Explain most common heart diseases with ecg findings
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
ECG findings myocardial infarction ST elevation
Reading File
Searching Images
atrial fibrillation ECG irregularly irregular rhythm absent P waves
Searching Images
hypertrophic cardiomyopathy ECG left ventricular hypertrophy deep S waves
Searching Images
pericarditis ECG diffuse ST elevation PR depression saddle shaped
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain pattern
Searching Images
complete heart block third degree AV block ECG dissociation
I now have rich content from multiple authoritative textbooks and ECG images. Let me compile the comprehensive answer.
Common Heart Diseases and Their ECG Findings
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery → transmural ischemia/infarction.
ECG Findings:
| Finding | Detail |
|---|---|
| ST elevation | >1 mm in ≥2 contiguous leads |
| Q waves | Pathological Q waves (>0.04 s duration) — develop within hours |
| T-wave changes | Hyperacute peaked T-waves early; T-wave inversion in evolution |
| New LBBB | Equivalent to STEMI — treat as occlusion |
| Reciprocal depression | ST depression in leads opposite to injury zone (marks larger territory, higher mortality) |
Localization by lead group (Tintinalli's Emergency Medicine):
| Territory | Leads with ST elevation | Culprit artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Inferior | II, III, aVF | RCA (ST III > II) or LCx (ST III < II) |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | ST depression V1–V3 (mirror image) → posterior leads V8–V9 | RCA/LCx |
| RV infarction | ST elevation in V4R | Proximal RCA |
"Elevation of aVR > V1 suggests left anterior descending artery occlusion." — Tintinalli's Emergency Medicine
Anterior STEMI (LAD occlusion):

Inferior STEMI (RCA occlusion) with reciprocal changes:
2. Non-ST-Elevation MI (NSTEMI) / Unstable Angina
Pathophysiology: Partial occlusion / subendocardial ischemia — no full-thickness injury.
ECG Findings:
| Condition | ECG |
|---|---|
| NSTEMI | ST depression ≥1 mm in concordant leads; T-wave inversion |
| Unstable Angina | Most often normal or nonspecific; may have T-wave inversion |
"Subendocardial infarction: T wave inversion or ST segment depression in concordant leads." — Rosen's Emergency Medicine
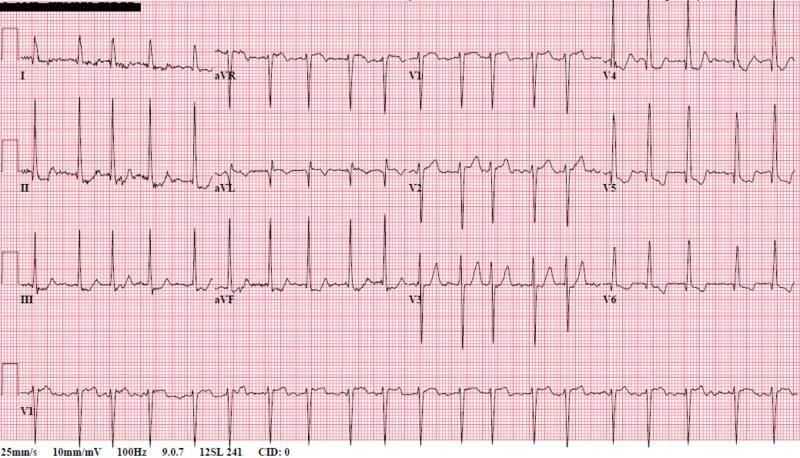
3. Atrial Fibrillation (AF)
Pathophysiology: Chaotic atrial electrical activity at 350–600 impulses/min; AV node conducts irregularly.
ECG Findings:
- Absent P waves — replaced by irregular fibrillatory baseline (f-waves), best seen in V1
- Irregularly irregular R-R intervals (no pattern to QRS timing)
- Narrow QRS (unless aberrant conduction or pre-excitation)
- Ventricular rate variable: slow (if treated/AV block) to rapid (>100 bpm = AF with RVR)
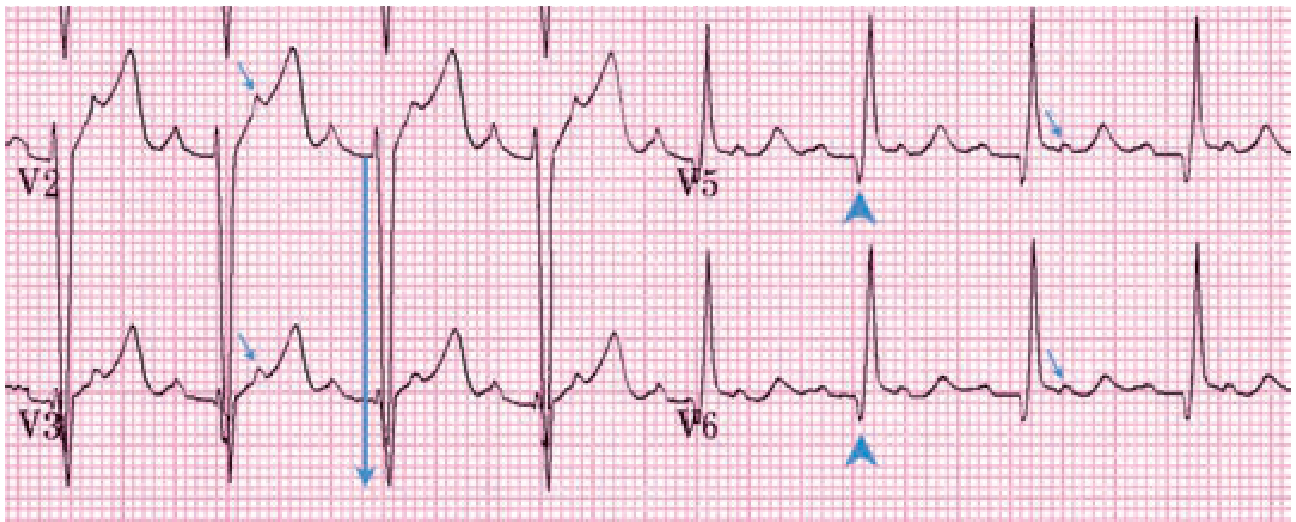
4. Hypertrophic Cardiomyopathy (HCM)
Pathophysiology: Asymmetric septal hypertrophy → LV outflow obstruction, diastolic dysfunction, arrhythmia risk.
ECG Findings (Tintinalli's Emergency Medicine):
- LV hypertrophy — deep S waves (V2–V3 ≥ 28 mm), tall R waves lateral leads
- Left atrial enlargement — broad notched P wave in lead II, biphasic P in V1
- Septal Q waves — narrow, deep Q waves in I, aVL, V4–V6 (≥0.3 mV) — pseudoinfarction pattern
- T waves upright in leads with septal Q waves (distinguishes from ischemic Q waves where T waves are inverted)
- Giant T-wave inversions in apical HCM (Yamaguchi syndrome) — deep symmetric inversions V3–V6
- Arrhythmias: AF, atrial flutter, VT

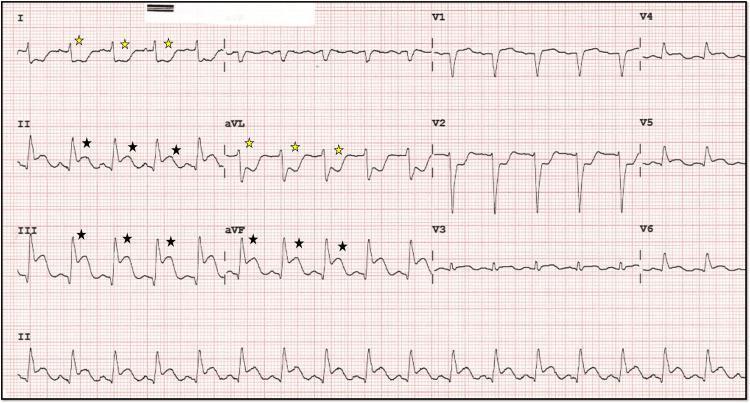
5. Pericarditis
Pathophysiology: Pericardial inflammation → diffuse epicardial irritation (subepicardial current of injury in all leads).
ECG Findings (4 classic stages):
| Stage | Finding |
|---|---|
| Stage 1 | Diffuse concave ("saddle-shaped") ST elevation in all leads except aVR (ST depression) and V1; PR segment depression in most leads; PR elevation in aVR |
| Stage 2 | ST segments normalize; T waves flatten |
| Stage 3 | Diffuse T-wave inversion |
| Stage 4 | ECG returns to normal |
Key distinguishing features from STEMI:
- ST elevation is diffuse (all territories), not localized to one artery
- Concave (saddle-shaped), not convex morphology
- PR depression present
- No reciprocal changes (except aVR)
- No pathological Q waves
"Pericarditis: diffuse ST segment elevation; PR segment depression." — Rosen's Emergency Medicine
Spodick's sign: Downsloping TP segment (highly specific for pericarditis).

6. Heart Failure / Left Ventricular Hypertrophy
Pathophysiology: Chronic pressure/volume overload → LV remodeling, hypertrophy.
ECG Findings:
- Sokolow-Lyon criteria for LVH: S in V1 + R in V5 or V6 > 35 mm
- "Strain" pattern: ST depression and T-wave inversion in lateral leads (I, aVL, V5–V6)
- Left axis deviation
- Left atrial enlargement (bifid P wave in II, biphasic in V1)
- Left bundle branch block (LBBB) — common in dilated cardiomyopathy/HF
- Non-specific ST-T changes
"The resting ECG may reveal various conduction disturbances, most frequently left bundle branch block and left anterior fascicular block." — Goldman-Cecil Medicine
7. Pulmonary Embolism (PE)
Pathophysiology: Acute RV pressure overload from pulmonary artery obstruction → RV strain pattern.
ECG Findings (Tintinalli's Emergency Medicine, Fuster and Hurst's The Heart):
- Sinus tachycardia — most common finding (HR >100)
- S1Q3T3 pattern — S wave in lead I, Q wave in lead III, T-wave inversion in lead III (McGinn-White sign)
- T-wave inversion V1–V4 — right precordial ischemia from RV strain
- Incomplete or complete RBBB
- Right axis deviation
- "P pulmonale" — tall peaked P wave in lead II (≥2.5 mm) from right atrial enlargement
- ECG may be entirely normal in ~30% of cases
"Findings of acute pulmonary hypertension on ECG include a heart rate >100 beats/min, T-wave inversion in leads V1 to V4, incomplete or complete right bundle branch block, and the S1-Q3-T3 pattern." — Tintinalli's Emergency Medicine

8. Complete (Third-Degree) AV Block
Pathophysiology: Total failure of AV conduction → atria and ventricles beat independently.
ECG Findings:
- P waves and QRS complexes completely dissociated — no relationship (P waves "march through" QRS/T waves)
- Regular P-P intervals at normal/faster atrial rate
- Regular R-R intervals at slow escape rate
- Escape rhythm:
- Junctional (AV nodal disease): narrow QRS, rate 40–60 bpm
- Ventricular (infra-Hisian): wide QRS >120 ms, rate 20–40 bpm
Causes: inferior MI (usually transient), Lyme disease, infiltrative disease, post-surgical.

9. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: Accessory pathway (Bundle of Kent) bypasses the AV node → ventricular pre-excitation.
ECG Findings:
- Short PR interval (<120 ms) — early ventricular activation
- Delta wave — slurred upstroke of QRS (pre-excitation)
- Wide QRS — fusion beat (delta + normal conduction)
- Discordant ST-T changes (secondary to abnormal depolarization)
- Can have pseudo-Q waves and ST changes mimicking MI
- Associated with orthodromic SVT (regular narrow complex tachycardia) and AF with rapid ventricular response (irregular, wide complex — dangerous)
10. Dilated Cardiomyopathy
Pathophysiology: Ventricular dilation + systolic dysfunction from various causes.
ECG Findings:
- LBBB — very common (reflects impaired conduction through dilated ventricle)
- LVH criteria — but voltage often low in the most dilated hearts
- Poor R-wave progression across precordial leads
- Non-specific ST-T changes
- AF and ventricular ectopy are frequent
Quick Reference Summary
| Disease | Key ECG Pattern |
|---|---|
| STEMI | ST elevation (contiguous leads), Q waves, new LBBB |
| NSTEMI | ST depression, T-wave inversion |
| Atrial Fibrillation | Absent P waves, irregularly irregular |
| HCM | LVH, narrow septal Q waves, upright T waves; giant TWI in apical type |
| Pericarditis | Diffuse saddle-shaped ST ↑, PR depression, no reciprocal changes |
| Heart Failure/LVH | LVH criteria, strain pattern, LBBB |
| Pulmonary Embolism | Tachycardia, S1Q3T3, RBBB, TWI V1–V4 |
| Complete Heart Block | AV dissociation, bradycardia, slow escape rhythm |
| WPW | Short PR, delta wave, wide QRS |
| Dilated Cardiomyopathy | LBBB, poor R-wave progression, arrhythmias |
Sources: Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E; Fuster and Hurst's The Heart, 15th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.