Explain me 10 common heart disease ECG changes illustrative ECGimage
Reading File
Finding Sources
Searching the Web
ECG changes 10 common heart diseases STEMI atrial fibrillation heart block illustrative
Finding Sources
Searching the Web
STEMI ECG ST elevation myocardial infarction classic ECG image site:ecgwaves.com OR site:litfl.com
Finding Sources
Searching the Web
atrial fibrillation heart block LVH LBBB Wolff Parkinson White ECG example images litfl
Finding Sources
Searching the Web
complete heart block third degree ECG ventricular tachycardia pericarditis ECG image examples
Finding Sources
Searching the Web
Brugada syndrome hypertrophic cardiomyopathy long QT syndrome ECG image examples litfl site:litfl.com
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have excellent ECG images and comprehensive information to deliver a detailed, well-illustrated answer. Here is the full guide:
10 Common Heart Disease ECG Changes - Illustrated Guide
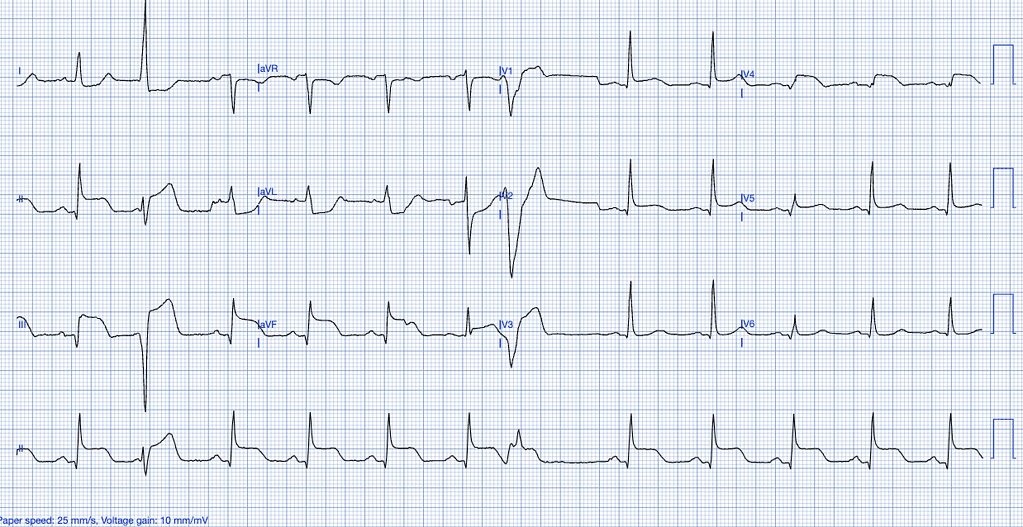
1. ST-Elevation Myocardial Infarction (STEMI)
Mechanism: Complete occlusion of a coronary artery causes transmural ischemia, producing ST-segment elevation in leads overlying the infarcted territory, with reciprocal ST depression in opposite leads. Q waves develop within hours as tissue necrosis occurs.
ECG Features:
- ST elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in V2-V3
- Reciprocal ST depression in mirror-image leads
- Hyperacute (peaked, broad) T waves early on
- Pathological Q waves (>40 ms wide, >25% of R-wave height) develop later
- T-wave inversion in the recovery phase
Localization:
| Territory | Leads with ST Elevation | Artery |
|---|---|---|
| Anterior | V1-V4 | LAD |
| Inferior | II, III, aVF | RCA |
| Lateral | I, aVL, V5-V6 | LCx |
| Posterior | ST depression V1-V3 (mirror) | RCA/LCx |
2. Atrial Fibrillation (AF)
Mechanism: Chaotic, rapid electrical impulses from multiple re-entrant circuits in the atria (often originating from pulmonary vein sleeves) replace organized atrial depolarization. The AV node conducts irregularly, producing an irregularly irregular ventricular response.
ECG Features:
- Absent P waves - replaced by fibrillatory (f) baseline (fine or coarse)
- Irregularly irregular RR intervals - the hallmark finding
- Narrow QRS complexes (unless aberrant conduction/LBBB)
- Ventricular rate typically 100-160 bpm if uncontrolled
- No distinct isoelectric baseline between complexes
Causes: Hypertension, ischemic heart disease, valvular disease (especially mitral), hyperthyroidism, alcohol, cardiomyopathy, sleep apnea
3. Left Bundle Branch Block (LBBB)
Mechanism: Block in the left bundle branch forces ventricular depolarization to travel right-to-left in an abnormally slow, cell-to-cell manner (not via the specialized conduction system), producing a broad, abnormally shaped QRS.
ECG Features (use the WiLLiaM pattern):
- QRS duration >120 ms (broad complex)
- Lead V1: broad, deep QS or rS complex ("W" shape)
- Lead V6/I/aVL: broad, notched or M-shaped R wave ("M" shape) - no septal Q waves
- ST depression and T-wave inversion in lateral leads (I, aVL, V5-V6) - these are "appropriate discordant" changes
- Left axis deviation may be present
Clinical significance: New LBBB with chest pain was historically treated as STEMI-equivalent. Sgarbossa criteria help identify true occlusion MI in setting of LBBB.
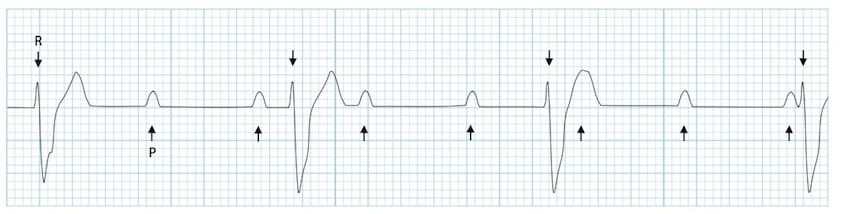
4. Complete (3rd Degree) AV Heart Block
Mechanism: Complete failure of conduction between atria and ventricles. The atria fire independently from the SA node; the ventricles are driven by a slow escape rhythm from the AV junction or ventricles. There is total AV dissociation.
ECG Features:
- P waves present at normal rate (~60-100 bpm) - but no P wave conducts to ventricles
- QRS complexes present at much slower escape rate (40-60 bpm for junctional; 20-40 bpm for ventricular)
- P waves and QRS complexes are completely independent of each other ("march through" each other)
- QRS may be narrow (junctional escape) or wide/bizarre (ventricular escape)
- No consistent PR interval
Causes: Inferior MI (usually reversible), anterior MI, Lyme disease, drugs (digoxin, beta-blockers, calcium channel blockers), infiltrative disease (sarcoid, amyloid)
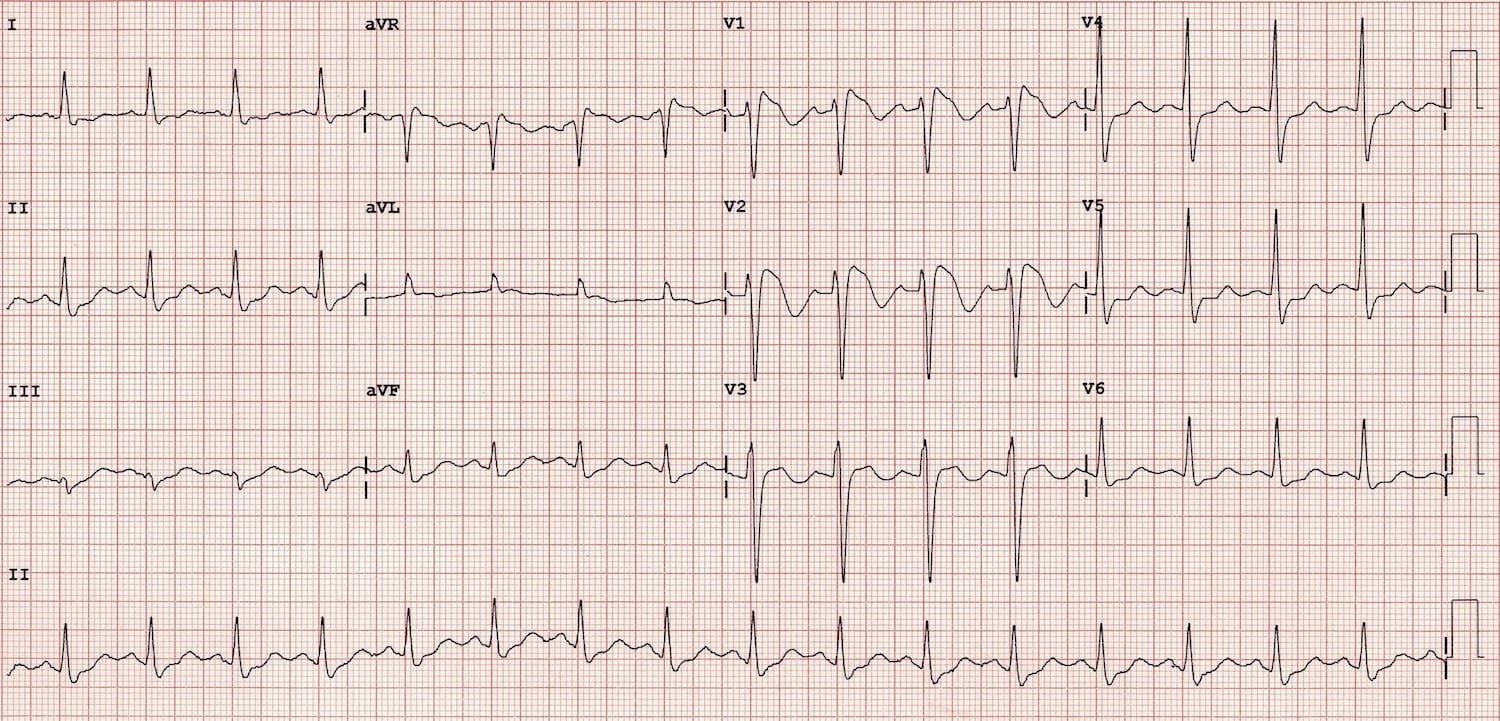
5. Left Ventricular Hypertrophy (LVH)
Mechanism: Increased myocardial mass from chronic pressure overload (hypertension, aortic stenosis) produces larger electrical vectors, causing increased QRS voltages. The thickened wall also repolarizes abnormally.
ECG Features (multiple criteria exist; Sokolow-Lyon most used):
- Sokolow-Lyon: S in V1 + R in V5 or V6 ≥35 mm
- Cornell: R in aVL + S in V3 ≥28 mm (men), ≥20 mm (women)
- Left axis deviation
- ST depression with asymmetric T-wave inversion in lateral leads (I, aVL, V5-V6) - "strain pattern"
- Prolonged QRS (~100-120 ms, but <120 ms)
- Left atrial enlargement (broad notched P waves, P mitrale)
Causes: Hypertension (most common), aortic stenosis, hypertrophic cardiomyopathy, coarctation of aorta
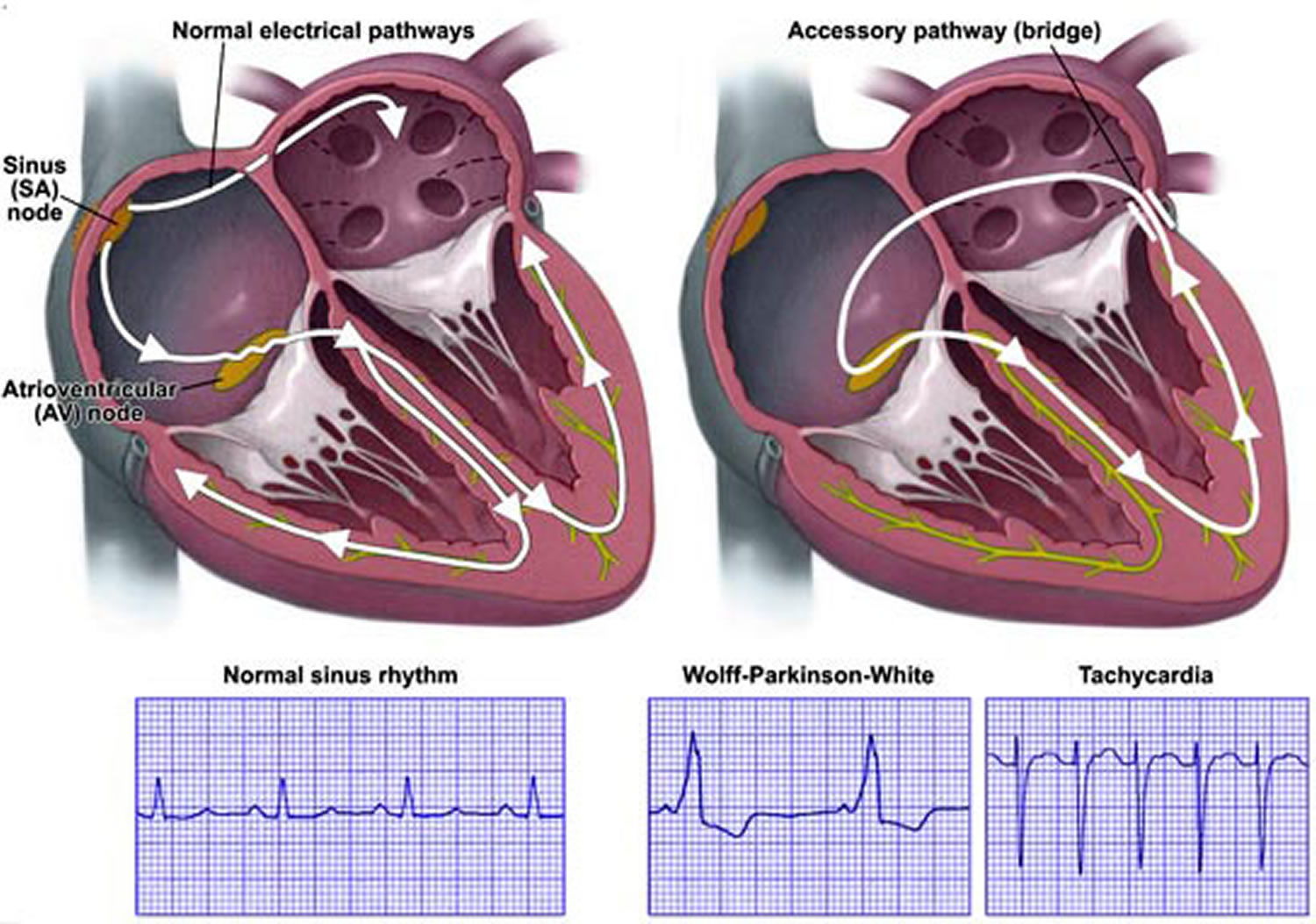
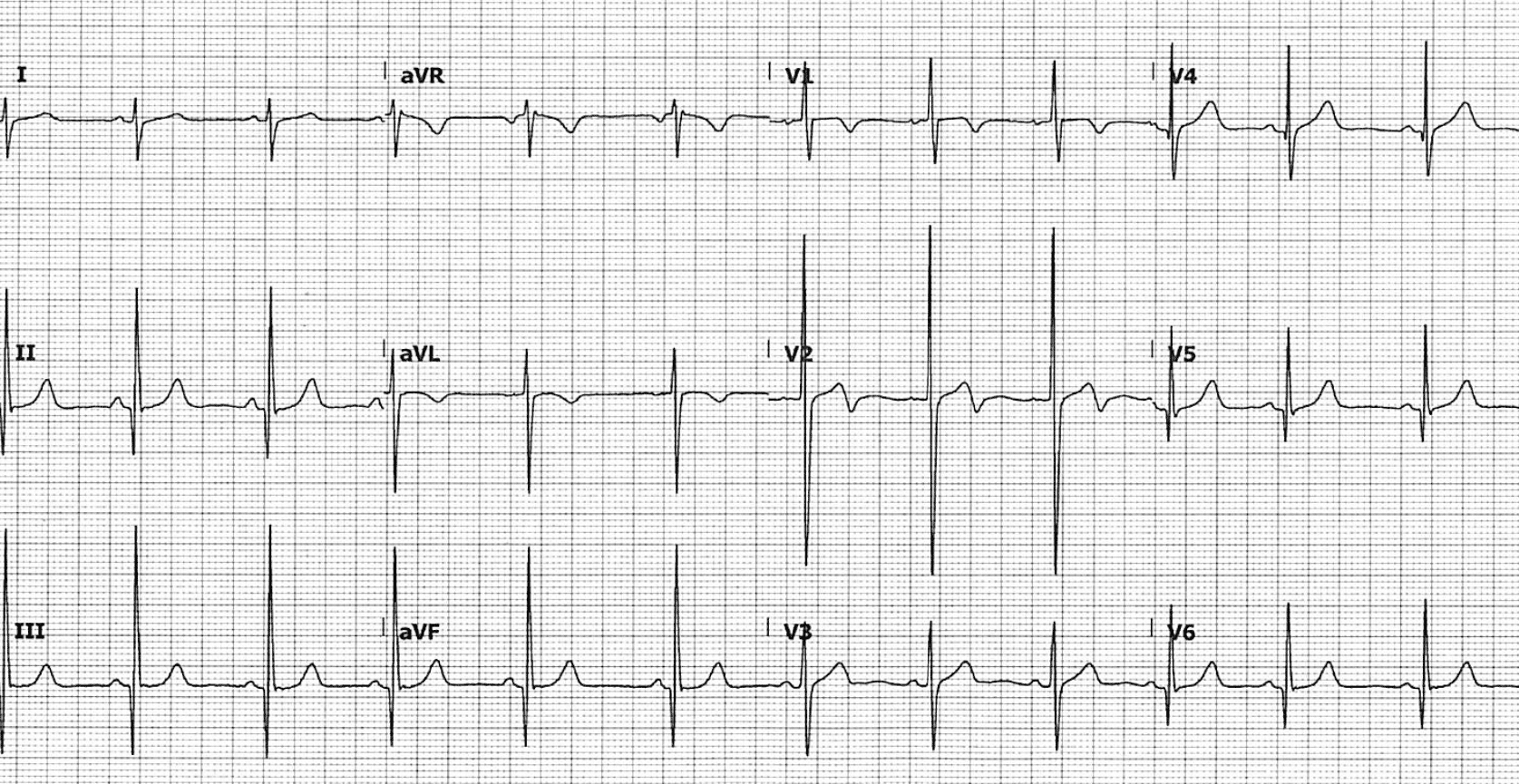
6. Wolff-Parkinson-White Syndrome (WPW)
Mechanism: A congenital accessory pathway (Bundle of Kent) bypasses the AV node, pre-exciting part of the ventricle before the normal conduction system depolarizes it. This creates the characteristic delta wave and short PR interval.
ECG Features:
- Short PR interval (<120 ms)
- Delta wave - slurred upstroke at the start of the QRS (ventricular pre-excitation)
- Broad QRS (>120 ms) due to fusion of pre-excited and normally conducted depolarization
- Secondary ST-T changes (discordant to QRS)
- Risk: AF with WPW is life-threatening - rapid conduction via the accessory pathway can cause VF
| WPW Type | V1 morphology | Accessory Pathway location |
|---|---|---|
| Type A | Dominant R wave V1 | Left-sided pathway |
| Type B | QS or rS in V1 | Right-sided pathway |
7. Ventricular Tachycardia (VT)
Mechanism: Rapid rhythm originating from ventricular myocardium (below the bundle of His), usually via re-entry around a scar from prior MI. Since conduction is cell-to-cell rather than via the His-Purkinje system, QRS complexes are broad and bizarre.
ECG Features:
- Rate: 100-250 bpm
- Broad QRS ≥120 ms, often ≥160 ms, with bizarre morphology
- AV dissociation - P waves independent of QRS (when visible, pathognomonic for VT)
- Fusion beats - QRS morphology partway between normal and VT (P wave conducts during VT)
- Capture beats - occasional narrow normal QRS during VT (P wave fully captures ventricles)
- Concordance in precordial leads (all positive or all negative V1-V6)
- Northwest axis (negative in I and aVF)
Brugada criteria help differentiate VT from SVT with aberrancy.

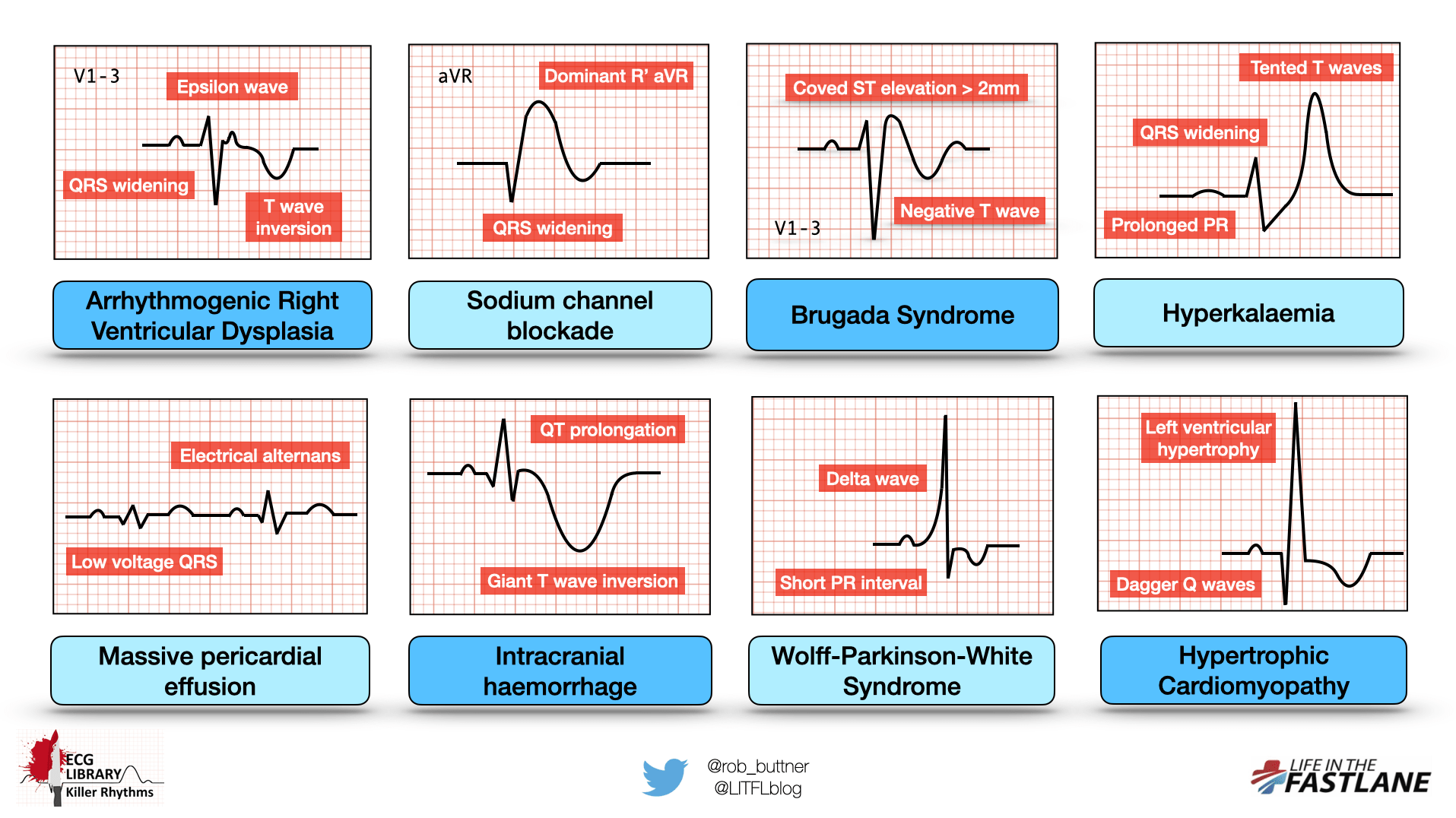
8. Hypertrophic Cardiomyopathy (HCM)
Mechanism: Asymmetric septal hypertrophy with myofibrillar disarray causes abnormal depolarization vectors, prominent septal forces, and impaired diastolic relaxation. ECG findings reflect massive left ventricular hypertrophy plus septal abnormalities.
ECG Features:
- LVH voltage criteria (usually extreme)
- "Dagger" Q waves - deep, narrow Q waves in lateral (I, aVL, V5-V6) and/or inferior leads - due to septal hypertrophy, NOT infarction
- ST depression and T-wave inversion in lateral leads
- Left axis deviation
- Giant negative T waves in mid-precordial leads (apical variant HCM - Yamaguchi)
- P-wave abnormalities (left atrial enlargement)
- 5% of HCM patients have a normal ECG
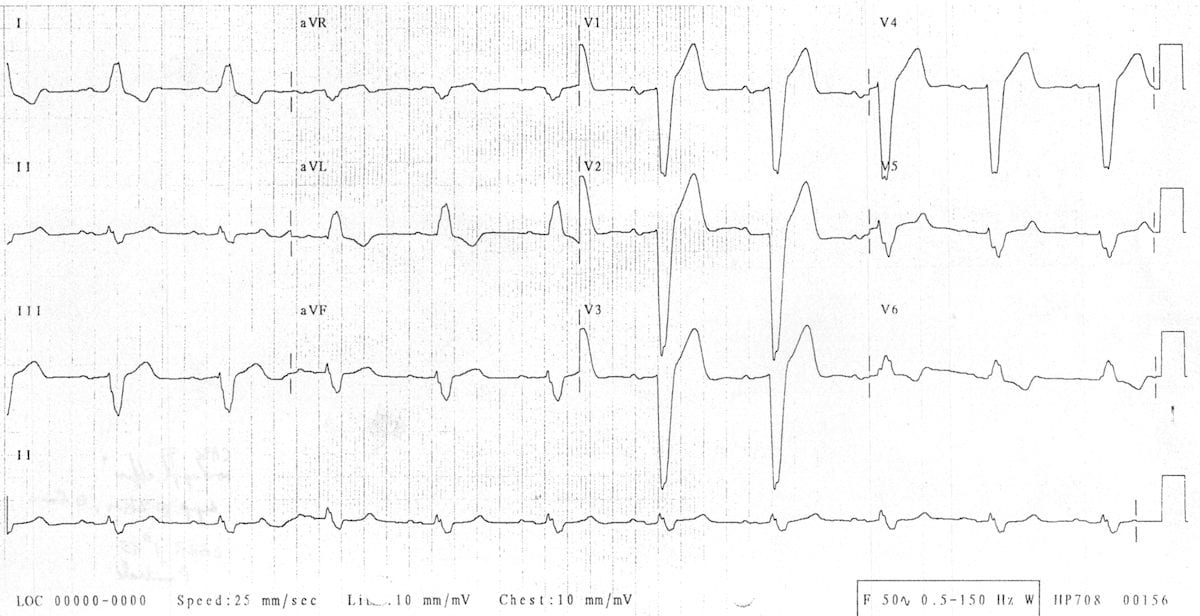
9. Brugada Syndrome
Mechanism: Loss-of-function mutation in sodium channels (SCN5A gene, ~30% of cases) causes abnormal repolarization predominantly in the right ventricular outflow tract (RVOT), creating a characteristic ST pattern in V1-V3 and predisposing to polymorphic VT and sudden cardiac death.
ECG Features (3 types, only Type 1 is diagnostic):
| Type | V1-V2 pattern | Diagnostic? |
|---|---|---|
| Type 1 | Coved ST elevation ≥2 mm + negative T wave | YES - Diagnostic |
| Type 2 | Saddleback ST elevation ≥2 mm + positive/biphasic T wave | No (screen positive) |
| Type 3 | ST elevation <1 mm | No |
- RBBB-like pattern in V1-V2
- Pattern may be intermittent ("concealed Brugada")
- Sodium channel blockers (ajmaline, flecainide) can unmask concealed Brugada
Clinical: Predominantly young males, Asian descent; causes sudden death especially at night/rest during fever.
10. Acute Pericarditis
Mechanism: Diffuse inflammation of the pericardium causes widespread myocardial irritation affecting repolarization globally (not in a vascular territory), producing the characteristic pattern of widespread concave ST elevation with PR depression.
ECG Features (4 stages):
| Stage | ECG Changes | Timing |
|---|---|---|
| Stage I | Diffuse concave ("saddle-back") ST elevation + PR depression in most leads; ST depression + PR elevation in aVR/V1 | Days 1-2 (acute) |
| Stage II | ST and PR return to baseline, T waves flatten | Days 3-7 |
| Stage III | Diffuse T-wave inversion | Weeks 1-3 |
| Stage IV | ECG normalizes | Weeks to months |
Key differentiators from STEMI:
- ST elevation is concave (saddle-shaped), not convex/tombstone
- Widespread in multiple vascular territories (not anatomically contiguous)
- PR segment depression - highly specific for pericarditis
- No reciprocal ST depression (except aVR)
- No Q waves
Causes: Viral (Coxsackievirus), idiopathic, post-MI (Dressler syndrome), autoimmune, uremic, neoplastic
Quick Summary Reference
Summary Table
| Condition | Key ECG Finding | Pathological Structure |
|---|---|---|
| STEMI | Convex ST elevation + Q waves (regional) | Occluded coronary artery |
| Atrial Fibrillation | Absent P waves + irregularly irregular QRS | Chaotic atrial foci |
| LBBB | Broad QRS, WiLLiaM pattern, no septal Q waves | Left conduction system failure |
| 3rd Degree AV Block | Complete P-QRS dissociation | AV node/His bundle block |
| LVH | Tall voltages + strain pattern | Thickened LV wall |
| WPW | Short PR + delta wave + broad QRS | Accessory pathway (Bundle of Kent) |
| Ventricular Tachycardia | Broad complex tachycardia + AV dissociation | Ventricular re-entry circuit |
| HCM | LVH + dagger Q waves | Asymmetric septal hypertrophy |
| Brugada Syndrome | Coved ST elevation V1-V2 + RBBB pattern | SCN5A sodium channel mutation |
| Acute Pericarditis | Concave ST elevation (all leads) + PR depression | Diffuse pericardial inflammation |
Sources: Harrison's Principles of Internal Medicine 22E; Tintinalli's Emergency Medicine; Ganong's Review of Medical Physiology; LITFL ECG Library; ECGwaves.com; REBEL EM
This is a shared conversation. Sign in to Orris to start your own chat.