Stomach surgical procedure
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching the Web
Roux-en-Y gastric bypass surgical procedure steps indications complications 2025
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from the Sabiston Textbook of Surgery and Current Surgical Therapy 14e to give a thorough answer.
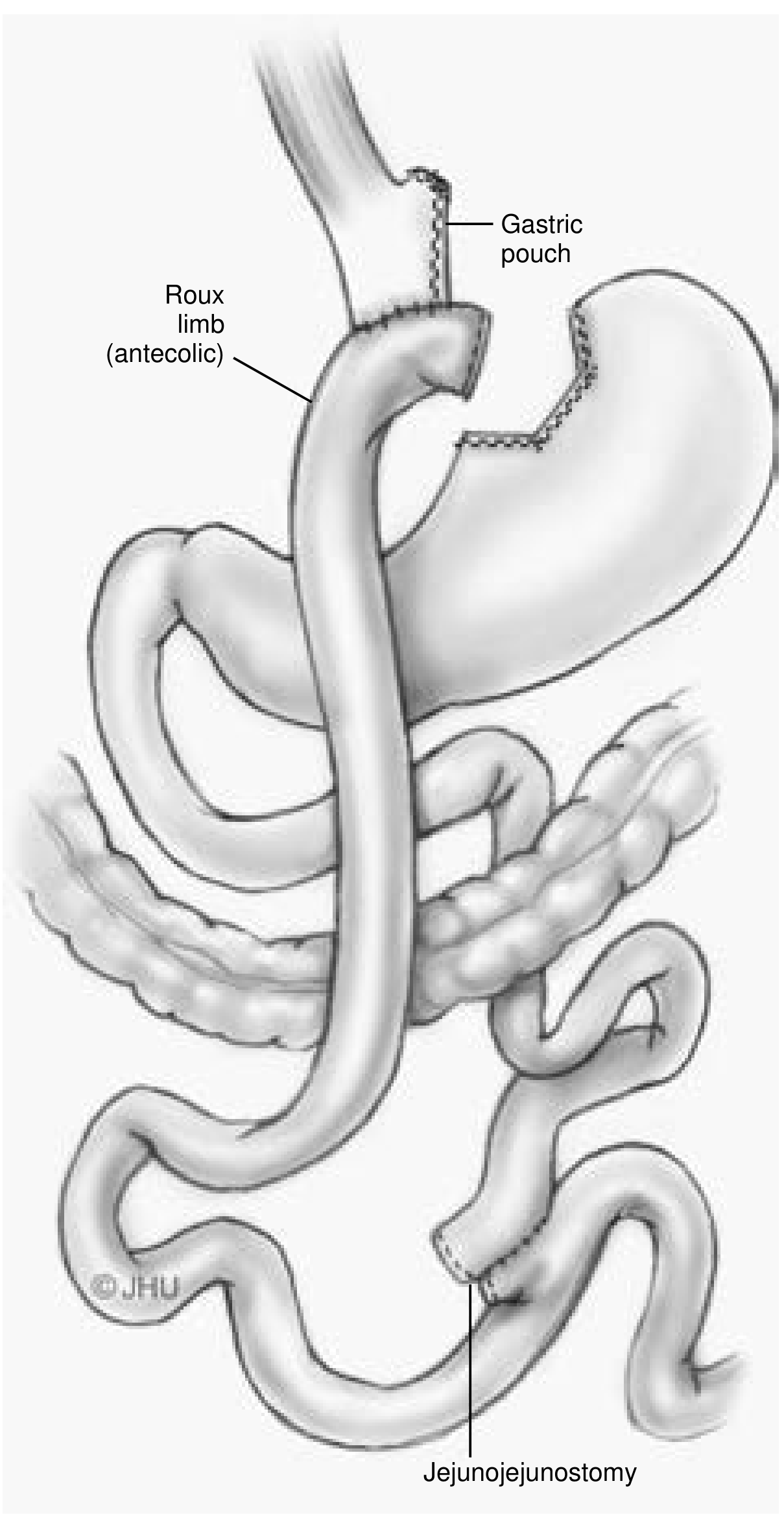
Gastric Bypass (Roux-en-Y Gastric Bypass - RYGB)
Overview
Roux-en-Y Gastric Bypass (RYGB) is currently the second most common bariatric procedure in the United States (~20% of all bariatric cases), and the gold standard for metabolic outcomes. It achieves weight loss through three mechanisms:
- Gastric restriction (small pouch limits food intake)
- Mild malabsorption (bypassing the duodenum and proximal jejunum)
- Profound gut hormone changes that increase satiety and suppress hunger (GLP-1, PYY)
Indications (Box I - Current Surgical Therapy 14e)
| Criterion | Details |
|---|---|
| BMI ≥ 40 kg/m² | No comorbidities required |
| BMI 35-39.9 kg/m² | With significant obesity comorbidities (diabetes, hypertension) |
| BMI 30-35 kg/m² | With comorbidities, failed non-surgical treatment (per ASMBS guidelines) |
| Required clearances | Dietitian + mental health professional evaluation |
| No contraindications | No medical, psychiatric, or compliance barriers |
Relative contraindications include: inability to comply with postoperative requirements, active alcohol/substance abuse, uncontrolled psychiatric illness.
Surgical Technique (Step-by-Step)
All steps are performed laparoscopically (or robot-assisted), with the patient in reverse Trendelenburg position. Five trocars are used. Hospital stay is typically 1 day or less.
Step 1: Jejunojejunostomy (Roux Limb Creation)
- Identify the ligament of Treitz
- Transect the jejunum 40-75 cm distal to the ligament of Treitz using a 60-mm white stapler
- Divide the mesentery with a gray stapler or ultrasonic shears
- Create a side-to-side jejunojejunostomy 75-100 cm distal from the transection point using a 60-mm white laparoscopic stapler - this forms the "Y" connection
- Close the mesenteric defect with running suture to prevent internal hernia
Step 2: Gastric Pouch Creation
- Retract the left lateral liver segment with a Nathanson retractor
- Dissect peritoneal attachments at the angle of His, expose the left crus
- Open the gastrohepatic ligament (lesser sac access)
- Divide the neurovascular bundle on the lesser curve just distal to the left gastric artery
- Use multiple 60-mm blue staple cartridges to transect the stomach superiorly, creating a vertically oriented ~20 mL proximal gastric pouch
- A 40Fr bougie guides the staple line along the lesser curve up to the angle of His
Step 3: Gastrojejunostomy
- Bring the Roux limb antecolic-antegastric to the gastric pouch (preferred over retrocolic - reduces internal hernia risk)
- Suture the side of the Roux limb to the gastric pouch staple line
- Create a small enterotomy and gastrotomy, then fire a 60-mm blue stapler (using only 40 mm) to form the gastrojejunostomy
- A 32Fr bougie calibrates the anastomosis to prevent stricture
- Close the common enterotomy with a 60-mm blue stapler
- Leak test the anastomosis
Step 4: Closure
- Close trocar sites and skin
- Routine DVT prophylaxis (subcutaneous LMWH, SCDs) and antibiotics are given pre/perioperatively
Outcomes
From randomized trials (SLEEVEPASS, SM-BOSS, STAMPEDE) comparing LRYGB vs Laparoscopic Sleeve Gastrectomy (LSG):
| Outcome | LRYGB | LSG |
|---|---|---|
| Excess weight loss at 5 years | ~57% | ~49% |
| Type 2 diabetes remission | 25-68% | 12-62% |
| Hypertension remission | 51-70% | 29-63% |
| LDL cholesterol | Lower | Higher |
| GERD remission | ~60% | ~25% |
| Mortality | 0.1-0.3% | Similar |
RYGB is superior for GERD, LDL reduction, and weight loss; LSG has a slightly safer complication profile. - Sabiston Textbook of Surgery, p. 2215
Complications
Early (< 30 days)
- Anastomotic leak (< 1% with laparoscopic technique) - presents with tachycardia, tachypnea, abdominal pain; treated with sepsis control, often operative management
- Hemorrhage (~1-1.6%) - from staple lines
- Pulmonary embolism/DVT (~0.23% with modern prophylaxis) - accounts for 17% of deaths
- Wound infection (~0.8-0.9%)
Late (> 30 days)
- Anastomotic stenosis (2-7%) - progressive food intolerance at 4-6 weeks; treated with endoscopic balloon dilation
- Marginal ulcer (2-14%) - epigastric pain; treated with PPIs; related to larger pouch, H. pylori, NSAIDs, smoking
- Internal hernia (0.9-4.5%) - can cause small bowel obstruction and requires urgent reoperation; mesenteric defect closure at time of surgery reduces incidence by ~70%
- Dumping syndrome - early (osmotic) or late (reactive hypoglycemia); requires dietary modification
- Wernicke's encephalopathy - from thiamine deficiency with persistent vomiting; treat with IV thiamine
Nutritional Deficiencies (Long-term)
- Iron deficiency (15-40%) - duodenum/proximal jejunum are bypassed; treat with oral iron gluconate
- Vitamin B12 deficiency (15-20%) - intrinsic factor loss and bypass of ileal absorption; supplement with B12
- Also: Vitamin D, calcium, folate, zinc deficiencies require lifelong supplementation
Key Anatomy of RYGB (3 limbs)
- Biliopancreatic (hepatobiliary) limb - from duodenum to jejunojejunostomy; carries bile and pancreatic enzymes; NOT connected to food
- Alimentary (Roux) limb - from gastric pouch to jejunojejunostomy; 75-100 cm; carries food
- Common limb - distal to the "Y" junction; both food and digestive juices mix here
Sources: Current Surgical Therapy 14e, pp. 163-170; Sabiston Textbook of Surgery, pp. 2215-2217; ACS 2025 systematic review on long-term RYGB vs sleeve gastrectomy outcomes confirms RYGB superiority for sustained weight loss and metabolic control.
This is a shared conversation. Sign in to Orris to start your own chat.