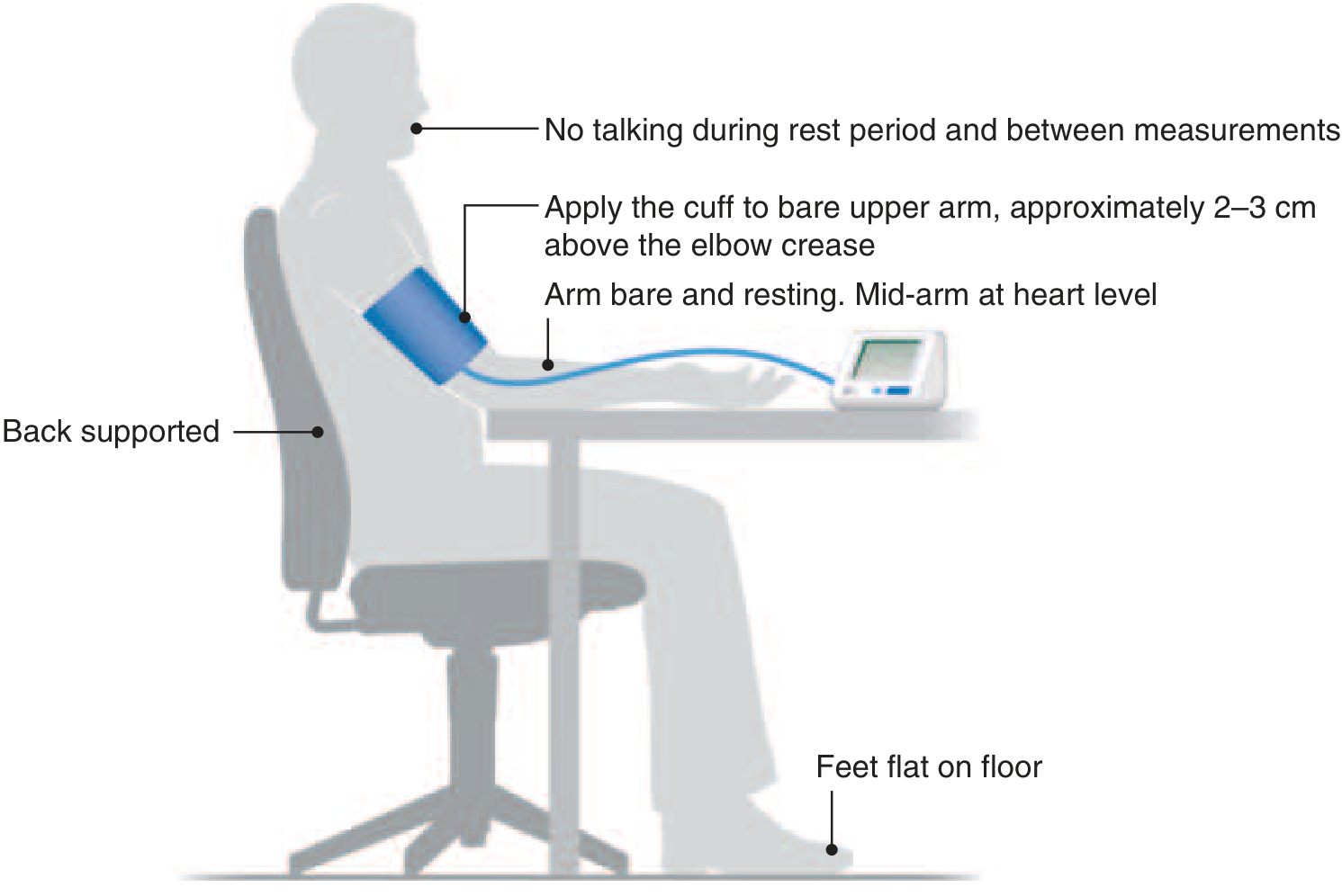
Correct positioning for office BP measurement (Harrison's, 22nd Ed.)
1. Patient Preparation (Before Measurement)
- Have the patient avoid caffeine, smoking, alcohol, and exercise for at least 30 minutes prior.
- Patient should have an empty bladder.
- Use a quiet room with a comfortable ambient temperature.
- Explain the procedure to the patient, including the number of readings.
- Allow the patient to rest quietly for 3-5 minutes before the first reading - no talking, no phone use during rest or measurement.
2. Positioning the Patient
- Seat the patient in a chair with upright back support.
- Feet should be flat on the floor (not crossed).
- The measurement arm should be comfortably supported on a surface.
- The cuff must be at heart level (mid-brachial level). If the arm hangs freely or is held up, readings will be falsely low or high.
3. Equipment Selection
- Use a clinically validated device - preferably an automated oscillometric device.
- Choose the correct cuff size for the patient's arm circumference. An undersized cuff gives falsely high readings; an oversized cuff gives falsely low readings.
- Aneroid and electronic oscillometric devices should be calibrated every 12 months.
| Cuff type | Indication |
|---|---|
| Standard adult | Most adults |
| Large adult | Obese arm |
| Thigh cuff | Upper extremity contraindications (in prone position) |
4. Cuff Application
- Apply the cuff to the bare upper arm (no clothing underneath).
- Position the cuff approximately 2-3 cm above the elbow crease (antecubital fossa).
- The cuff bladder should be centered over the brachial artery.
- Ensure the cuff fits snugly - you should be able to slip two fingers under it.
5. Auscultatory Method (Manual Sphygmomanometer)
This remains the standard manual technique, using Korotkoff sounds:
- Estimate systolic pressure first - palpate the radial pulse while inflating the cuff; note the pressure at which the pulse disappears. Add 30 mmHg to this value to set your inflation target (prevents auscultatory gap errors).
- Place the stethoscope over the brachial artery in the cubital fossa (do not tuck it under the cuff).
- Inflate the cuff to the estimated systolic pressure + 30 mmHg.
- Deflate slowly at ~2 mmHg/second.
- Systolic BP = pressure at which the first tapping sound (Korotkoff Phase I) is heard.
- Diastolic BP = pressure at which sounds disappear (Korotkoff Phase V).
- Deflate completely and record both values.
6. Recording and Averaging
- Take at least 2 readings, separated by 1-2 minutes, and record the average.
- At the first visit, measure BP in both arms; use the arm with the higher reading for all subsequent visits.
- A difference >10-15 mmHg between arms warrants investigation (e.g., subclavian stenosis).
- Use an average of two or more readings at two or more visits to estimate the patient's usual BP level.
7. Special Situations
Orthostatic BP measurement:
- Measure after the patient has been supine for 5 minutes.
- Repeat at 1 minute and 3 minutes after standing.
- A drop of ≥20 mmHg systolic or ≥10 mmHg diastolic = orthostatic hypotension.
White-coat effect:
- Some patients have elevated office BP but normal readings outside (white-coat hypertension).
- Automated multiple readings with the patient alone in the room help eliminate this effect.
- Ambulatory BP monitoring (ABPM) or home BP monitoring are superior for true BP burden assessment.
ACC/AHA BP Classification (Adults)
| Category | Systolic (mmHg) | Diastolic (mmHg) | |
|---|---|---|---|
| Normal | <120 | and | <80 |
| Elevated | 120-129 | and | <80 |
| Stage 1 Hypertension | 130-139 | or | 80-89 |
| Stage 2 Hypertension | ≥140 | or | ≥90 |
Source: Harrison's Principles of Internal Medicine, 22nd Ed., Table 288-1
Key Points to Avoid Errors
| Error | Effect on Reading |
|---|---|
| Cuff too small | Falsely HIGH |
| Arm below heart level | Falsely HIGH |
| Patient talking | Falsely HIGH |
| Cuff over clothing | Falsely HIGH |
| Back unsupported / legs crossed | Falsely HIGH |
| Deflating too fast | Underestimates systolic, overestimates diastolic |
- Harrison's Principles of Internal Medicine, 22nd Ed., pp. 288
- Brenner & Rector's The Kidney, Box 46.1
- Gray's Anatomy for Students
Create a quick reference checklist for BP measurement
Asking for Preferences
Here is your quick reference checklist:
✅ Blood Pressure Measurement - Quick Reference Checklist
🔲 BEFORE YOU START — Patient Preparation
- No caffeine, smoking, alcohol, or exercise for 30 min prior
- Bladder emptied
- Patient resting in quiet room for 3-5 minutes
- No talking or phone use during rest and measurement
- Explain the procedure to the patient
🔲 EQUIPMENT CHECK
- Validated BP device (automated oscillometric preferred)
- Correct cuff size selected for arm circumference
- Device calibrated (within last 12 months)
| Arm Circumference | Cuff Size |
|---|---|
| 22-26 cm | Small adult |
| 27-34 cm | Standard adult |
| 35-44 cm | Large adult |
| 45-52 cm | Adult thigh cuff |
🔲 PATIENT POSITIONING
- Seated in chair with back fully supported
- Feet flat on floor (not crossed)
- Bare arm resting on a flat surface
- Mid-arm (cuff) at heart level
🔲 CUFF APPLICATION
- Applied to bare skin (no sleeve underneath)
- Positioned 2-3 cm above elbow crease
- Bladder centred over brachial artery
- Snug fit (2 fingers slip underneath)
🔲 TAKING THE READING (Auscultatory Method)
- Estimate systolic first by palpating radial pulse while inflating
- Inflate to estimated systolic + 30 mmHg
- Stethoscope placed over brachial artery in cubital fossa
- Deflate slowly at ~2 mmHg/second
- Record systolic = first Korotkoff sound (Phase I)
- Record diastolic = sounds disappear (Phase V)
- Deflate cuff completely
🔲 RECORDING & AVERAGING
- Take ≥ 2 readings, 1-2 min apart
- Record the average of the readings
- At first visit: measure both arms; use the higher arm going forward
- Arm difference >15 mmHg → investigate further
- Diagnose only after readings from ≥ 2 separate visits
🔲 INTERPRET & COMMUNICATE
- Share result with patient immediately
| Category | Systolic | Diastolic | |
|---|---|---|---|
| Normal | <120 | and | <80 |
| Elevated | 120-129 | and | <80 |
| Stage 1 HTN | 130-139 | or | 80-89 |
| Stage 2 HTN | ≥140 | or | ≥90 |
⚠️ COMMON ERRORS TO AVOID
| ❌ Error | Effect |
|---|---|
| Cuff over clothing | Falsely HIGH |
| Cuff too small | Falsely HIGH |
| Arm below heart level | Falsely HIGH |
| Back unsupported / legs crossed | Falsely HIGH |
| Patient talking | Falsely HIGH |
| Deflating too fast | Inaccurate both values |
🔲 SPECIAL CHECKS (when indicated)
Orthostatic BP:
- Measure after 5 min supine
- Repeat at 1 min and 3 min after standing
- Drop ≥20 mmHg systolic OR ≥10 mmHg diastolic = orthostatic hypotension
White-coat effect suspected:
- Consider automated unattended readings (patient alone in room)
- Refer for ABPM or home BP monitoring
Based on ACC/AHA guidelines and Harrison's Principles of Internal Medicine, 22nd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.